
INTRODUCTION
Musculature balance is the key to long-term case stability, whether orthodontic or restorative.1 Mandibular posture is intimately related to cervical posture through the musculature and fascia. Establishing physiologic rest and balance within both systems relies on correctly understanding anatomy, function, assessment protocols, and treatment modalities.2,3 Failure to diagnose and treat existing pathology within the musculoskeletal system, stomatognathic system, or fascia can limit case success and increase relapse potential.4,5
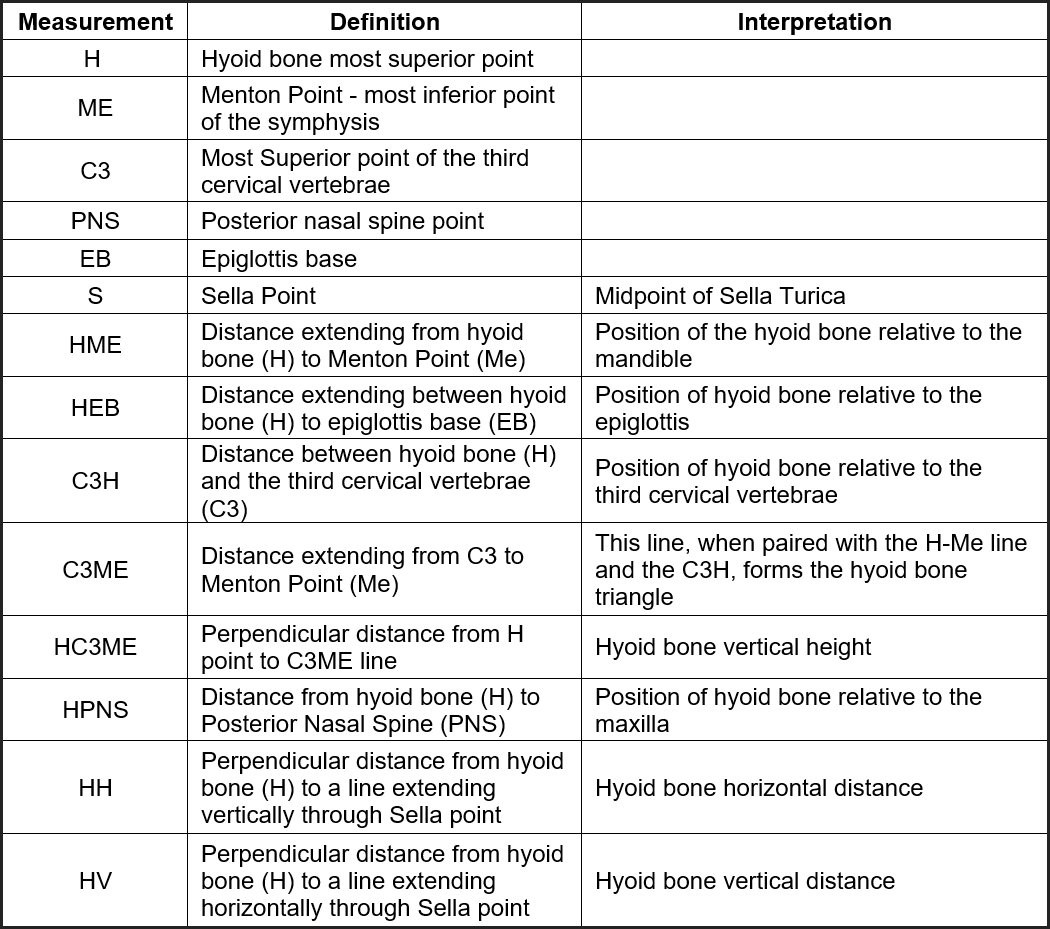
The hyoid bone is a horseshoe-shaped bone that plays a pivotal role in craniomandibular function because of its unique anatomy. It floats at the anterior portion of the neck between the mandible and thyroid cartilage at the level of C3.6 It has no bony articulations, which make movement and posture entirely dependent on attachments of ligaments, fascia, and muscles.7 It is critical for airway maintenance, mastication, phonation, swallowing, breathing, esophageal sphincter opening, tongue posture, craniocervical posture, mandibular posture, and shoulder girdle posture.7 Simply put, the hyoid bone position provides the link between craniocervical posture and craniomandibular posture, and its position may reflect the health of the head and neck.7 The hyoid bone position can easily be visualized on CBCT images. Noting the position of anatomical landmarks and measuring the distance between those landmarks is an accepted method for hyoid bone evaluation, especially when comparing pre- and post-treatment scans for a particular individual.8 A summary of the anatomical landmarks and their abbreviations may be referenced in Figure 1.

Fascia is the soft tissue component of the connective tissue system permeating the human body.9 It is composed of fibrous collagenous tissues constituting a body-wide tensional force transmission system.10 The fascial system is now seen as one interconnected tensional network that can adapt the arrangement of fibers and density according to the demands of local tensions.9 The lingual frenum is a central fold in a layer of fascia that extends across the floor of the mouth, not a discrete cord or band as often described in literature. The fascial fibers forming the frenulum have a basket-weave orientation as they cross the midline.11 Anterior tongue movements create tension in this central region of the floor of mouth fascia, which, when elevated, create the midline fold forming the lingual frenulum.11 The thickness of this fascia varies between individuals, which can cause functional restrictions, limiting tongue range of movement.11
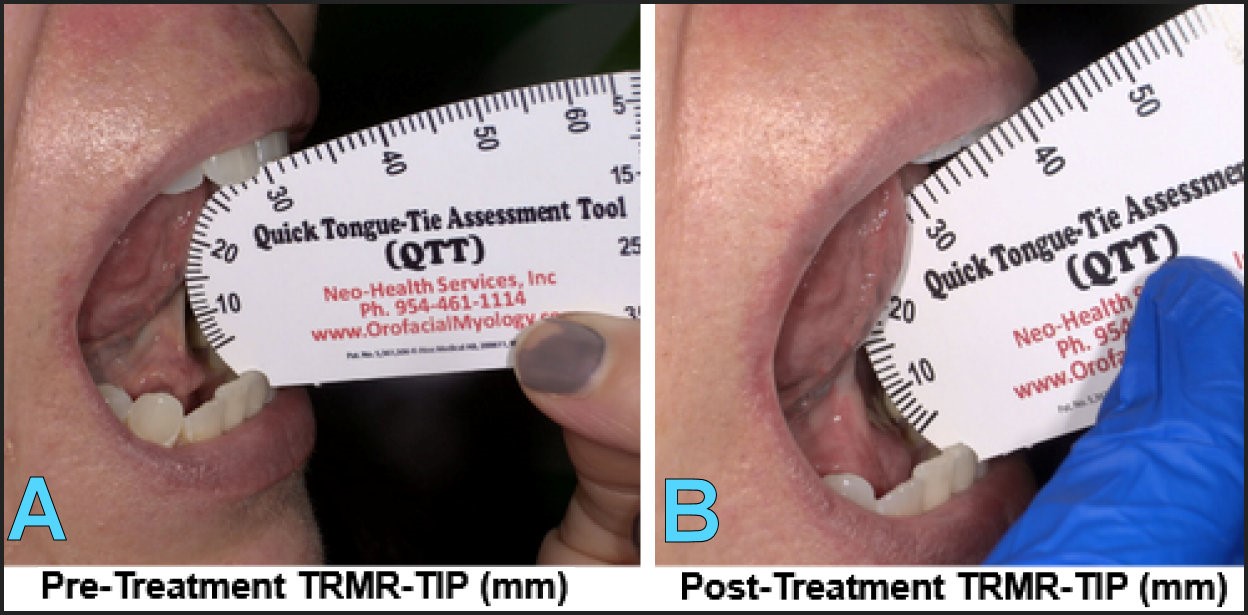
Functional Ankyloglossia is defined as restrictions existing in tongue mobility.12 Restricted tongue mobility and low tongue posture can impact speech, feeding, oral hygiene, maxillofacial development, mouth breathing, myofascial tension, and sleep disordered breathing.13 Assessment through the tongue range of motion ratio (TRMR), based on work by Irene Marchesan, is validated as a valuable tool for evaluating tongue mobility.13 This scale is based on two assessment criteria in comparison with the maximal interincisal mouth opening: (1) TIP - vertical extension of the tongue to the incisive papilla and (2) LPS - vertical extension when the tongue is held in suction against the roof of the mouth in lingual palatal suction.13 TRMR is the only independent measurement of tongue mobility directly associated with restrictions in tongue function.12 The Quick Tongue-Tie Assessment Tool (QTT) can quantify tongue range of motion (TIP and LPS) pre- and post-treatment to assess mobility improvements and treatment success. Figure 2 demonstrates using the QTT pre- and post-treatment to measure tongue range of motion with the tongue tip on the incisive papilla (TRM-TIP).
__post_treatment_range_of_motion_same_subj.jpeg)
Morphological changes to craniofacial development resulting from low resting tongue posture and tongue thrust follow the concept that form follows function.14 These morphological adaptations all result in a reduction, or obstruction, of pharyngeal airway volume. To compensate for the reduced airway space and improve airflow, the head extends forward, adopting a forward head posture.15,16 CBCT studies demonstrate that head extension reduces airway collapsibility, and flexion increases collapsibility.9 Removing the frenulum restriction and retraining normal function through a protocol of myofunctional therapy and frenectomy is paramount in addressing malocclusion and cervical mandibular dysfunction. Screening patients for airway adaptations impacting pharyngeal volume can be efficiently conducted through CBCT imaging software. A 2014 study by Mattos et al. found that cross-sectional areas at the levels of the palatal plane, soft palate, and tongue may provide reliable data for patient screening.17
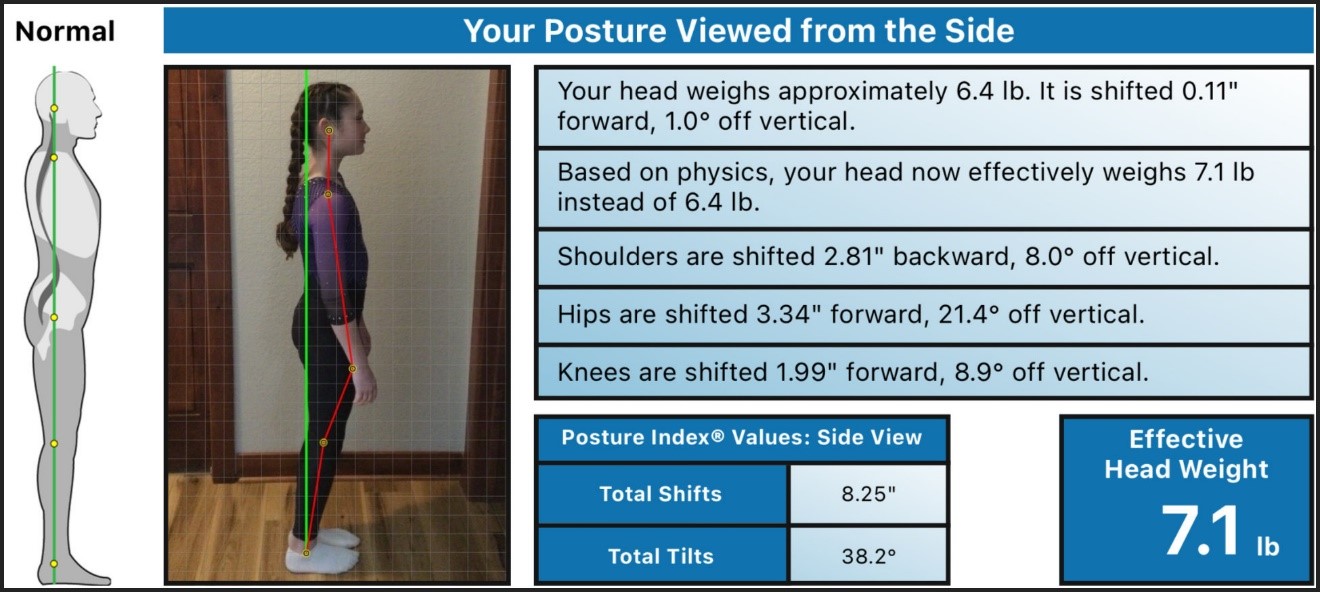
Forward head posture is the head’s anterior movement to the spine’s normal weight-bearing axis. It has been well established that head extension results in posterior displacement of the mandible, whereas head flexion causes the mandible to be displaced anteriorly.3,18 Goldstein, et al. demonstrated alterations in anterior-posterior head posture immediately affect the trajectory of the mandible on closure.19 Accepted methods for evaluating forward head posture include CBCT and lateral posture photo analysis. PostureScreen Mobile® (PostureCo Inc., Trinity, FL, USA) is a commercially sold photographic mobile application that identifies deviations from the ideal standing posture. A 2016 NIH study investigated the inter- and intra-rater agreement when using PSM, as well as understanding whether standard clothing can obscure the reliability of such measurements.20 The study’s results indicated that PSM is a reliable and user-friendly tool for characterizing static standing posture. Results of the study also suggest that to maximize agreement, assessments should be conducted with the subject wearing minimal clothing to better identify anatomical landmarks.20
Masticatory muscles accommodate to adapt to functional demands of occlusal interferences, cervical strain, tethered oral tissues, airway challenges, and ascending postural issues.14,21 This adaptive, or habitual, muscle position will impact occlusal relationships.22 It is, therefore, necessary to quantify and measure where the occlusion and rest position should be within the body’s unique physiological window so we can easily and predictably overcome pathological conditions.23 Utilization of ULF-TENS and the Myotronics K7 Evaluation System (Myotronics, Kent, WA, USA) for neuromuscular orthotic fabrication allows us to overcome pathologic conditions within the stomatognathic system.24 It is important to note that bioinstrumentation is excellent in establishing a proper physiological bite position on a neuromuscular trajectory.25 However, it does not reveal the underlying skeletal imbalances. This bioinstrumentation cannot be used without a proper skeletal analysis, both pre- and post-treatment.26
Our understanding of the anatomy and physiology of the cervical vertebrae, tongue and floor of mouth, hyoid bone, and fascial connections leads us to hypothesize that improvement in tongue function and occlusal relationships will lead to a reduction in forward head posture.
METHODS AND MATERIALS
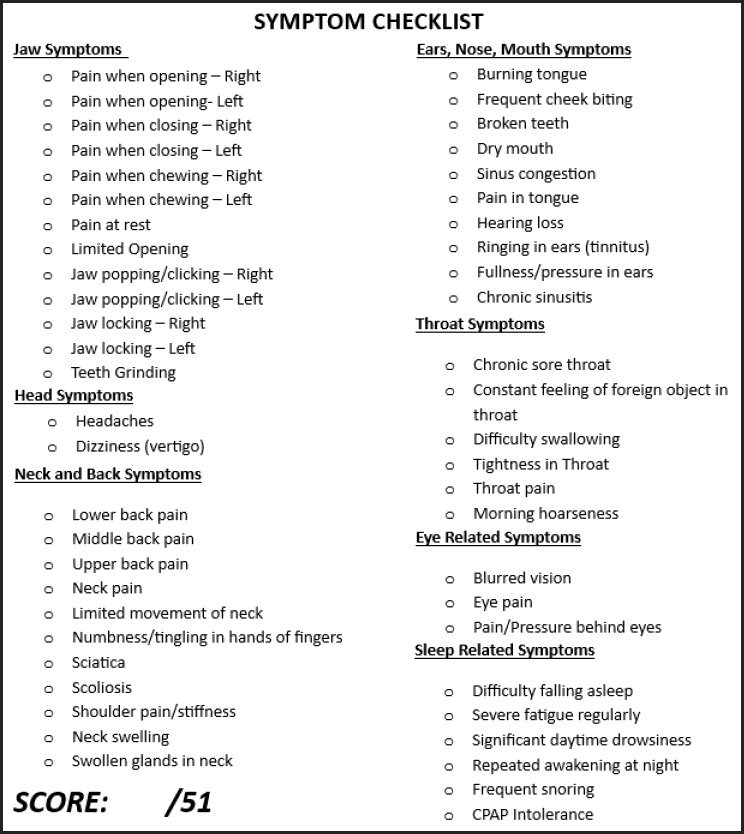
Pre- and post-treatment data was obtained on a sample of 32 female, symptomatic TMD patients between the ages of 25 and 70. Patient inclusion into the study required the following: (1) symptom checklist score of at least 5/51, (2) diagnosis of functional ankyloglossia obtained through TRMR-TIP, TRMR-LPS, and Floor of Mouth Hold assessments, (3) no body-work performed between the pre- and post-treatment evaluations. Informed consent was received from all patients.
Pre- and post-treatment tongue range of motion with tip of tongue on incisive papilla (TRM-TIP) was assessed through measuring and recording vertical extension of the tongue to the incisive papilla via the Quick Tongue Tie (QTT) Assessment Ruler ® (OrofacialMyology). See Figure 2.
Pre- and post-treatment subjective patient evaluations include the Symptom Checklist Score (Figure 3) and HIT6 Score (Figure 4). The Symptom Checklist Score is a number up to 51 (all symptoms) and is designed to represent the number of symptoms a patient is experiencing at a given moment. The HIT6 (Headache Impact Test) is a 6-item questionnaire that assesses the impact of headaches on daily life, with scores ranging from 36 to 78, where higher scores indicate a more significant impact.


Pre- and post-treatment lateral posture was assessed through the PostureScreen Mobile ® Application (Figure 5). The metrics recorded and compared were the head shift forward (mm) and head shift off of vertical (degrees).

CBCT images were taken in NHP (natural head position) with the following patient instructions: close mouth, breathe through the nose, place teeth together, swallow once, and then rest the tongue where it naturally goes. All images were taken by dental assistants extensively trained on the above protocol. CBCT images were taken on a Vatech Green CT SC 15x17cm view machine (Vatech Co., Ltd., Seoul, Korea), and the *.dicom files were evaluated by the same dentist using the Ez3D-i Software (Vatech Co., Ltd., Seoul, Korea). The following images were obtained for each patient in the study: (A) pre-treatment in habitual occlusion, (B) post-treatment in habitual occlusion, and (C) post-treatment in neuromuscular occlusion.
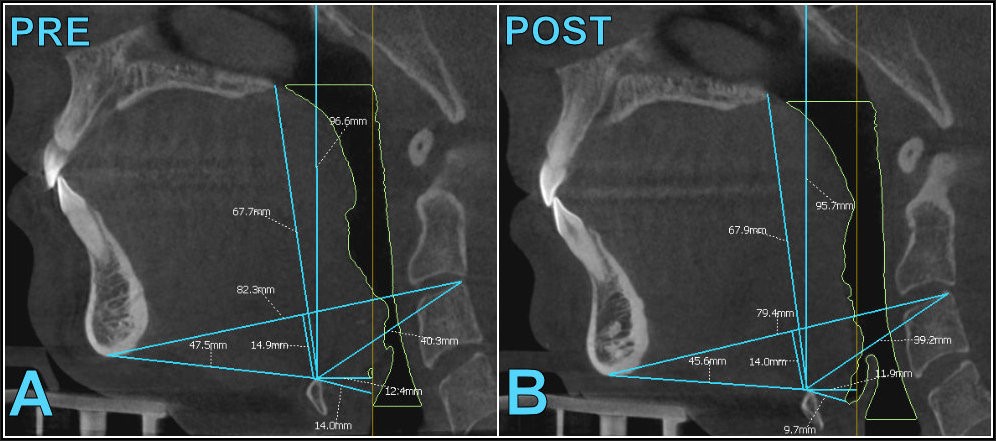
Data collection for each CBCT image included: (1) minimum cross-sectional area (mm2), (2) total airway volume (cc), (3) minimum lateral airway dimension (mm), (4) distance between anatomical landmarks (mm) for HME, HEB, C3H, C3ME, HC3ME, HPNS, HH, and HV. See Figure 1. All CBCT data collection was performed by the same dentist and reviewed by an independent evaluator for accuracy. Analysis example of CBCT image comparison pre-treatment, post-treatment habitual occlusion, and post-treatment neuromuscular occlusion on a single patient can be referenced in Figure 6.
_pre-treatment_and_(b)_post_treatment.jpeg)
Each of the 32 patients underwent a treatment protocol that included 8 sessions of myofunctional therapy, frenectomy, and fabrication of a neuromuscular orthotic. Myofunctional therapy was provided by one of two myofunctional therapists at the same office, using the same myofunctional therapy protocol. The protocol consisted of four pre-frenectomy sessions and four post-frenectomy sessions. The sessions were customized per patient to provide individualized care and spaced at least a week apart. A frenectomy was performed by the same dentist using a LightScalpel CO2 laser (LightScalpel, Bothell, WA, USA) under local anesthesia. The functional frenectomy technique was used, and silk sutures were placed. Healing exercises were given, and all patients were evaluated at one-week post-op before resuming the myofunctional therapy protocol. All treatment procedures were standard of care, none were experimental.
Neuromuscular occlusal position was established by the same neuromuscular dentist through a protocol of ULF-TENS, computerized mandibular tracking (CMS), and surface electromyography (sEMG) using the Myotronics K7 Evaluation System (Myotronics, Kent, WA, USA). Patients were placed on the Myotronics J5 ULF-TENS (Myotronics, Kent, WA, USA) for at least 40 minutes with a separating medium (cotton rolls) between the teeth. Verification of the lowering of EMG values after ULF-TENS was obtained with Scan 10 on the K7 Evaluation System.27 Instructions were followed for K7 Scan 4/5 to record the patient’s physiological rest position, and the desired neuromuscular/physiologic occlusal relationship was recorded with PVS bite registration material. This bite relationship was recorded with an iTERO intraoral scanner (Align Technology, Tempe, AZ, USA) for storage and lab fabrication of the removable neuromuscular orthosis. The removable neuromuscular orthosis allowed the patient to occlude in neuromuscular occlusion predictably and was inserted at least four months before the post-treatment CBCT images.
Statistical Analysis
The Wilcoxon Signed-Rank test is a “Paired” test specific for detecting significant changes within subjects while ignoring differences between subjects. It is the non-parametric equivalent of Student’s Paired T-test. This was used to compare pre-treatment to post-treatment patient data. The total sample size for the study was 32 subjects (n=32). The mean pre-treatment and post-treatment subjective outcome comparisons (Symptom Checklist Score and HIT-6) sample sizes were 21 subjects (n=21), as exclusions were made from the original dataset for incomplete post-treatment patient feedback. The CBCT mean pre-treatment to mean post-treatment habitual occlusion data comparison sample size were also decreased to 22 subjects (n=22), as 10 exclusions were made because the hyoid bone was not visible on their images. The comparison of the CBCT mean pre-treatment to the post-treatment with neuromuscular occlusion mean sample size was 28 subjects (n=28) for the same reason as stated above.
RESULTS
Pre- and post-treatment Symptom Checklist Score comparisons demonstrated a statistically significant decrease in mean score (p < 0.00001) with a pre-treatment score of 14.9 (±6.98) and a post-treatment score of 7.1 (±4.22). See Table 1. Pre- and post-treatment mean HIT-6 score comparison also displayed a statistically significant decrease (p<0.00001) with a pre-treatment score of 52.5 (±8.19) and post-treatment score of 44.6 (±5.44), See Table 1. TRM-TIP pre- and post-treatment mean measurements were found to have a statistically significant increase (p<0.00001), with a pre-treatment measurement of 25.3 (±7.12) mm and post-treatment measurement of 32.7 (±5.65) mm. See Table 1. As measured through PostureScreen Mobile ® application, lateral posture showed statistical improvements when pre- and post-treatment data was compared. Head shift forward improved from 1.81 (±0.75) inches to 1.37 (±0.69) inches (p < 0.00014). The head shift off vertical improved from 13.53 (±5.29) degrees to 10.31 (±5.36) degrees (p < 0.00043). See Table 2.
CBCT comparison study of airway metrics (total airway volume, minimum cross section airway, lateral minimum width) pre- and post-treatment indicate no statistical differences. CBCT comparison study of mean distance between anatomical landmarks pre- and post-treatment can be summarized as follows (See Table 3 and Table 4):
(1) Hyoid bone to epiglottis base (HEP): No statistical significance in comparison of mean pre- and post-treatment distance (habitual occlusion or neuromuscular occlusion).
(2) Hyoid bone to posterior nasal spine (HPNS): No statistical significance in comparison of mean pre- and post-treatment distance (habitual occlusion or neuromuscular occlusion).
(3) C3 to hyoid bone: Increase trend (p<0.0935) in comparison of mean pre- and post-treatment habitual occlusion distance. No statistical significance in the comparison of mean pre- and post-treatment neuromuscular occlusion distance.
(4) Hyoid bone to Menton (HME): Statistically significant decrease (p<0.0047) in comparison of mean pre- and post-treatment habitual occlusion distance. Statistically significant decrease (p<0.0017) in comparison of mean pre- and post-treatment neuromuscular occlusion distance.
(5) C3 to Menton (C3ME): Decrease trend (p<0.0618) in comparison of mean pre- and post-treatment habitual occlusion distance. Statistically significant decrease (p<0.0068) in comparison of mean pre- and post-treatment neuromuscular occlusion distance.
(6) Hyoid bone to a horizontal line from Sella Turcica (HV): Statistically significant increase (p<0.0072) in comparison of mean pre- and post-treatment habitual occlusion distance. Statistically significant increase (p<0.0294) in comparison of mean pre- and post-treatment neuromuscular occlusion distance.
(7) Hyoid bone to the vertical line from Sella Turcica (HH): Statistically significant decrease (p<0.0072) in comparison of mean pre- and post-treatment habitual occlusion distance. Decrease trend (p<0.918) in comparison of mean pre- and post-treatment neuromuscular occlusion distance.
(8) Hyoid triangle height (HC3ME): Decrease trend (p<0.0902) in comparison of mean pre- and post-treatment habitual occlusion distance. Statistically significant decrease (p<0.0202) in comparison of mean pre- and post-treatment neuromuscular occlusion distance.
DISCUSSION
Treatment protocol effectiveness is an essential aspect of establishing result validity. Quantifying patients’ subjective feelings about symptom improvement is one way to document this. The pre- and post-treatment comparison of mean Symptom Checklist Score and HIT-6 score demonstrate a statistically significant improvement in the patient’s subjective feelings about symptoms. Statistically significant improvements in TRM distance indicate the treatment approach of OMT and frenectomy effectively improved tongue mobility and functional ankyloglossia. Combining symptom improvement with improvements in physiologic tongue function suggests the treatment protocol (OMT, frenectomy, neuromuscular orthotic) provided to symptomatic TMD patients was effective and repeatable.
Data from comparison of lateral posture photos and distance between anatomical landmarks on CBCT indicate the treatment protocol also results in a reduction of forward head posture. Pre- and post-treatment comparisons of lateral head photos analyzed by the PostureScreen Mobile ® application demonstrate statistically significant improvements in mean head shift forward (mm) and head shift off of vertical (degrees). Additional analysis of comparisons of pre- and post-treatment CBCT distance between anatomical landmarks further confirms this postural change.
The statistically significant changes in the mean distance of anatomical landmarks from the hyoid bone leave us to evaluate whether there was a change in cervical posture, cranium position, or hyoid bone position. This author believes it is a combination of positional change of all three anatomical structures. Results support minimal hyoid bone movement and more dramatic positional changes with the cranium and C3. CBCT result comparisons suggest that changes result from cranial-cervical flexion, which will directly cause the improvement in forward head posture seen in lateral posture photo assessment. Interestingly, data comparison demonstrates more statistically significant changes occur when comparing pre- to post-treatment in neuromuscular vs. habitual occlusion. This would suggest that transition of a patient to neuromuscular occlusion from habitual occlusion allows for an additional decrease in forward head posture.
The theory that the decrease in forward head posture is due to an increase in cranial-cervical flexion is supported by the data comparing the distance of anatomical landmarks from the hyoid bone. There is a decrease in the mean distance from the chin to the hyoid bone, but the mean distance from the hyoid bone to C3 changes very little. In addition, we observed a decrease in the mean distance from C3 to Menton and a decrease in the mean depth measurement of the hyoid triangle (HC3ME). As flexion increases, Sella Turcica moves superiorly and posteriorly. This fits the observation that there is an increase in the mean distance from the hyoid bone to a horizontal line from Sella Turcica point (HV) and a decrease in the mean distance from the hyoid bone to a vertical line from Sella Turcica point (HH).
Data demonstrates no statistically significant changes additionally support the theory that changes are due to increased cranial-cervical flexion. An increase in cranial-cervical flexion would not affect vertical positional change of PNS (posterior nasal spine) or epiglottis base. No statistically significant change was noted in the mean vertical distance of hyoid bone to PNS or hyoid bone to epiglottis base, which would be expected if changes were due to cranial-cervical flexion.
CBCT studies demonstrate that head extension reduces airway collapsibility, and flexion increases collapsibility.28 Interestingly, we do not observe statistically significant changes regarding the pharyngeal airway metrics of total airway volume, minimal cross-sectional area, and minimum lateral airway width. If changes are due to cranial-cervical flexion as the above data suggests, we should see airway metrics indicating an increase in collapsibility. The fact that we do not observe this may suggest that the studied treatment protocol may increase airway volume, thereby reducing airway collapsibility. Still, these changes are not observed due to the dramatic improvements in forward-head posture.
LIMITATIONS
The smaller sample in this study (n=21 to n=32) creates limitations in that a larger sample size may impact comparison data, changing statistical trends to statistical significance. Training on CBCT acquisition will need to be addressed, as 10 images had to be dismissed for the purpose of this study as the hyoid bone fell outside the capture window. Technicians were so focused on the NHP method of image acquisition they did not monitor to make sure all anatomical landmarks desired were visible within image capture. Another limitation, and idea for further study, would be to directly measure cranial-cervical flexion metrics. This study focused on CBCT anatomical landmark distance comparison vs. CBCT measurement of cranial-cervical flexion. In analyzing the results of anatomical landmark distance, it became apparent that changes are likely due to increases in cranial-cervical flexion. Still, confirmation of this theory through further study and direct measurement is necessary.
CONCLUSIONS
A treatment protocol of OMT, frenectomy, and neuromuscular orthotic for symptomatic TMD patients effectively improves subjective symptoms and TRM-TIP measurements. Lateral patient photo analysis through the PostureScreen Mobile ® application demonstrates that this treatment protocol improves forward head posture (FHP). CBCT pre- and post-treatment data comparison further demonstrates this improvement in FHP may be due to an increase in cranial-cervical flexion, and transition to neuromuscular occlusion vs. habitual occlusion demonstrates more statistically significant improvement in forward head posture.
Disclosure Statement
No conflicts of interest were reported.
Funding statement
No money or in-kind value was received from any source for this work.