






INTRODUCTION
Masticatory function has been studied in several ways; 1.) assessing chewed particle size by optical scanning or sieving,1 with real or with artificial food,2 2.) calculating the Average Chewing Pattern of motion,3,4 3.) analyzing EMG muscle activity5 or 4.) by asking the patient if they have any difficulty when eating.6 A limitation of patient input is that he or she has no frame of reference as to what is good function. The other three methods can be either laborious, time consuming and/or provide incomplete results. However, a correlation has been found between the patient’s perception of chewing ability and his or her oral health-related quality of life (OHRQoL).7 Historically, the value of good masticatory function has been underestimated or completely ignored by dentistry, along with the deleterious effects of inadequate mastication upon the rest of the body.
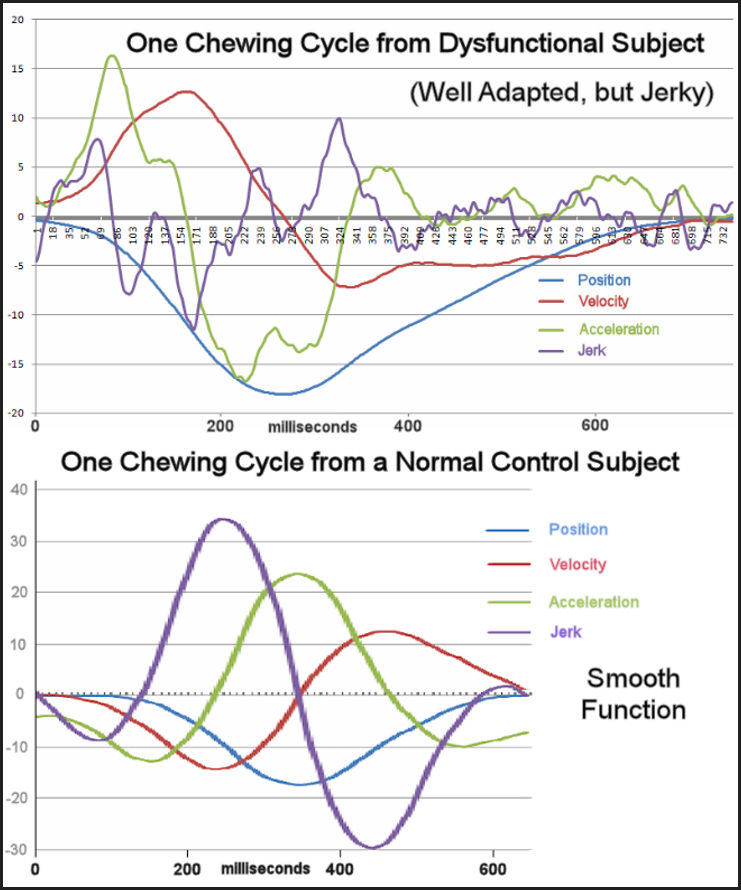
While particle size analysis can evaluate the efficiency of mastication, a poor result usually does not provide an indication of what needs to be corrected. The Average Chewing Pattern has been used to classify types of TMJ internal derangements4 and document obvious malocclusions.8,9 Another factor that has been separately extracted from masticatory motion is the smoothness of function. Smoothness is assessed from the Jerk function, the third derivative of motion, the rate of change of acceleration.10 Jerkiness, the opposite of smoothness, is present when acceleration and deceleration alternate extensively. A simple way to measure jerkiness is to simply count the average number of transitions per cycle, (the inflection points), between acceleration and deceleration that occur within a chewing sequence. The smallest number of possible inflection points per cycle is four, two during opening (one acceleration and one deceleration) and likewise two during closing. Normal asymptomatic subjects average about 3.4 transitions during opening and 3.2 during closing, but dysfunctional subjects often exhibit many more.
Asymptomatic control subjects with good occlusions chew at a certain rate (from 1.3 to 2 cycles/second) and with greater consistency. Patients with masticatory dysfunction as a group, chew more slowly, with more variability and with smaller movement patterns.11,12 See Figure 1.
_is_compared_to_a_dysfunctional_(tmd)_group_(n___38).jpg)
Of course, every individual is unique and a well-adapted patient with some type of dysfunction can still function more effectively than one who has the same dysfunction, but is poorly adapted. A huge advantage of recording the motion of chewing is that segmenting the timing into individual cycles and separating the opening movement from the closing movement is very straightforward. However, it is the musculature that moves the mandible and nearly normal movements are sometimes present with a struggling musculature in the dysfunctional patient. Thus, it is necessary to simultaneously record both the movement and the muscle activity to fully understand the quality of masticatory function.
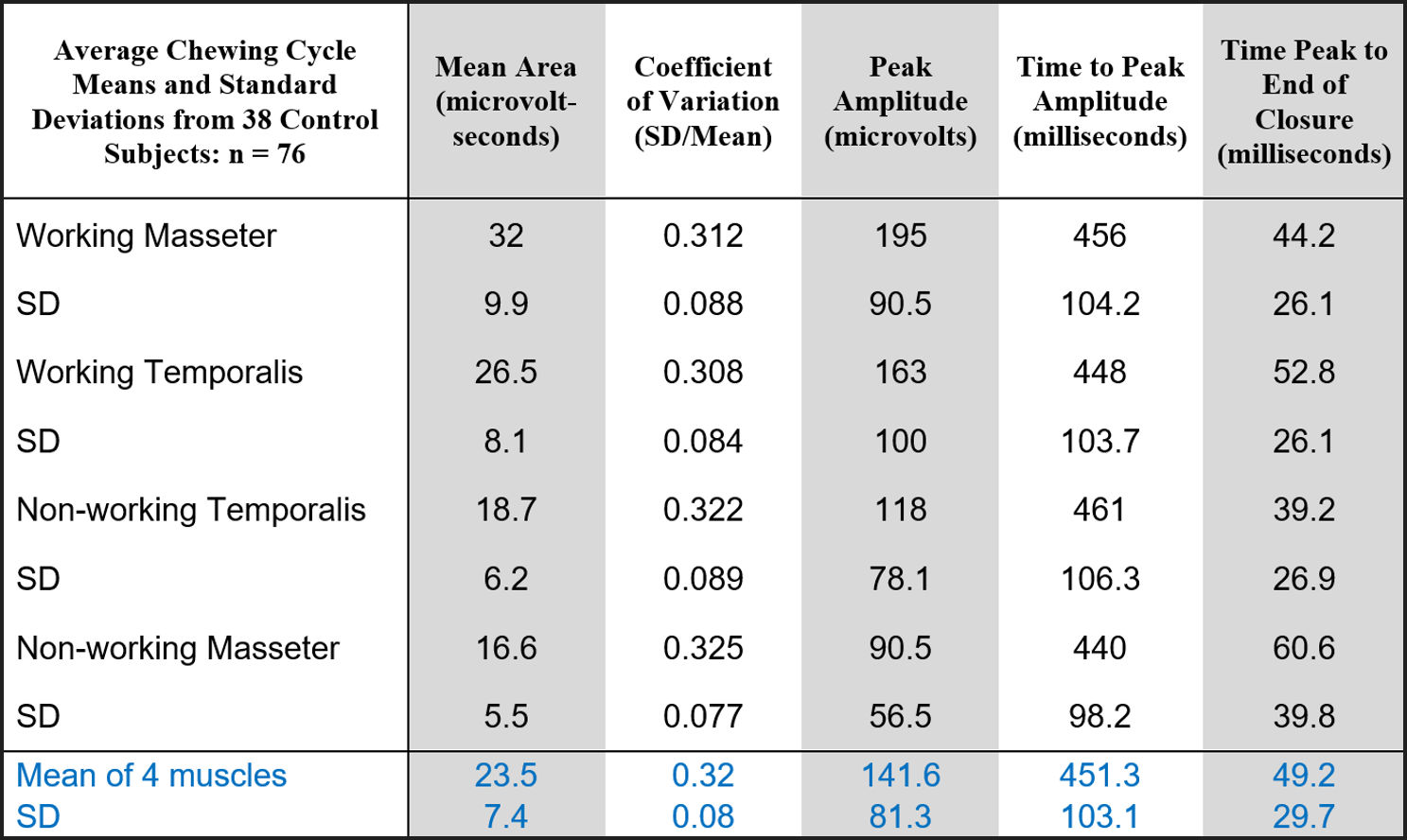
Asymptomatic control subjects with good occlusions exhibit a consistent pattern of muscle activity. The hierarchy of the intensity of the activity is; 1) the working masseter is the most active, 2) followed by the working temporalis, 3) followed by the non-working temporalis and 4) followed by the least active non-working masseter muscle. See Figure 2.

The variability can be observed by calculating the Coefficient of Variation (SD/Mean), which falls near 0.32 within normal groups. The Peak Amplitude follows the same hierarchical pattern. The time from the onset of opening to the Peak Amplitude of the activity is similar for all muscles, but the non-working masseter most often reaches its peak first and the working temporalis last. The time from the Peak Amplitude to the End of Closure is an indication of the confidence of the subject. Positive values indicate the peak occurred confidently during bolus crush before the End of Closure, but negative values indicate the Peak Amplitude occurred after the End of Closure. Late peaking indicates a lack of confidence and is associated with masticatory dysfunction.
An important factor that affects the ability of the patient to masticate is the stability of the occlusion. A stable occlusion allows the patient to function smoothly, rapidly, forcefully and efficiently with short bursts of muscle activity.13 Occlusal interferences are often avoided to the extent that the Central Nervous System (CNS) is able to do so, but unavoidable occlusal interferences hyperactivate the muscles that are attempting to avoid them. Electromyography (EMG) can be used to identify the presence of unavoidable occlusal interferences by detecting exteroceptive suppression (Silent Periods) occurring during gum chewing.14 See Figure 3. When the presence of silent periods has been identified, occlusal interferences can be most accurately located and removed by using the T-Scan (Tekscan, Inc. South Boston, USA).15,16
_occurring_repeatedly_throughout_a_gum_chewing_s.jpeg)
Patients in need of prosthodontic services often do not have good masticatory functional capacity due to missing teeth and/or compromised occlusions. A lack of good masticatory function can contribute to gastrointestinal dysfunction (e. g. irritable bowel syndrome,17,18 Gastroesophageal Reflux Disease19,20 (GERD), etc.). Note: Although more research has been focused on the loss of tooth enamel due to GERD, the loss of the ability to masticate effectively can contribute to the development of GERD. Restoration of the teeth is often necessary for restoring masticatory function, but just replacing missing teeth does not guarantee ideal correction of masticatory function. However, it is possible today to evaluate the results of dental restorations in terms of its effects on masticatory function.
OBJECTIVE
The objective of this study was to compare the overall masticatory function of prosthodontic patients prior to and subsequent to fixed restorative treatment. The purpose was to elucidate some objectively measurable, statistically significant changes in masticatory function that could be identified after any fixed restorative prosthodontic treatment, not limited to the particular treatment procedure.
METHODS
A standard medical history and clinical examination were conducted to determine the status and eligibility of presenting patients seeking prosthodontic treatments according to the following criteria;
-
Inclusion Criteria: Good general health, a need for prosthodontic treatment, a willingness to participate, a signed informed consent
-
Exclusion Criteria: Patients with systemic diseases, the presence of identified temporomandibular disorders, inability to chew gum or hard bolus prior to treatment, potential subjects with facial hair preventing surface EMG recording of the masseter and temporalis muscles.
The thirty prospective patients were selected from a continuous series of patients seeking prosthodontic treatments, who met all of the criteria. Mastication was recorded with a magnet-based JT-3D incisor-point tracker, a BioEMG III electromyograph and analyzed with the BioPAK version 8.80 computer program (BioResearch Associates, Inc. Milwaukee, WI USA). See Figure 4. Records were made prior to and subsequent to all of the restorative prosthodontic procedures.
A magnet was secured in the labial vestibule with a stomahesive material and EMG surface electrodes were placed bilaterally after cleansing the masseter and anterior temporalis areas with alcohol. See again Figure 4. The subjects were recorded chewing gum first and then given a tough bolus (Chikki, a peanut-based candy) and directed to masticate alternately on their left and right sides for at least 20 cycles.
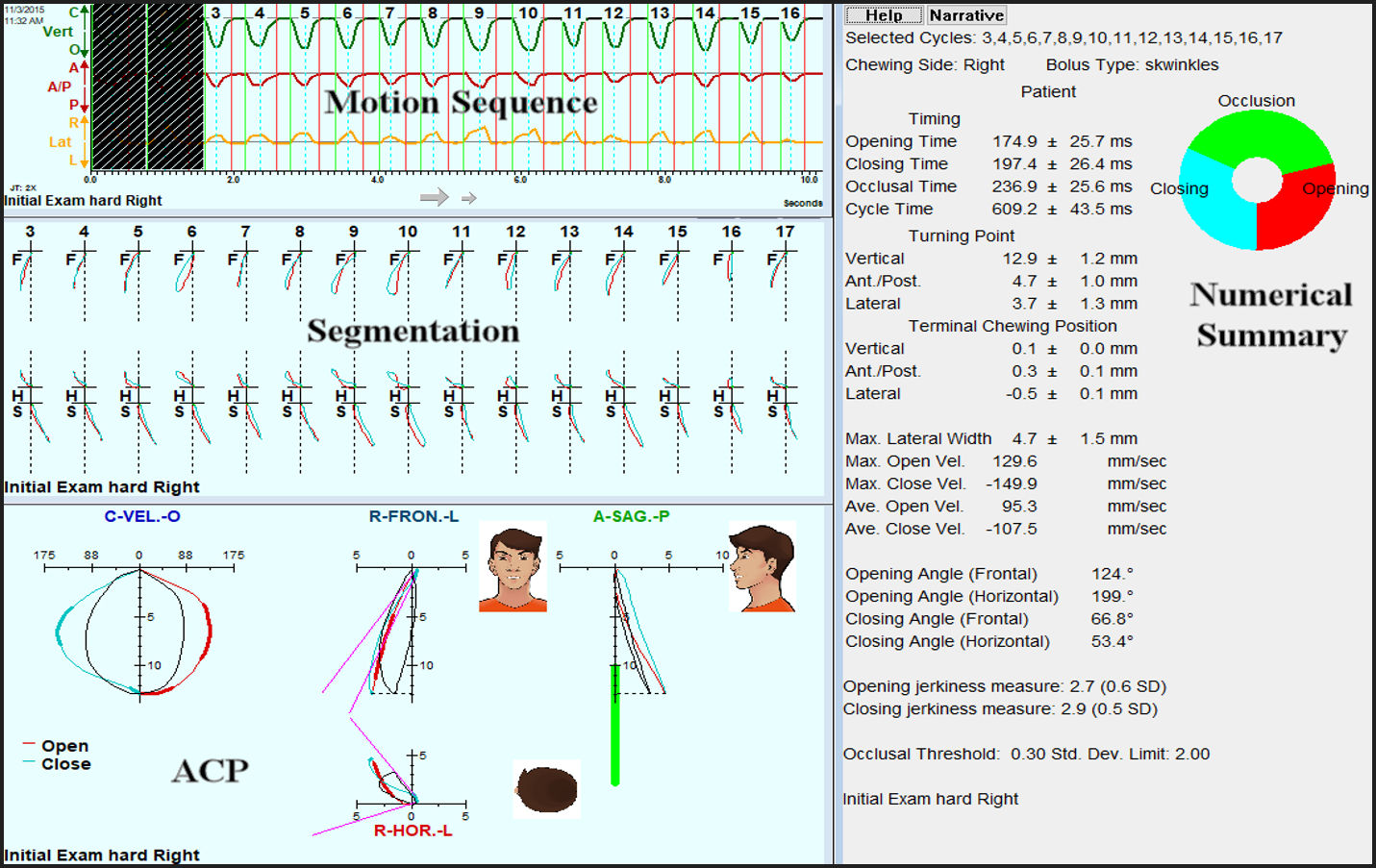
The BioPAK Computer Program segmented the chewing sequence movement into individual cycles. See Figure 5. Then an Average Chewing Pattern (ACP) was calculated and graphed to reveal the underlying pattern in relation to the mean normal pattern (black lines). A summary was also created describing the chewing motion numerically.

The simultaneously recorded EMG activity was also averaged by muscle to create the graph of the Average Chewing Cycle (ACC) of muscle activity, along with a numerical summary of the EMG activity. See Figure 6. The Superimposed View of the EMG activity reveals graphically the variability of the ACC pattern.

To provide a frame of reference, an asymptomatic control group’s data is also graphed. Figure 7.

Certain numerical parameters that are calculated within the BioPAK program, extracted from the motions and the muscle activities, have previously been identified as indicating the presence of various masticatory dysfunctions.21–25 The Cycle Time, the Antero-Posterior position at the Turning Point (most open position), the Maximum Lateral Width of the frontal movement pattern, the Maximum Opening Velocity and the Maximum Closing Velocity were selected as parameters to be tested within this study. In addition, the Opening and Closing Jerkiness values were calculated. See Figure 8.
.jpg)
For the EMG analysis five additional parameters were calculated; 1) the Mean Area representing the total work (mean integrated activity) of all four muscles, 2) the Coefficient of Variation of the working activity of all four muscles, 3) the mean Peak Amplitude of the activity for all four muscles, 4) the mean Time to Peak Amplitude of the activity of all four muscles measured from the onset of opening and 5) the mean time from the Peak Amplitude to the End of Closure for all four muscles. Because the treatments applied to this group were heterogenous, it was not possible to test the efficacy of any specific treatment.
All subjects included in this study sought prosthodontic treatment to repair damaged or replace missing teeth. The treatments included single crowns, small bridges or full arch prostheses, with or without implant support. Inasmuch as this study simply evaluated the subject’s ability to masticate prior to and after routine prosthodontic treatments, an IRB exemption was granted. All treatments were provided following the recommendations of the World Medical Association Declaration of Helsinki. (a = 0.05 was chosen)
RESULTS
Masticatory movement patterns
According to the parameters selected, this group of thirty subjects exhibited only marginal masticatory dysfunction prior to prosthetic treatment. This is evident by comparison to the reference control group data. See Figure 9. The criteria requiring the ability to chew gum and a hard bolus actually eliminated any potential subjects with substantial dysfunction. The mean cycle times chewing gum were not significantly different from pre-treatment to post treatment and similar to the reference control group mean. The maximum lateral width did increase slightly, but not significantly with gum chewing post treatment. The jerkiness was slightly reduced during gum chewing post treatment, but also not significantly. However, the mean A/P Turning Point values did increase significantly (p < 0.0003 for left gum chewing and p < 0.0175 for right gum chewing). The opening velocity values were also significantly increased (p < 0.0381 for left gum chewing and p < 0.0364 for right gum chewing), but only the left gum chewing closing velocity exhibited a significant increase (p < 0.0236). Non-significant reductions in jerkiness were found for gum chewing.

The mastication of a hard (tough, resistant) bolus challenged the masticatory systems and consequently revealed more significant changes in the timing, maximum lateral width, the velocities and the jerkiness. See Figure 9. The maximum lateral width increased significantly for hard bolus mastication (p < 0.0495 for left and p < 0.0254 for right) post treatment. Both the left and right mastication maximum opening velocities increased significantly (p < 0.0235 for left, p < 0.0005 for right) and essentially reached the reference values. Likewise, the closing velocities increased significantly (p < 0.0048 for left, p < 0.0022 for right), better matching the reference values. The opening jerkiness reduced significantly for left-side hard bolus mastication (p < 0.0355), but did not reach significance or right chewing. Significant reductions in jerkiness were present in both left and right mastication of the hard bolus. See Figure 9.
Masticatory Muscle Activity Patterns
In terms of the overall work effort, (Mean Area), for gum chewing only the right-sided Mean Area was significantly reduced post treatment (p < 0.0116). The pre-treatment variability (indicated by Coefficient of Variation) was high compared to the reference value for all four conditions. It was reduced significantly post treatment for all (p < 0.05), but it did not reach the reference value for any condition. The Peak Amplitudes increased significantly for all four conditions even though the amount of Mean Area did not (p < 0.05). This was due to a shortened time of contraction at higher amplitudes, a common characteristic of efficient mastication.
The mean time from the onset of opening to the Peak Amplitude (Time to Peak Amplitude) of muscle activity decreased significantly for all four conditions (p < 0.05), which corresponds to shorter cycle times as well. An important parameter, the time from the Peak Amplitude to the End of Closure is related to the confidence of the subject. This parameter changed very significantly for all four conditions (P < 0.0111), indicating increased confidence and reduced hesitancy while chewing. See Figure 10.

DISCUSSION
A remarkable early effort was made to evaluate changes in masticatory function post treatment with complete maxillary and bilateral distal-extension mandibular removable partial dentures.26 The authors found that the velocity increased, the mandibular displacement also increased, the pattern of motion became more of a “teardrop” shape and the number of chewing cycles required was also reduced. In a subsequent study some adaptive changes were recorded in the masticatory movements after osseointegrated fixed prostheses were placed in edentulous patients.27 The authors found a shortened occlusal phase reducing cycle duration, higher mandibular velocity and a greater displacement, all of which were maintained long term.
Incisor-Point Movements
The subjects within this patient treatment group were not classified with temporomandibular disorders (TMD) but were in need of various prosthodontic restorations. The group exhibited less than ideal masticatory function, but some were well enough adapted that many of the group’s mean parameters fell within the limits of an asymptomatic control reference group. See Figure 9. This was most noticeable with the parameter Maximum Lateral Width. In general, when patients are muscularly well adapted to their specific dysfunctional situation, they are able to chew with a movement pattern that closely mimics a normal pattern regardless of the food hardness.28 The ability to chew a soft gum bolus with mostly normal movement parameters, but not as well a hard bolus, suggests an intermediate level of adaptation. The level of adaptability of the masticatory system has been previously shown to be robust.29
In aggregate, the post treatment movement parameter values for hard bolus mastication moved closer to the reference values, suggesting improved functional patterns post treatment. Only the opening jerkiness values of the right-side hard bolus mastication did not change significantly. That obviously was due to both the pre-treatment and post treatment values already nearly identical to the mean of the reference group.
The mean vertical opening is determined mostly by the size of the bolus by necessity regardless of the degree of dysfunction, but the mean antero-posterior range is subject to other factors such as the skeletal A/P relationship of the mandible to the maxilla in centric occlusion. When the mandible is distalized in the maximum intercuspal position, the chewing pattern tends to occur in a more forward position reducing the value of the A/P turning point. Consequently, an increase in the A/P turning point value commonly occurs when an over-closed bite is restored to a more normal vertical dimension because overclosure also tends to distalize the intercuspal position. The A/P turning point value increased in this group towards the reference value for all four conditions, suggesting an improved maxillo-mandibular relationship post treatment.
The degree of laterality of the frontal chewing pattern is a factor used in assessing mastication due to the known asymmetrical nature of it. An overly wide pattern is associated with a worn-flat occlusion (very low cuspal angles) while a very narrow pattern suggests either some occlusal restrictions or a wildly variable chewing pattern such that the left and right extreme movements are cancelled out by calculating the ACP. Within this group a significant increase in the maximum lateral width towards the reference value was measured only for the hard bolus condition post treatment.
Note: The mean normal opening movement begins towards the non-working side and then crosses over to the working side at about mid opening. The turning point (maximum vertical opening) is deflected to the working side as is the complete closure path. See Figure 5. However, chewing in children without fully developed dentitions is different enough from adults that comparison to this study is not warranted.30 See also Figure 5. In the presence of a unilateral posterior crossbite or a severe opening occlusal interference the normal sequence can be reversed.31 Reversed sequencing is an adaptation to a malocclusion that also alters the pattern of muscle function. Consequently, correction of the crossbite may not reduce the incidence of reversed sequencing comparable to control subjects.
The opening velocity is usually less affected by any dysfunction except by an opening occlusal interference, such as a crossbite32 or by a more restricted opening pathway.33 An introduced closing working side interference can decrease the closing velocity and narrow the closing path as the subject attempts to avoid the interference when approaching occlusion.34 Within this group, both the opening and closing velocities increased after treatment for seven of the eight values, except the right closing velocity of gum chewing. This result suggests that the prosthodontic treatment successfully improved the masticatory function of the group. However, it may not have been true for every patient.
The correction of class III malocclusions has demonstrated reduced jerkiness along with increased chewing velocity.35 A lack of smoothness or its inverse, jerkiness, has been evaluated and closely associated with masticatory dysfunction.36 Although gum chewing did not reveal significant reductions in jerkiness within this group, the hard bolus mastication did. This suggests that the level of dysfunction within this group was moderate on average and that their individual adaptations were usually sufficient to overcome any during gum chewing, but not as well when the challenge of a hard/tough bolus was masticated.
Muscle activity
Muscle activity during chewing has been shown to be stable within intraindividual repeated measures.37 Thus, any significant changes in the muscle activity cannot be credited to chance. Also, in the working portion of the cycle during closing, the activity of normal control subjects, is asymmetrical with more activity on the working
side than on the non-working side.38 See Figure 7. In asymptomatic groups, the working masseter is the most active followed by the working temporalis, the non-working temporalis and the least active muscle, the non-working masseter. This hierarchy is usually altered with significant dysfunction.
Considering the aggregate muscle activity value (Mean Area), this group only deviated (perhaps by chance) from the reference value when subjects chewed gum on the right side. See Figure 10. Consequently, the right-side gum chewing value reduced toward the reference value significantly after treatment (p < 0.0116) and the same direction (p = 0.0661 ns), but did not reach significance. Meanwhile the left-sided chewing did not show significant change in either case. Note that none of the four Mean Area values were hugely different from the reference value, suggesting that most of these subjects could probably chew gum or a hard bolus by using only a little extra effort.
The variability of the muscle activity as indicated by the coefficient of variation (CV) was reduced significantly in all four conditions after treatment (p < 0.05). Although none of the four conditions quite reached the CV level of the reference value, the statistically significant measured reductions that occurred can be viewed as real measured improvements in masticatory function.
The Peak Amplitudes in all four conditions were significantly increased by the treatments. The amount of work needed to crush a given bolus does not change between pre-treatment and post treatment. The work needed to crush the bolus can either be done slowly with less peak activity as is common when masticatory dysfunction is present or it can be done quickly with greater peak activity as seen in asymptomatic subject groups. The fact that this group increased their Peak Amplitude and at the same time reduced their Time to Peak Amplitude is strong evidence for improved masticatory function.
The importance of the measure of the time from the Peak Amplitude (PA) to the End of Closure (EOC) is related to the confidence of the subject. A confident chewing subject will reach PA well before EOC (maximum bolus crush). However, subjects lacking in masticating confidence will often apply their PA only after the bolus is full crushed and the mandible is secure in centric occlusion. Note: In this parameter a positive value indicates peaking prior to EOC and a negative value after EOC. See Figure 10. The significant changes in this parameter were the most dramatic and consistent of the five muscle parameters measured. Note: Both right side pretreatment values were negative (after EOC) and changed to positive values for both gum and the hard bolus after treatment, indicating most likely that there were higher average levels of dysfunction pre-treatment when the group chewed on the right side.
Gum chewing has an advantage for detecting occlusal interferences that produce exteroceptive suppression because normal subjects rarely ever produce any silent periods while chewing gum. See Figure 3. In contrast, a hard bolus can induce silent periods when it fractures unpredictably. However, the Chikki used in this study can be characterized as tough enough to resist unpredictable fractures.
Occlusal Adjustment has been shown to significantly reduce the incidence of silent period production15 as well as their durations.39 Likewise, orthodontic correction of incisor crossbites has also been shown to reduce the incidence and duration of nociceptive reflex-initiated silent periods.40 The limitation of Gum is that it does not challenge the system sufficiently to fully reveal all of the specific factors present in a moderately dysfunctional subject. A hard, tough resistant bolus challenges the system and reveals moderate dysfunction of the masticatory system more definitively than gum chewing.
LIMITATIONS
The heterogenous subject group of this study was selected from patients presenting at a university clinic seeking various fixed prosthodontic treatments. The purpose was to simulate a real clinic situation. Thus, no effort was made to limit the procedure types. Due to the wide variety of procedures done, it was not possible to test any one treatment for effectiveness. It was necessary to average the parameters across the group and only evaluate the changes within the group. It would be interesting to test specific prosthodontic procedures in separate future studies, evaluating one specific treatment at a time.
Incisor-point tracking requires consistently correct placement of the magnet in the labial vestibule, which is not at all difficult. However, aligning the sensor array to the magnet with the patient in the intercuspal position is not as precise. Fortunately, all of the measurements are relative to the intercuspal position and not dependent on the exact absolute starting relationship of the sensor array to the magnet. Errors in motion measurement should be randomly distributed throughout any group of thirty subjects and therefore tend to be cancelled out when the groups’ values are averaged. However, chance is not predictable with certainty and some degree of residual error may have been present.
The placement of EMG surface electrodes can vary from session to session, casting some doubt on the changes between pre-treatment and post treatment. Within a sizeable group of thirty subjects, the small variations due to electrode placements should also be randomly distributed and consequently tend to cancel out when averaged. However, some residual errors due to chance may have affected the outcome.
CONCLUSIONS
The prosthodontic treatments applied to this group of patients have significantly changed these objectively measured parameters towards more normal chewing motions and muscle activities. The mastication of a hard bolus challenged the masticatory system and more thoroughly revealed mild aberrant measures than the gum chewing. Only the detection of silent periods appears to be most appropriate for gum chewing. However, the highly dysfunctional patient may not be able to chew a hard bolus at all and therefore limited to only chewing gum. The recording of combined chewing motion and muscle activity is an effective method for detection of actual masticatory dysfunction and objectively measuring any improvement after treatment.
Potential Conflicts of Interest
The 1st and 2nd authors reported no conflicts. J Radke is the Chairman of the Board of Directors of BioResearch Associates, Inc. and receives no commissions from their sales.
Funding Statement
No funding was received in support of this activity.