


INTRODUCTION
Digital radiography has been used widely in medicine, but it was only in the 1980s that the first intraoral sensors were developed for use in dentistry. Initially, digital radiography includes the use of charged couple devices which marked the introduction of radiovisiography (RVG). Unfortunately, the early systems could not capture panoramic and cephalometric images, which was overcome by the advances in digital technology in later systems.1
Some of the advances are Computed tomography (CT), Magnetic resonance imaging, Cone beam computed tomography (CBCT) and many more.2 Computed Tomography has continued to evolve, contemporary multi-slice computed tomography (MSCT) allows the acquisition of large volumes of data, capturing a large section in less than a second. Although, offering spectacularly high-speed imaging of both hard and soft tissues, X-ray dose is high, the equipment is exceptionally expensive and generally only found in hospital settings. More recently, CBCT was developed as an alternative to Computed Tomography. CBCT had several advantages over CT such as; acquisition of data in one single 360 degree rotation, high resolution images at considerable lower radiation dose; cost effectiveness, etc.3,4
Clinical applications of CBCT are rapidly being applied in the dentistry. However, CBCT imaging is most frequently used for presurgical implant assessment as it provides precise alveolar bone measurements. CBCT is more practical and perhaps even better for implant assessment than CT. When comparing accuracy of diagnostic measurements between CT and CBCT; which are of crucial importance in determining accurate site for implant placement; CBCT was found just as accurate as CT.4,5
Previous studies showed that; the accuracy of linear measurements obtained by CBCT is comparable to the measurements by MSCT, which is considered as a gold standard.6,7
CBCT machines are usually not equipped with a cephalostat. Therefore, the skull might be in eccentric position during scanning procedure. The patient’s position might deviate from ideal before the exposure. It is important to determine whether the accuracy of measurements decreases or remains unchanged, when the patient’s head position changes.8 One of the study by Shiekhi et al (2012) reported that; the difference of position affects linear dimensions for CBCT. But the difference found was less than 0.5mm, so it was clinically acceptable.9
It is important to reproduce linear measurements accurately but at the lowest radiation dose possible. Chief advantages of CBCT over MSCT is lower radiation dose exposure. In their study; Chau et al stated that; CBCT delivered the lowest radiation dose to the organs, whereas spiral computed tomography (spiral CT) & MSCT delivered the highest dose.10
Thus, it is important to assess; the accuracy of CBCT and MSCT measurements and compare them to actual values using Digital Vernier Callipers (DVC). The other objective was to find out the effect of change in patient position on linear dimensions for both CBCT and MSCT. Hence the present study was undertaken to compare and analyze external linear measurements of dry mandibles in correct and rotated positions using both CBCT and MSCT.
OBJECTIVE
To reveal any significant differences between CBCT and MSCT accuracy in calculating linear measurements and to determine if positional alignment is critical for either machine.
MATERIALS & METHODS
The present in vitro study was conducted in Department of Oral Medicine and Radiology. Ethical approval for the study was obtained from institutional ethical committee.
Inclusion and Exclusion criteria
Total of 15 dry mandibles were selected irrespective of their size and shape and were selected for the present in vitro study. Both dentate and edentulous mandibles were considered for this study. Mandibles affected with any pathologies affecting their structural integrity were excluded from the study.
Procedure
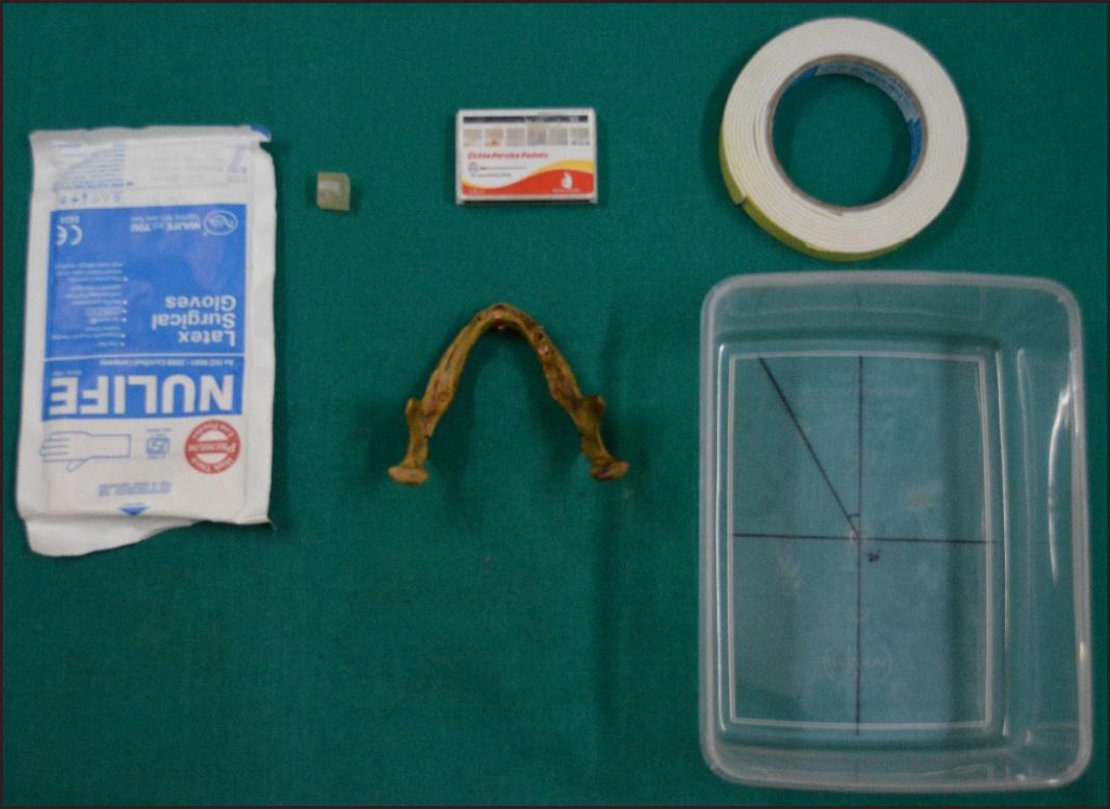
Supplies used are shown in Figure 1.
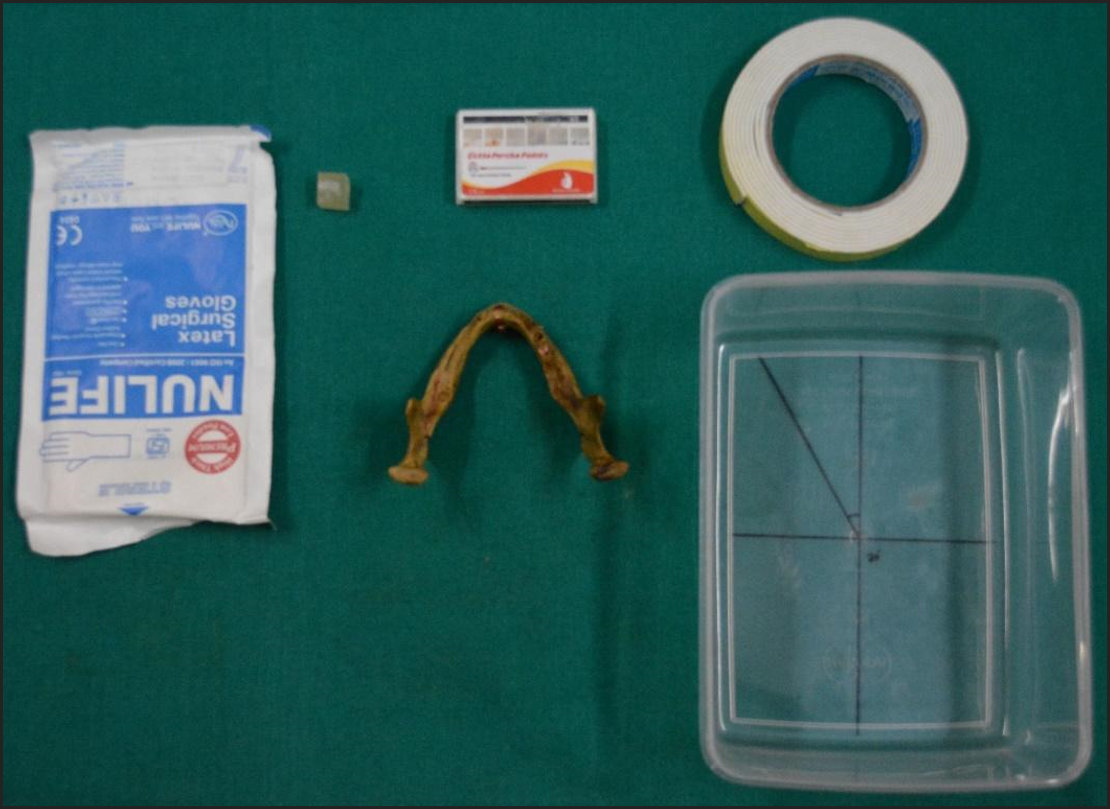
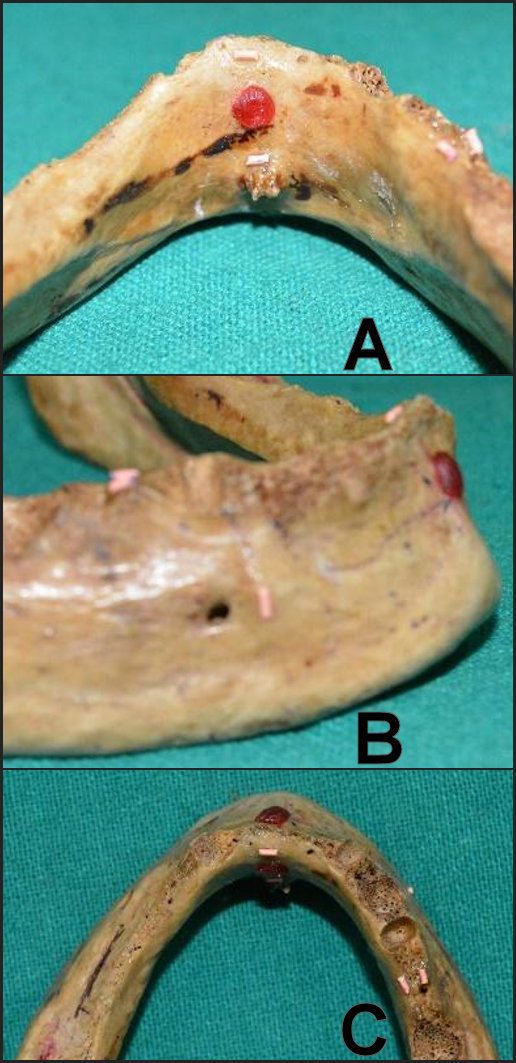
Number 40 gutta percha points were attached to five specific reference points on mandible. First reference point was superior border of lingual cortical plate in the midline of mandible. Second reference point was superior border of genial tubercle. Third reference point was anterior to the mental foramen. Whereas the fourth and fifth references were the superior border of buccal cortical plate in mandibular posterior region and the superior border of lingual cortical plate on the lingual cortical plate respectively. See Figure 2.
_reference_points_1_and_2_and_orientation_point_2._b)_reference_point_3_and_orientation_.jpg)
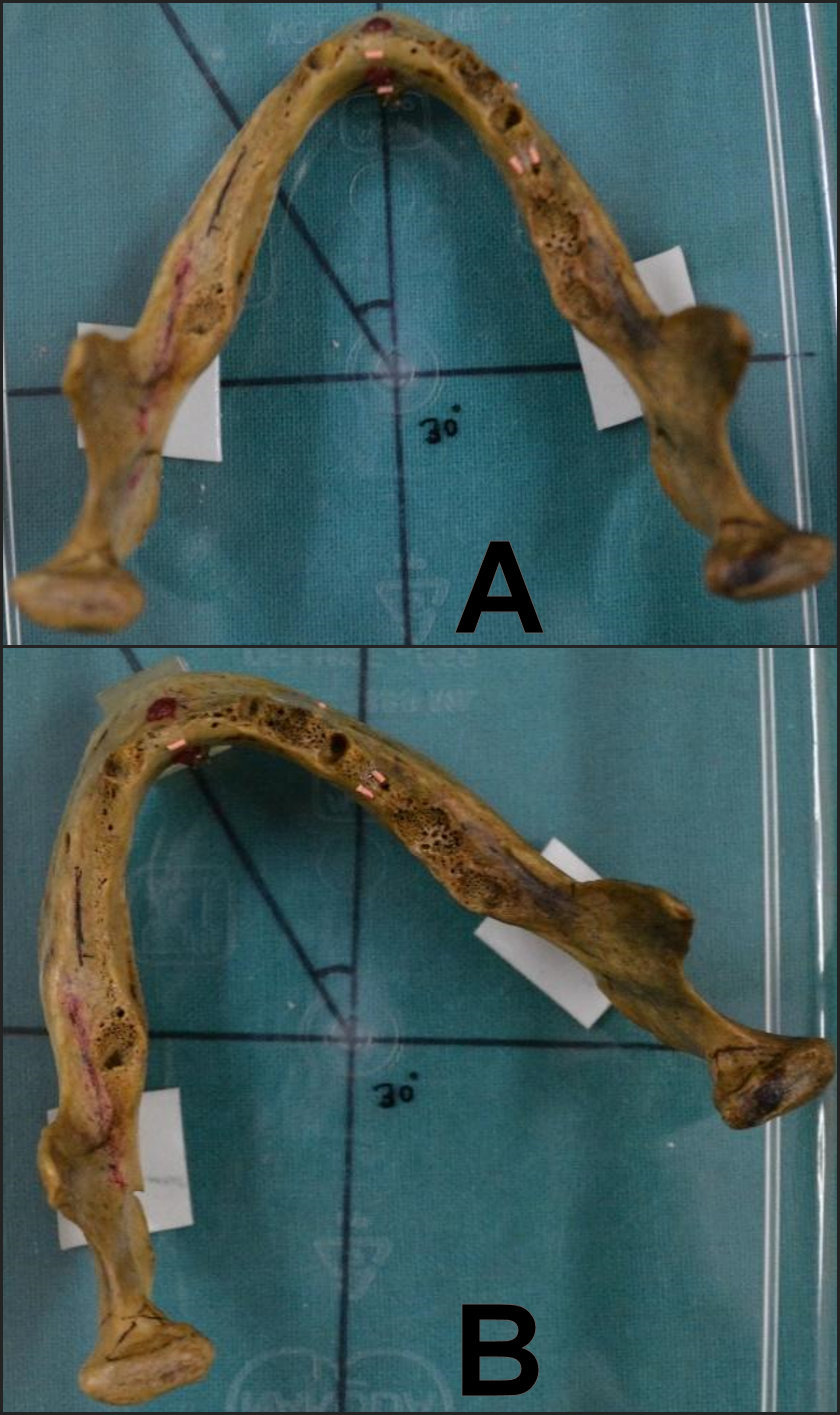
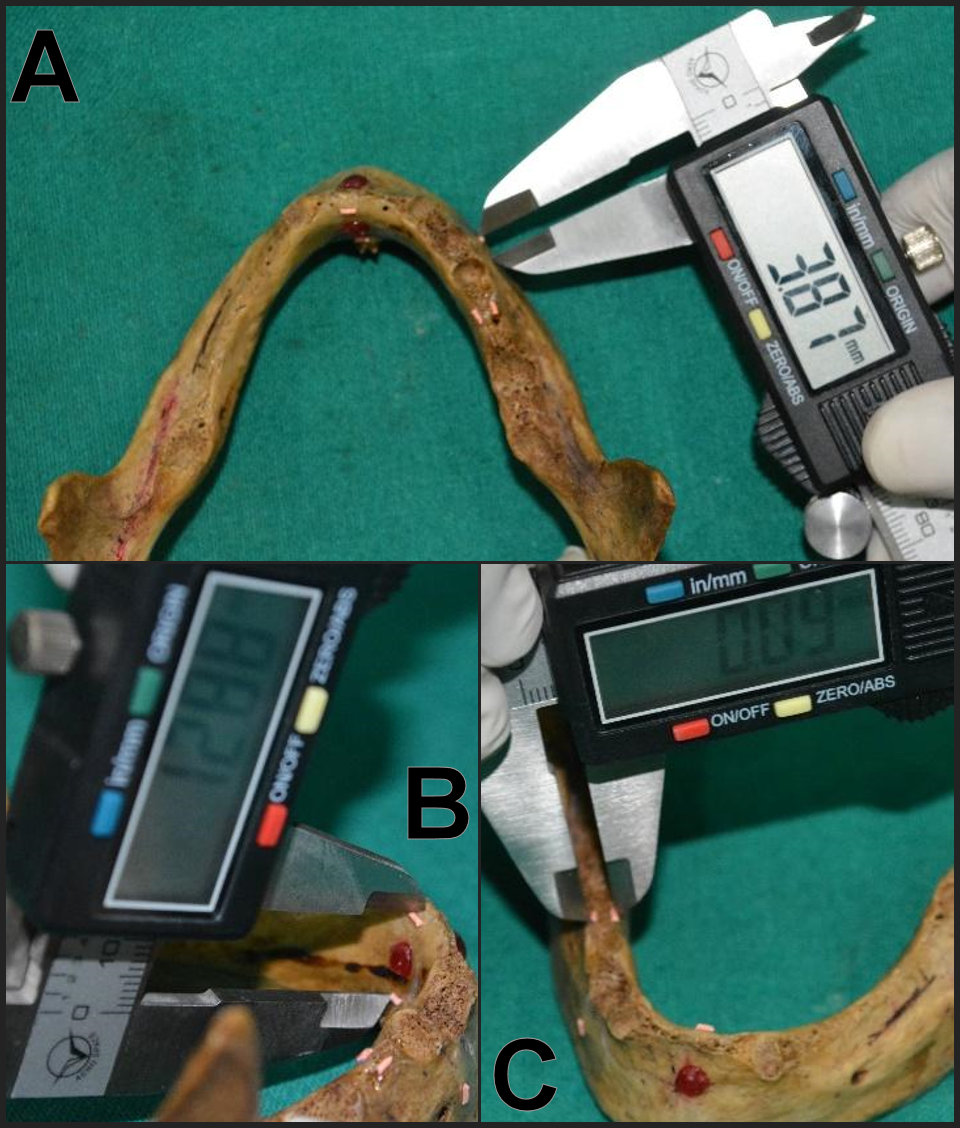
The distance between reference point no 1 and 2 was termed as DISTANCE 1. The distance between reference point 3 and the anterior aspect of the mental foramen was denoted as DISTANCE 2. The distance between points 4 and 5 was termed as DISTANCE 3. Direct measurements were obtained, using digital Vernier calliper for all 3 distances. Orientation points 1 and 2 were marked on the buccal and lingual cortical plate respectively using radiolucent material (modelling wax) in the midline of the mandible. Mandible was then fixed to the base of a custom-made container made of non-radiopaque material such that the line joining orientation points 1 and 2 was in the midline of the container. See Figure 3.
_normal_positioning_of_the_mandible._b)_rotated_positioning_of_the_mandible.jpg)
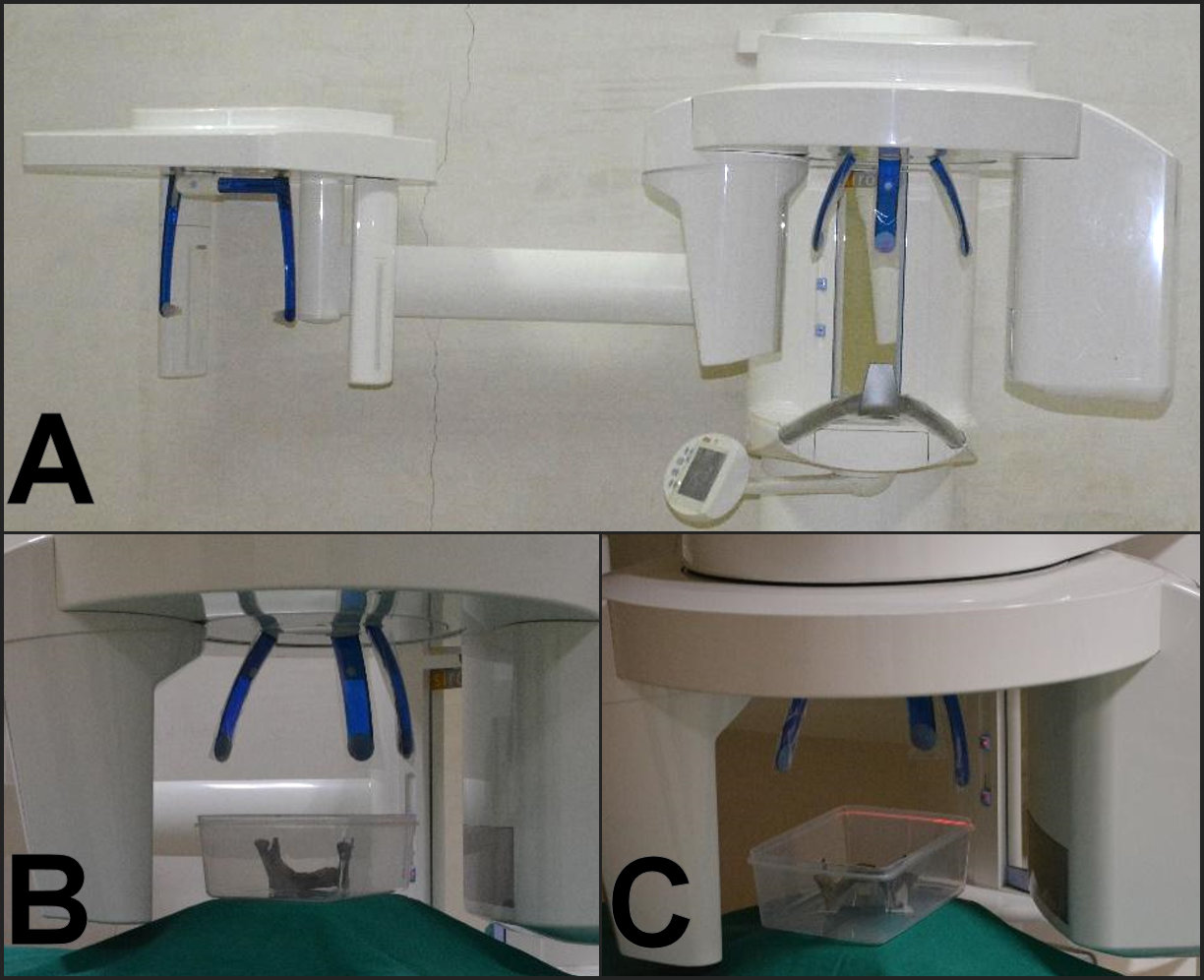
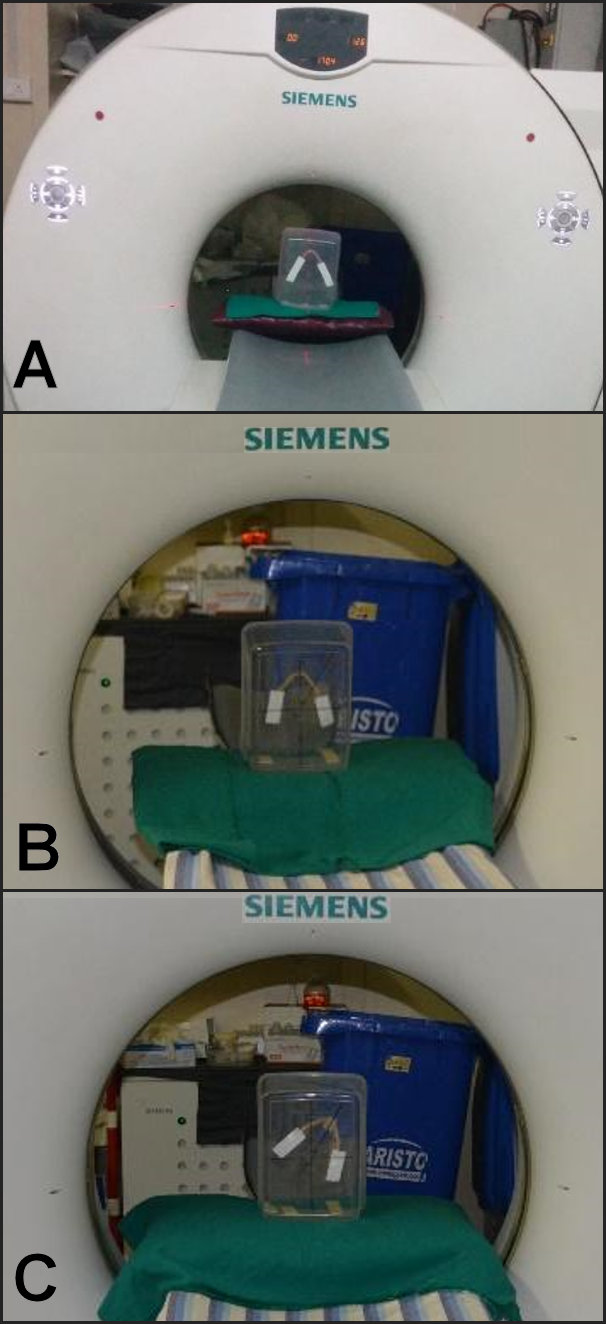
CBCT (Orthophos XG 3D, Sirona, Germany) and MSCT (SOMATOM Emotion 16 slice configuration, Siemens, Germany) scans were taken in this normal position. See Figures 4 & 5. Specifications used for CBCT were voxel size of 0.1mm with 85/7 Kv/mA and 3.2 seconds effective radiation time. Effective dose for the selected setting was 32 micro-Sieverts. Pixel size with 0.1 mm and flat panel detector with CMOS technology was used for CBCT machine. The software used was Galaxis Galileos viewer.
_cbct_machine._b)_normal_positioning_of_the_mandible._c)_rotated_positioning_of_the_mand.jpg)
_msct_machine._b)_normal_positioning_of_the_mandible._c)_rotated_positioning_of_the_mand.jpg)
Number of slices for MSCT scan was 16 x 0.6 mm / 16 x 1.2 mm. Voxel size was considered at 0.6 x 1.2 mm. Detector used for MSCT machine was ultrafast ceramic flat panel detector. For tomograms with MSCT, tube position was lateral and top, whereas specifications used were 30 mA and 130 kV. Similarly, for PNS spiral, X-ray exposure factors were 80 mA and 110 kV. Specifications used for reconstruction using MSCT were 0.75 mm size of slice with 0.3 mm of increment size. Caudocranial image order was considered for reconstruction program. Syngo software was used to view MSCT scans.
Due to difference in patient positioning protocols, plastic container along with mandible was oriented in horizontal position for CBCT and vertical position for MSCT. To mimic real situation like bone with soft tissues, exposures parameters were reduced for both CBCT and MSCT.
Measurements were performed on CBCT and MSCT using standardized linear measurement tools which provide submillimeter measurements. See Figure 6. DISTANCE 1 was measured on coronal view for both CBCT and MSCT. DISTANCE 2 was measured on axial view and DISTANCE 3 was measured on sagittal view for both CBCT and MSCT. Mandible was then rotated by 30 degrees and placed on custom made acrylic block (1.5 x 1.5 x 1 cm). Mandible along with acrylic block was fixed to the container in this rotated position such that; the line joining orientation point 1 and 2 was 30 degrees to the midline of the container. See Figure 1. CBCT and MSCT scans were taken, and measurements were performed like those performed on normal position. See Figure 7.
_distance_2._b)_measurements_obtained_by_digital_vernier_callipers._c)_distance_3.jpg)
_the_measurement_tools_of_cbct._b)_the_measurement_tools_of_msct.jpg)
Statistical Analysis
The data collected was tabulated, recorded in Microsoft excel and analyzed by SPSS software (IBM Corp. Released 2010. IBM SPSS Statistics for Windows, Version 19.0. Armonk, NY: IBM Corp). Comparison between measurements obtained using DVC, CBCT normal position, MSCT normal position and DVC, CBCT rotated position, MSCT rotated position was evaluated with one way ANOVA test (20 of freedom and 95% confidence level). Similarly, comparisons between measurements obtained using DVC, CBCT normal, CBCT rotated and DVC, MSCT normal, MSCT rotated were also assessed using one way ANOVA test. To assess the difference between CBCT and MSCT in normal and rotated positions the paired t test was used with 440 of freedom, at a 95% confidence level. The p-values less than 0.05 were considered statistically significant for Paired t Test and One way ANOVA Test.
RESULTS
Table 1 reveals the comparison of mean linear dimensions of mandible obtained in normal and rotated position using CBCT and MSCT. See Figure 8. Mean dimensions for both CBCT normal position and rotated positions were 7.78 mm. Whereas, MSCT normal and rotated position showed mean dimension of 7.8 mm and 7.82 mm respectively. See Figure 9. The paired t-test was applied to analyze for any differences between the dimensions of the mandibles in normal and rotated positions using CBCT and MSCT. No statistically significant differences were found in the dimensions of both the CBCT (p = 0.99) and the MSCT scans (p = 0.06) in normal and rotated position. Hence, there were no significant differences found between mean measurements of external surface of dry mandibles taken by CBCT and MSCT in the normal and rotated positions.
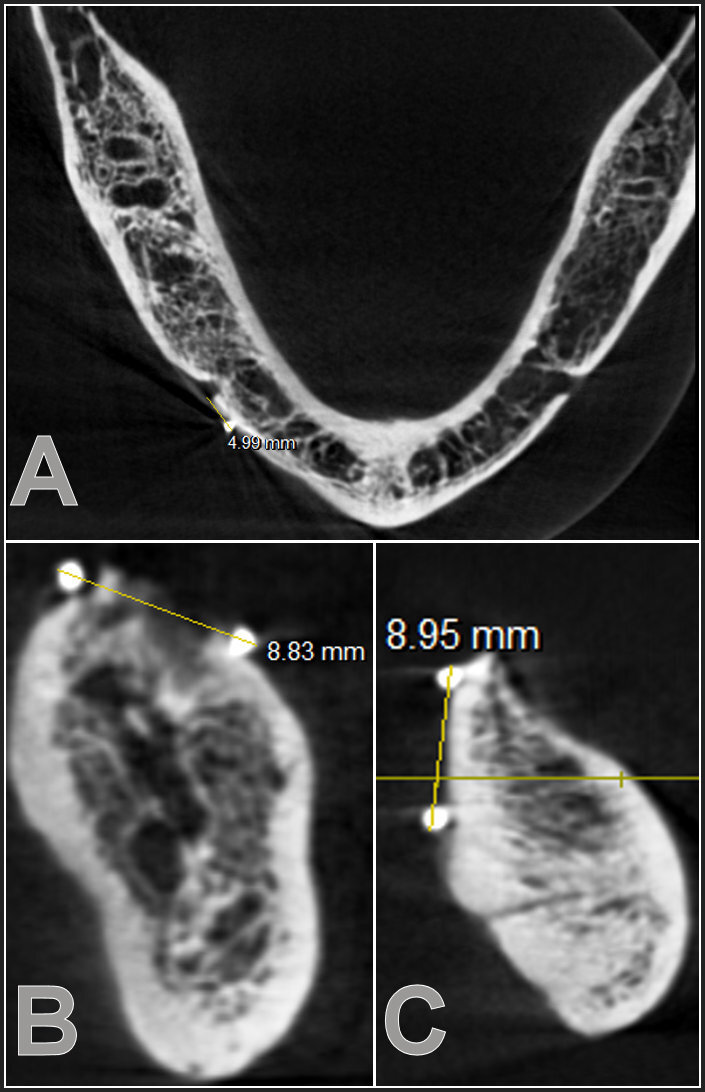

Table 2 depicts the comparison of linear dimension accuracies of the CBCT and MSCT scans in their normal and in rotated positions. A difference of 0.02 mm between mean measurements of external surface of dry mandibles taken by CBCT and MSCT were seen in the normal position, but this difference was not statistically significant (p = 0.16). Similarly, in the rotated position, differences of 0.04 mm were seen with both the CBCT scans, the MSCT scans and the differences observed were statistically significant (p < 0.05).
The mean dimension for the DVC was 7.67 mm, while for the CBCT normal position and the MSCT normal position the dimensions were 7.78 mm and 7.80 mm respectively. See Table 3. A statistically insignificant difference was found between the external dimensions obtained using DVC, CBCT and MSCT in normal positioning (p = 0.98). Whereas in the rotated position, the mean dimensions were 7.67mm for DVC, 7.78mm for CBCT, and 7.82 mm for MSCT. Statistically insignificant differences were found between the external dimensions obtained using DVC, CBCT and MSCT in the rotated position (p = 0.98). Comparison of linear dimensions of mandible using DVC, CBCT in normal and CBCT in rotated position was also done but the difference found was statistically insignificant (p = 0.99). Similarly, DVC was also compared with MSCT in normal and MSCT in rotated position and the difference found was also statistically insignificant (P = 0.98).
DISCUSSION
The present study was carried out to assess the accuracy of the linear measurements of dry mandibles on CBCT and MSCT in normal and rotated positions with reference to a digital vernier callipers.
In the present study, human dry mandibles were selected to assess linear measurement accuracy of CBCT and MSCT which was in accordance with a study by with Loubele M et al (2007).11 They compared dimensional accuracy of CBCT, MSCT and spiral CT using 25 dry human mandibles and one formalin fixed maxilla. Whereas Kobayashi K et al (2004) studied five cadaver mandibles to assess measurement accuracy of CBCT and spiral CT.12 However, Lagravere MO et al (2008)13 used a synthetic mandible and Mischkowsky RA et al (2007)14 used a dry skull and geometric phantom for geometric analysis in their studies.
The present study was carried out in vitro settings, to avoid any multiple ionizing radiation exposures to patients. Exposure parameters were reduced to achieve soft tissue simulation. This was in agreement with a study by Schropp L et al (2012) who stated that exposure parameters could be reduced if no material is used for soft tissue simulation.15 However, in a study by Moreira CR et al (2009)16 and Al Rawi B et al (2010)17 jaw bones were placed in a plastic container with water to achieve soft tissue simulation. Veyre-Goulet S et al (2008)18 used gutta percha points as radiopaque markers for assessing the accuracy of linear measurements using CBCT, which was in concurrence with our study.
Our study demonstrated statistically insignificant difference between the linear dimensions of CBCT in normal and rotated position of mandible (P = 0.99). Like the findings of CBCT, a statistically insignificant difference was found between the dimensions of MSCT in normal and rotated positions of mandible (P = 0.06). When the dimensions of CBCT in the normal position were compared with those of MSCT in the normal position, a statistically insignificant difference was found (P = 0.16). However, when the dimensions of CBCT measurements in the rotated position were compared with those of MSCT in the rotated position, a statistically significant difference was found (P = 0.02).
The present study also showed that there was a statistically insignificant difference between the dimensions of DVC, CBCT and MSCT in the normal and the rotated positions of mandible (P = 0.98). Al-Ekrish AA et al (2011) asserted that the CBCT measurements were significantly more accurate than those of MSCT and a statistically significant difference was found between mean absolute errors of CBCT and MSCT.19 However, in our study both CBCT and MSCT had very high linear measurement accuracy reproducing direct measurements precisely. This agreed with the studies by Kim M et al (2012)20 and Gaia BF et al (2014)21 who stated that the linear measurements were accurate for both CBCT and MSCT when compared with the true measurements. Similar results were demonstrated in a study conducted by Terra GT22 et al (2013) using spiral CT and CBCT, showing accurate linear measurements. However, Lascala CA et al (2004)23 and Fatemitabar S et al (2010)24 reported the underestimation of linear dimensions of dentomaxillofacial region by CBCT and MSCT, but a statistically insignificant difference was found between the direct measurements, CBCT and MSCT.
Our study showed that change in the orientation of the mandible had no effect on linear measurement accuracy with both CBCT and MSCT compared with direct measurements obtained using DVC (P = 0.99, P = 0.98 respectively). The results of our study were consistent with those of El-Beialy AR et al (2011) who stated that the accuracy and reliability of CBCT measurements were not affected by changing the skull orientation.25 Thus, they concluded that; the bite blocks and chin rests should not be considered as absolute requirements during CBCT imaging if a stable head position is ensured. Similar findings were reported by Ludlow JB et al (2007).26 Hassan B, et al (2009),27 Berco M, et al (2009),28 Lund H et al (2009),29 which were in concordance with our study. Whereas Sforza NM et al (2007) conducted a study to observe the effect of positioning of mandible on the accuracy of cross-sectional images obtained by reformatted CT scans. They concluded that the position of mandible in relation to CT gantry can influence the precision of linear measurements.30
CBCT can be recommended as a dose-sparing technique compared with the alternative of standard MSCT scans for common oral and maxillofacial radiographic imaging tasks. Effective dose from a standard dental protocol scan with the MSCT was from 1.5 to 12.3 times greater than comparable medium FOV CBCT scans.31 Additionally, a scout image is required for MSCT, which is responsible for the increase in radiation exposure, whereas most CBCT systems do not require scout images.
Since our study suggested that there was no difference between CBCT and MSCT in terms of linear measurement accuracy, and since the radiation dose of CBCT is considerably less than MSCT, CBCT should be used for oral and maxillofacial imaging over MSCT to minimize ionizing radiation exposure.
LIMITATIONS
One limitation of the present study was that the study used dry mandibles without the presence of soft tissues. The present study also comprised of only one CBCT machine. Further studies should be undertaken including multiple CBCT machines and a larger number of parameters.
CONCLUSIONS
The results of the present study can be concluded:
-
CBCT and MSCT are both highly accurate in terms of external linear dimensional accuracy.
-
Both CBCT and MSCT can reproduce actual dimensions in 1:1 ratio. There was no difference between external linear dimensional accuracy of CBCT and MSCT.
-
Linear measurement accuracy of CBCT and MSCT remains unaltered despite a change in the orientation of mandible. Thus, the use of bite blocks, contact segments, bars, rods and chin rests may not be considered as an absolute requirement for patient positioning in CBCT.
-
In the rotated position, differences of 0.04 mm were seen with both the CBCT and MSCT scans that were statistically significant (p < 0.05), but this small difference did not detract from the usefulness of the images produced.
-
However, due to its very low radiation exposure, ease of convenience and simple mechanism, CBCT should be preferred over MSCT in oral and maxillofacial imaging.
NOTE
This study was successfully defended for partial fulfilment of Master of Dental Surgery degree in Oral Medicine and Radiology.
Funding
This was a self-funded study.
Conflicts of interest
None were reported.