


INTRODUCTION
As estimated in many previous studies, the TMJ internal derangement (ID) is probably one of the most common symptoms that are associated with temporomandibular disorders (TMD). Reciprocal clicking (DDR) has been found in 7 % and with progression to TMJ locking (DD) with deviation to the affected side additionally in 12 % of a group of 403 non-TMD adults.1 This level of prevalence represents nearly 1 in 5 of the non-treatment-seeking public. In a study analyzing 115 TMD patients, 78 % had various stages of TMJ internal derangements while only 22 % had normal TMJs.2 Another study examining pre-orthodontic children clinically and using MRI found that 10 out of 51 had a history of pain or clicking of the TMJ.3 In a large pre-surgical study of 355 TMD patients, MRI indicated 72 % of the TMJs were found to have internal derangements and 28 % normal TMJs but only 50% of abnormal TMJs were correctly identified by clinical examination.4
The most common sub-categories of internal derangement are; 1) partial disc displacement with reduction (PDDR), 2) complete disc displacement with reduction (DDR),5 3) disc displacement without reduction (DD), 4) degenerative joint disease with arthritis or arthrosis (DJD) after long-term displaced disc.1–6 A fifth subcategory of “Stuck Disk,” although not common, is also sometimes present, but clinical diagnoses of ID very often do not match MRI diagnoses.6 The above categories correspond to the Piper classifications; a.) PDDR = Piper 3a, b.) DDR = Piper 4a and c.) DJD = Piper 5a if arthritis or Piper 5b after progressing to arthrosis.7 There is also a Piper 2 category that describes a loose capsule condition where the disk partially displaces, but only occasionally.
Since internal derangements have been found in up to 80 % of symptomatic subjects, but also in 33 % of so-called asymptomatic subjects when ID is not considered to be a symptom,8 it is likely that the difference may just be adaptability.9 Because internal derangements are prevalent, the accuracy of clinical examination to correctly identify TMJ internal derangements has been repeatedly questioned and measured with reliabilities of only 43 %10 to 59 %6 or 53 %.11 This lack of reliability of clinical examination methods suggests that an alternative needs to be employed when examining a TMD patient. JVA can be a quick, easy to implement adjunct to improve the clinical examination process.
Patients are often categorized as “myogenous” when muscle pain is their main reason for seeking treatment or “arthrogenous” when TMJ pain is their most significant complaint.12 However, in a study of 163 consecutive TMJ pain patients, the Kappa statistical test indicated poor diagnostic agreement between the presence of TMJ-related pain and the MRI diagnosis of TMJ ID (K = 0.16).13 In another similar study the Kappa found was (K = 0.21)14 In a comparison of the RDC/TMD to MRI, a Cohen’s Kappa of 0.223 was found for group IIa (DDR) and an overall Kappa of 0.336 that showed poor agreement.15 While TMJ pain is associated with the more severely degenerative internal derangements as indicated by MRI, it lacks specific diagnostic indications.16 Even though the clinical presentation of TMJ pain has been significantly correlated with synovitis,17–19 it is more often an indication that additional diagnostic procedures are needed to accurately evaluate the TMJ.
MRI to visualize disk position and inflammation and CBCT to visualize degenerative changes in bone provide morphologic views of the TMJ, but the usefulness of each is entirely dependent upon the quality of the radiologist’s interpretation. The predictive reliability of MRI has been shown to be excellent for normal discs, fair for anterior disc displacements with reduction, but less reliable for disc displacements without reduction because of false-positive MRI findings.12 Of course, there are also many temporomandibular disorders that do not involve the TMJ,20 but for those that do, a choice between MRI and CBCT may be necessary either for diagnostic or for economic reasons.
There are two distinct aspects to TMJ conditions: 1) the morphology and position of the disc, the condyle and the eminence and the soft tissue surrounding the joint or 2) the dynamic function of the joint as one structural component of the masticatory system. While imaging (MRI & CBCT combined) reveals condition 1 very well, attempts that have been made to visualize condition 2 with pseudo-dynamic MRI21 and semi-dynamic MRI22–24 at 3 to 15 frames/second have experienced very limited success. Since it is not economically feasible to image all patients with both CBCT and MRI, a bridge is needed to assist in the selection of the more likely beneficial technology. Our hypothesis is that JVA represents a bridge between the clinical examination and the imaging choice.
OBJECTIVE
Retrospectively evaluate four parameters of recorded vibrations from 114 dysfunctional TMJs (69 F) divided into 4 categories when compared to 86 (48 F) age and gender matched asymptomatic control TMJs.
METHODS
The temporomandibular Joint Vibration Analysis (JVA) records of TMD patients previously diagnosed by clinical examinations and imaging records with; a.) permanently non-reducing disk displacements, DD (29, 19F), b.) disk displacements with reduction, DDR (23, 13F), c.) partial disk displacements with reduction, PDDR (24, 14F) or d.) vibrating loose capsules without an internal derangement (38, 23F) were compared to control subjects (43, 23F) with bilaterally normal functioning and asymptomatic TMJs. See Figure 1. The mean intensities, the mean ranges of motion (ROM) and the mean frequency contents for each dysfunctional group were compared to the control group data using the Mann-Whitney U Test. (α = 0.05).

RESULTS
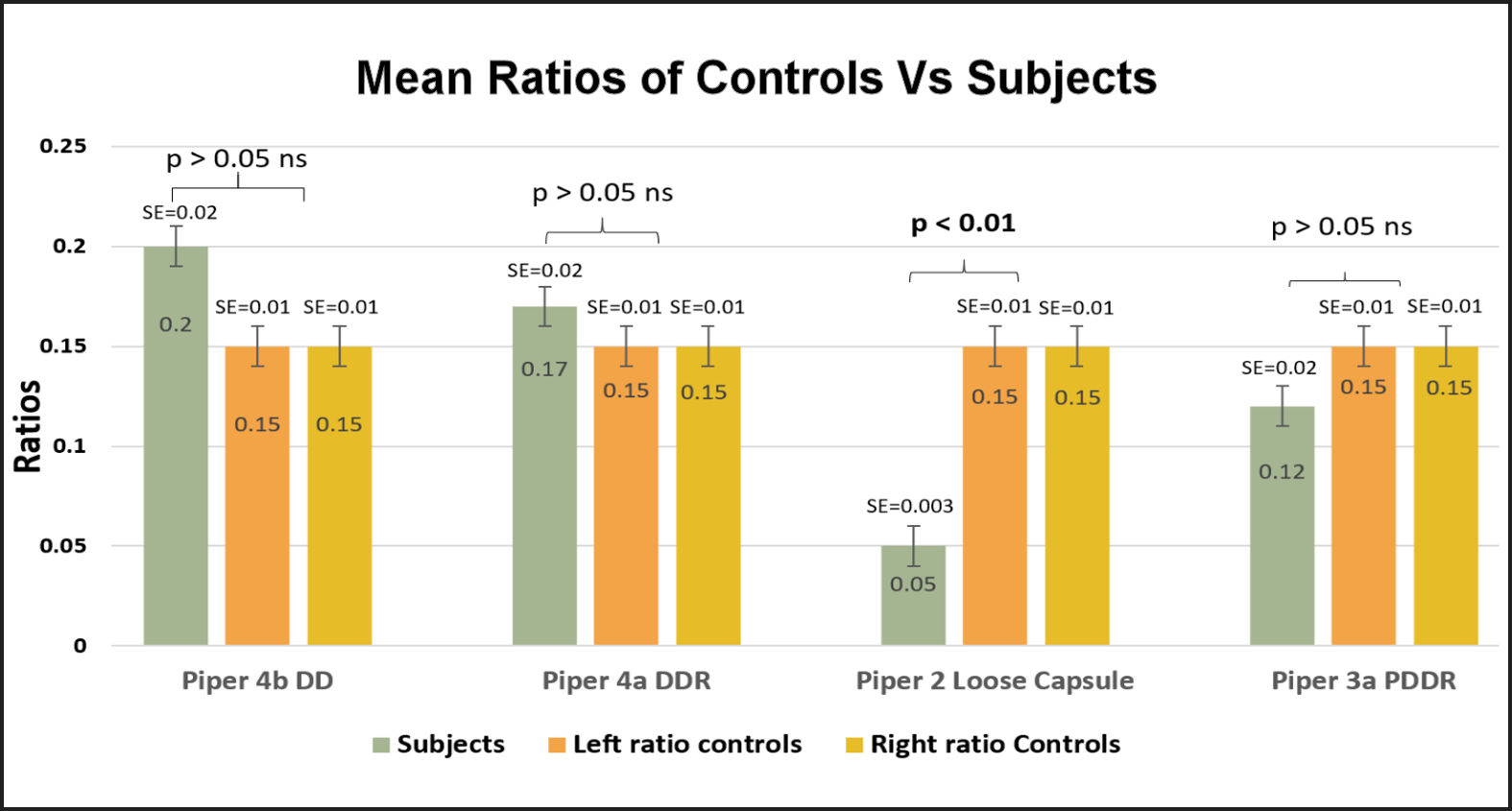
No significant differences were found in the mean ages of any of the several groups compared to the control group (p > 0.05). See Figure 2. No significant differences were found between the left and right TMJ vibration parameters of the control group in any measured parameter (p > 0.05). See Figures 3, 4 & 6.
._ba.jpg)

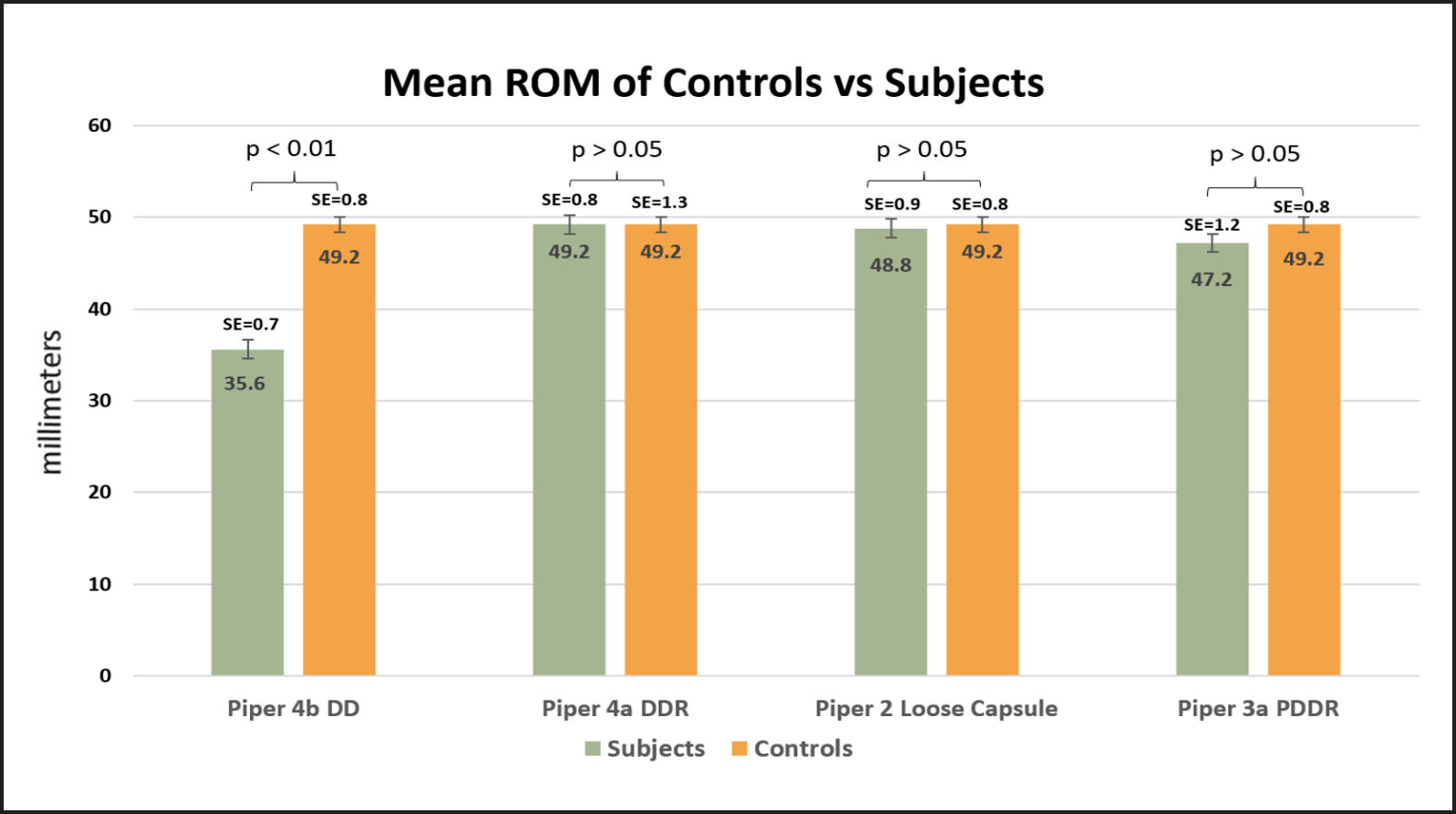
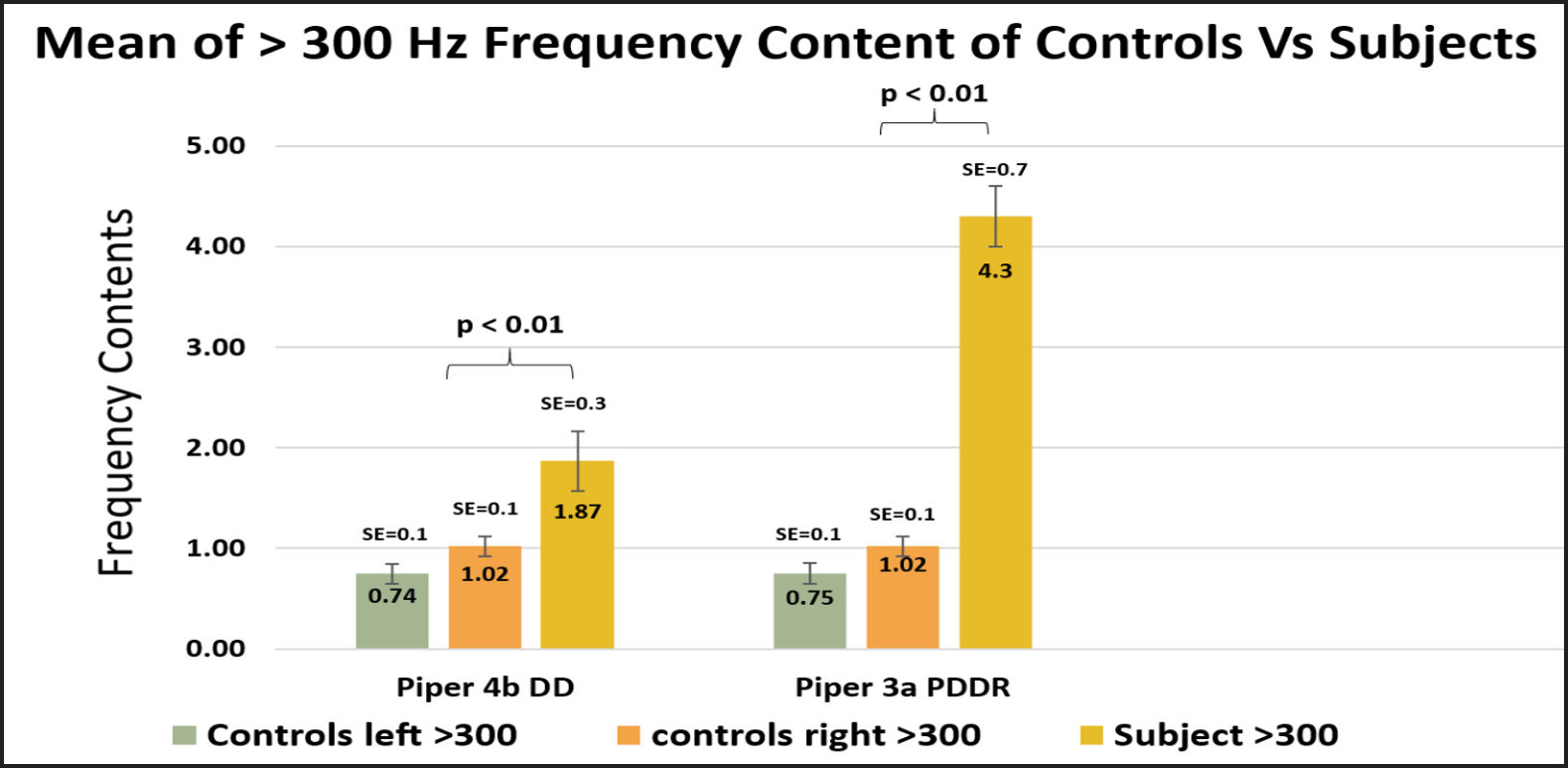
The mean vibration intensities of each of the four dysfunctional groups were significantly higher than the mean of the control group (p < 0.002). See Figure 3. A significant difference was found between the mean ratio of high to low frequencies within the loose capsule group (0.05 +/- 0.02) and the mean (0.15 +/- 0.1) of the control subjects (p = 0.00001). See Figure 4. A significantly reduced mean ROM (35.7 mm) in the DD group compared to the control group was found (p < 0.01). See Figure 5. A significant increase in the mean high frequency content was found within the permanently non-reducing disk displacement group (DD) compared to the controls (p < 0.0013). See Figure 6. A significant difference was found between the mean high frequency content of the partial disk displacement with reduction group (4.33 +/- 3.81) compared to the mean high frequency content (0.88 +/- 0.91) of the control subjects (p = 0.00001). See Figure 6.



DISCUSSION
Four common stages of internal derangements of the TMJ are 1.) vibrating loose capsules that have non-displacing disks, 2.) partial disk displacements with reduction, 3.) complete disk displacements with reduction and 4.) non-reducing permanent complete disk displacements.25 No single test is 100 % accurate in the process of differentiating between these four conditions. Thus, multiple inputs are required to arrive at a precise diagnosis. The process of TMJ diagnosis should begin with the patient’s history and a clinical examination.26 Joint vibration analysis is an intermediate step between clinical examination and MRI or CBCT imaging, to positively detect the presence of damage in the joint and to justify the added expense of imaging. JVA was never designed to be used in a vacuum, but to add additional dynamic data to the existing diagnostic process.
A vibrating loose capsule (hypermobility) may also be considered as only a pre-clinical condition, but it is not reliably detectable clinically or always with imaging.26 The mean intensity of the symptomatic subjects’ joint vibrations was significantly higher and the ratio lower compared to the controls (p < 0.01). This is because the vibration of a loose capsule is sub-audible and may or may not be detectable by palpation either as a joint wobble during closure, depending upon how loose it is. Since the disk is most often not displacing at all or only slightly, it may not be detected on an MRI either. Only the most experienced TMJ radiologist is likely to notice a Piper 2 (loose capsule) condition.
All mean intensities of the internal derangement conditions were found to be higher than control subjects’ mean intensities (p < 0.01). A quiet TMJ with a normal range of motion is the completely undamaged condition. To the contrary, some authors have claimed that a (clicking and/or popping) reducing displaced disk is an alternative normal condition, perhaps to rationalize its higher prevalence among post orthodontic patients.27 A quiet TMJ with a significantly reduced range of motion is a characteristic of a disk displacement without reduction. See Figure 5.
It is important to understand that relying on “sounds,” which imply human hearing, is very different from recording joint vibrations that are often inaudible. In one recent study the authors compared “click sound” to RDC/TMD and MRI diagnoses. None of the RDC/TMD diagnoses were in good or excellent agreement with MRI diagnoses and, contrary to every other joint sound study, they concluded that a “click sound” is more strongly correlated to disk displacement without reduction than to disk displacement with reduction.28 This erroneous conclusion can only be explained by the inaudible nature of certain TMJ vibrations. In contrast, JVA records a TMJ vibration 100 % of the time when a disk displacement reduces on opening. Other sound and vibration recording studies have arrived at the same conclusion.29–31
Although the recording of TMJ vibrations is not intended to provide a definitive diagnosis, it can reliably detect the presence of TMJ damage and provide a reliable indication when imaging is likely to add value to the diagnostic process. JVA can also detect the ipsilateral side when a medially displaced disk reducing causes bilateral vibrations, indistinguishable to palpation.30 No other criterion or “Indications for Imaging” are present in the dental literature besides TMJ pain, which is usually not specific. JVA is related to MRI and CBCT as it provides an indication of a dynamic function that complements the static images that reveal morphological data.
LIMITATIONS
The control group subjects were not imaged with MRI or CBCT scans to verify their normalcy. However, JVA has a been determined to have a 98 % specificity (determining normalcy), leaving a 2 % chance of false negatives.32 While the TMD patients provided a medical history, were examined clinically and received either MRI or CBCT imaging in addition to JVA, the control group subjects were not examined clinically and their TMJ conditions were determined to be asymptomatic by history and JVA only.
CONCLUSIONS
The four parameters; 1) Range of Motion to maximum opening, 2) vibration intensity, 3) high frequency content and 4) the ratio of high to low frequencies each contributed to distinguishing differences between the dysfunctional conditions of these four groups of TMD patients when compared to the asymptomatic control group.
Potential conflicts of interest
No conflict of interest was reported by Dr. Ruiz Velasco. Mr. John Radke is an engineer, a scientist and the chairman of the board of advisors for Bioresearch Associates, Inc. and Parvathi Kadamati is a biomedical engineer employed by same. Neither Mr. Radke nor Ms. Kadamati received any monetary or other inducement to participate in this research study.
Funding
No funding was provided for this research.