


INTRODUCTION
Pain of dental origin is most frequently related to structural alteration of individual teeth or the associated periodontium. Depending upon the localization of damage to either maxillary or mandibular structures, nociceptive sensory pain commonly follows the dermatomal distribution of the second or third divisions of the trigeminal nerve, but not to both. Exceptions arise when deviations occur concurrently in the structures of both the upper and lower jaws. However, generalized maxillary and mandibular pain involving both divisions may exist without apparent structural damage, and dentists and pain specialists need more insight into this enigma of intraoral tooth sensitivity to cold that follows non-dermatomal or multi-dermatomal pathways and extends beyond a single division of the trigeminal nerve.
Dental Cold Hypersensitivity (DCH) is an accepted explanation for generalized tooth sensitivity in the dermatomal distribution of both the second and third divisions of the trigeminal nerve. DCH affects both maxillary and mandibular teeth in 25-30% of the global population. Exposed dentinal tubules that activate trigeminal nerve afferents have been theorized as the cause of (DCH), also commonly known as dentinal hypersensitivity (DH).1–10
In the 1990s, Pashley identified cervical dentin hypersensitivity (CDH), originating from the cervical root of teeth, as distinct from DH. In clinical practice, DH typically presents as a dull pain and often resolves by itself in a week or two. CDH is an acute, sharp pain associated with cold exposure, which usually requires intervention, such as removing a biocorrosive agent or initiating occlusal therapy.11–14 DH is further distinguished as exposed coronal dentin presenting with a dull pain of presumed c-fiber origin, as distinguished from CDH occurring from exposed cervical dentinal tubules presenting with a sharp, fast pain attributed to a-delta fibers.6,15 Though several theories exist regarding the etiology of DH and CDH, the classical hydrodynamic theory proffered by Brännström & Åström in 1964, involving fluid flow within dentinal tubules, is currently the most widely accepted etiology.3,16 Various chemical medicaments, laser treatments, occlusal therapies, and medical grade ozone exposure have been purported to address DCH, with mixed and often less than predictable results.17–20 Due to the variability of treatment responses and the lack of improvement in some patients, practitioners may encounter complex DCH unrelated to the trigeminal c-fiber-alpha-delta nociceptors.
The presence of non-myelinated C-fibers in the dental pulp provides an alternative pathway for DCH. Although 90% of nerve fibers entering the dental pulp are myelinated sensory afferents from the trigeminal nerve, another 10% are unmyelinated sympathetic fibers arising from the superior cervical ganglion.3,21 Of note, parasympathetic fibers have not been histologically identified within the dental pulp.22–24 It is widely accepted that sympathetic c-fibers are a source of nociception and that the autonomic nervous system aids in regulating pain.25 It is beyond the scope of this paper to detail all mechanisms of sympathetic-mediated nociceptive, neuropathic, and inflammatory pain, but these pathways are detailed elsewhere.26–28 The sympathetic response to acute injury is vasodilatation; in chronic pain, there is sympathetic-maintained vasoconstriction.25 Sympathetically maintained pain, aka SMP (defined as confounding pain and hyperalgesia which is maintained by efferent sympathetic activity and circulating catecholamines), has been reported in the literature to occur throughout the body.29 Sympathetic nerve blocks are effective in modulating neuropathic pain and other SMPs elsewhere in the body, and this paper explores whether there may be analogous sympathetic nociception and altered blood flow in DCH.
A prior study supported a correlation between cervical spine innervation and confounding cases of DCH.30 In the present retrospective clinical study, the authors sought further support for the role of cervical input into DCH by anesthetizing the greater auricular nerve (GAN), a branch of the superficial cervical plexus. The Superior Cervical Ganglion of the sympathetic trunk sends branches to the common and external carotid vasculature, and it also supplies grey rami to cervical nerves C1 through C4, which in turn form the cervical plexus.31–33 VAS responses were recorded pre-block and post-block. A reduction in sensation was noted at the angle of the mandible to confirm a positive GAN block, but no branches of the trigeminal nerve were anesthetized. Responses were consistent with a cervical source of pain in some cases of DCH. Given that there was no intraoral sensory anesthesia initiated throughout the patient pool in this study, the positive responses are consistent with sympathetic c-fiber nociception of the cervical plexus as an alternative source of DCH. These findings may be supportive of exploring c-fiber nociception in other sources of facial pain.
MATERIALS & METHODS
Informed written consent was obtained from the 194 participants in the study in accordance with the World Medical Association Declaration of Helsinki, all of whom expressed DCH pain conditions, including a history of confounding cold sensitivity in their dentition. All subjects responded with moderate to severe tooth pain during a diagnostic 5-second ice-cold water swish test.
The Verbally Announced Score (VAS) responses of the patients (0 to 10) were assessed following uniform testing procedures as follows:
-
Water was cooled with ice for 5-6 minutes minimally in a cup
-
The patients were instructed to swish the cold water for 5 seconds before expectorating or swallowing and then asked to indicate the sensitivity of their teeth on a scale of 0 to 10 (10 unbearable pain, zero no pain)
-
The blocking GAN injections were given by one author (NY). Approximately 0.5 – 1.0 cc of Bupivicaine w/ 1:200 epinephrine was injected superficial to each sternocleidomastoid muscle using a 12.7mm needle with 2-4mm of subcutaneous penetration. The effectiveness of the GAN block was confirmed by subsequent anesthesia along the ipsilateral mandibular angle, the inferior aspect of the auricle, and the mastoid region
-
Approximately 10-15 minutes after each GAN block, a post-injection ice-cold water swish of approximately 5 seconds was once again initiated, and the second VAS was recorded. A retrospective statistical analysis was applied to the 194 patients in the study by an independent statistician (JR).
-
A separate group of subjects with their VAS = 0 prior to injection of the GAN and with zero post-injection response served as controls.
Inclusion Criteria
-
All subjects were older than 18 years of age
-
All patients previously sought professional opinions on tooth hypersensitivity to cold
-
Patients reported pain from cold drinks or foods affected their everyday life
-
Acceptance of the GAN injection procedure following informed consent
-
Patients with at least twenty vital permanent teeth
Exclusion Criteria
-
Allergy to Bupivicaine (Marcaine)
-
Evidence of active periodontal disease or pulpal pathology
-
Patients needing operative interventions due to dental pathology
-
Signs of profound and/or generalized gingival recession
-
Patients with anterior open bite
-
History of temporomandibular joint surgery
-
Evidence of failing restorations, cracked tooth syndrome, or retentive pins in dentin in either vital or non-vital teeth
-
Palato-gingival groove or other enamel invaginations
-
Patients with four or more endodontically treated teeth
Initiating the GAN Block to Reduce Excessive Sympathetic Tone and Test For the SDH Endotype
Following the preoperative cold-water swish, the patient’s neck was disinfected with alcohol-saturated gauze on both sides where the GAN nerve tracks closest to the epidermis. This was at the postero-superior aspect of the superficial fibers of the sternocleidomastoid (SCM) muscle at the level where a line drawn parallel with the inferior aspect of the mandibular angle intersects with the location of the GAN. Note: A line drawn parallel with the inferior aspect of the mandibular angle should intersect with the location of the GAN, just slightly superior to Erb’s point. See Figures 1 & 2. Using a ½-inch, ultra-short 30-gauge needle, the operator slowly injected 0.5 to 1.0 cc of bupivacaine with 1:200 epinephrine on one side of the neck, fanning out to ensure GAN saturation, while aspirating to avoid the external carotid vasculature. One rule was to never drop below the SCM to avoid anesthetizing the phrenic nerve. The usage of the ultra-short needle essentially removed that possibility from occurring.

_injection_of_a_patients__left_gan_using_an_ultra-short___inch__30-gauge_needle_using_.jpeg)
After injecting, the clinician looked for signs on the injected side to confirm that the ipsilateral GAN had been anesthetized (Figure 1). The inferior border/angle of the mandible, the ventral pinna, the inferior preauricular region and the mastoid region became anesthetized within a few minutes following a successful block. After 10 to 15 minutes, the clinician again prompted another cold-water swish, queried the patient as to their response, and looked for any change regarding their cold hypersensitivity. A decrease in the VAS response to the cold-water swish signified sympathetic inputs as likely contributory, and hence the presence of the SDH endotype. The patients were also queried as to any other profound changes that might have experienced due to the temporary blockage of excessive sympathetic tone.
The clinician then repeated the procedure on the contralateral side by injecting the other GAN, and once again began looking for signs of anesthetization and any subsequent changes from yet another ice-cold water swish challenge, as well as any other changes that they might have experienced in and around their head and neck region. A change in the intensity of the response to the cold-water swish on one side likely indicated that the SDH endotype was in play. The patients were informed that within 6-8 hours, any reduction in symptoms they may have experienced in sensitivity to cold would likely return to pre-injection levels after the local anesthetic wore off. Interestingly, in several cases the GAN block proved effective against other symptoms such as acute muscular trismus; however, the DCH levels in all 194 studied patients returned to baseline after the local anesthetic wore off.
The 194 subjects were divided into three similar sized groups as follows:
Group 1 – Subjects with zero VAS change in cold sensitivity after GAN block (n = 65).
Group 2 – Subjects with limited VAS reductions, post GAN block injection levels > 3.0 (n = 71).
Group 3 – Subjects with significant VAS reductions, post GAN block injection levels ≤ 3.0 (n= 58).
To identify any significant differences in the initial status of the three groups prior to the GAN block injections, the non-parametric Wilcoxon Rank-Sum Test was used to compare the pre-block VAS data, which was determined to be non-normal. Subsequently, the Sign Test was chosen to evaluate the within-subject changes in each group as reported from pre-block to post-block of the Great Auricular Nerve. The Sign Test was used when too many tied values were reported because no change occurred in the VAS. Student’s Paired T test and the Wilcoxon Signed-Rank test cannot handle many tied values.
STATISTICAL ANALYSIS
The means and standard deviations of the pre-injection and post-injection VAS sensitivities to ice-cold water swish were calculated for; a) the whole group, b) for a subgroup of all responders, and c) for those that responded maximally. Due to the subjective nature of the VAS data, the pre-injection and post-injection means were compared using the Wilcoxon Signed-Rank test to detect any significant differences. Alpha was selected at 0.05. The comparisons between groups pre and post injection were tested using the Wilcoxon Rank-Sum test.
RESULTS
Before the GAN block injections, each subject was tested for cold sensitivity. The pre-injection mean VAS sensitivity levels were compared between the three groups, including means between 6.1 and 6.7, and were found not to be significantly different (p > 0.05). See Table 1.
Ten minutes after the injections, all subjects were re-tested looking for any significant change in mean VAS levels. A significant reduction in patient-reported ice-cold water swish VAS responses was observed among the entire group of subjects (n =194) (p < 0.00001). See Table 2.
Based upon the subjects’ post-injection verbally announced scores, they were then categorized based upon their response levels into three groups: 1) no response, 2) a limited response and, 3) a maximal response.
The no response group, 65 of the 194 study participants, did not respond at all, with no significant change in their ice-cold water swish VAS after the GAN block. These non-responders did not possess the theoretical SDH endotype, at least not via the GAN anatomical pathway. There were two patients (1 %) who reported slight increases in their VAS numbers post-injection, which accounted for the slightly negative mean value of -0.04 for the mean change in sensitivity within the non-responding group. See Table 3. However, considering that VAS is a subjective patient report with low resolution, it is possible that those two minimal changes were not real. No subject complained that the GAN block itself was very uncomfortable.
Among the remaining 129 subjects, 71 showed a limited but significant reduction (p < 0.00001). See Table 4. This second group showed a significant, but limited response (Limited Responders) with a mean reduction from 6.44 to 4.14.
The remaining subgroup (n = 58) included those who reported their post-injection symptoms reduced their mean VAS (0 to 10) from a mean of 6.69 to 1.47. See Table 5. Within this maximal responder group, the reduction was found to be statistically significant (p < 0.00000). This third group showed a maximal response (Maximal Responders).
Focusing on the most sensitive patients, the 4th quartile subjects from each group were compared between pre-injection and post-injection. See Table 6. These were all the patients, n = 89 (45.9 %), who were initially reported VAS ≥ 7.5. The distribution of those in the 4th percentile among the three groups was non-responders = 16 (18 %), limited responders = 48 (53.9 %) and maximal responders = 25 (28.1 %). The non-responders had a significantly lower pre-GAN injection than the maximal responders (p < 0.0386). Otherwise, the significance levels were comparable to the whole group.
The comparison of the limited responders and the maximal responders is shown in Table 7. The latter group’s response was significantly greater (p < 0.00000) than the former group. The mean VAS post-GAN-block injection for the latter group was 1.48 (+/- 1.11), which is widely considered a successful resolution of sensitivity. However, for the limited responders, their mean post-GAN-block injection VAS was 4.14 (+/-2.02), commonly considered only a partial response or improvement.
DISCUSSION
The separation of Group 1 is quite clearly justified, as the members did not respond to the GAN-block injection at all, which suggests no GAN sympathetic nerve contribution to the symptom. The division of Groups 2 and 3 is somewhat less precise, as it has a degree of arbitrariness with the decision to consider a VAS score of 3 as mild, although it is a common practice. The rationale was that those in Group 2 were responders, but more likely had at least one additional factor besides a GAN sympathetic nerve input contributing to their VAS reports. Those in Group 3 may have had mostly or only a GAN sympathetic nerve input, as their response was more complete. Since there was no significant difference between the pre-GAN injection VAS means for these three groups (p > 0.05), the significant differences in their post-injection means were more likely etiological.
Since it is well accepted that tooth sensitivity to cold includes multiple etiologies, it would be reasonable to expect that within this group of subjects, some might have a single etiology while others could have multiple etiologies. That could account for the fact that the GAN injections had no effect on some, a partial effect on some, and a complete resolution of others.
The Sympathetic Effect upon DCH when the SDH Endotype was in Play
Importantly, the sympathetic fibers are efferent, not afferent, as their neighboring trigeminal sensory cohorts are. This is an important distinction, as the efferent sympathetic nerves induce changes in the smooth muscle arteriole endothelium, leading to contraction, which in turn causes vasoconstriction. Additionally, the sympathetic fibers can also cause a localized inflammatory response, leading to leakage of blood vessels within the affected pulpal arterioles. The concomitant release of biologically active sensory neuropeptides in the dental pulp causes vasodilation, leading to increased local tissue pressure and consequently, increased capillary permeability, resulting in plasma extravasation and edema formation.3 This leakage of fluids out of the arterioles and the subsequent edema substantially reduces blood flow distal to the affected region, potentially creating a hypoxic event given that the dental pulp is encased in a non-compliant, hard outer shell and has no room for volumetric expansion; a classic compartment syndrome.3,30
Reducing sympathetic nervous input via a local anesthetic block of the pathway whereby 3rd-order neurons that accompany the GAN may temporarily reverse the vasoconstriction/inflammatory response leading to edema cascade, resulting in almost instantaneously better perfusion of blood and reduction of the hypoxia within distal vessels of the pulpal arteriole system. This volumetric increase in blood flow and loss of hypoxia may be directly responsible for the instantaneous loss of cold hypersensitivity in individuals with the SDH endotype. One must always remember that the sources of the sympathetic nerve fibers present in the dental pulp are third-order, efferent, unmyelinated postganglionic sympathetic nerve fibers originating in the superior cervical ganglion of the neck.
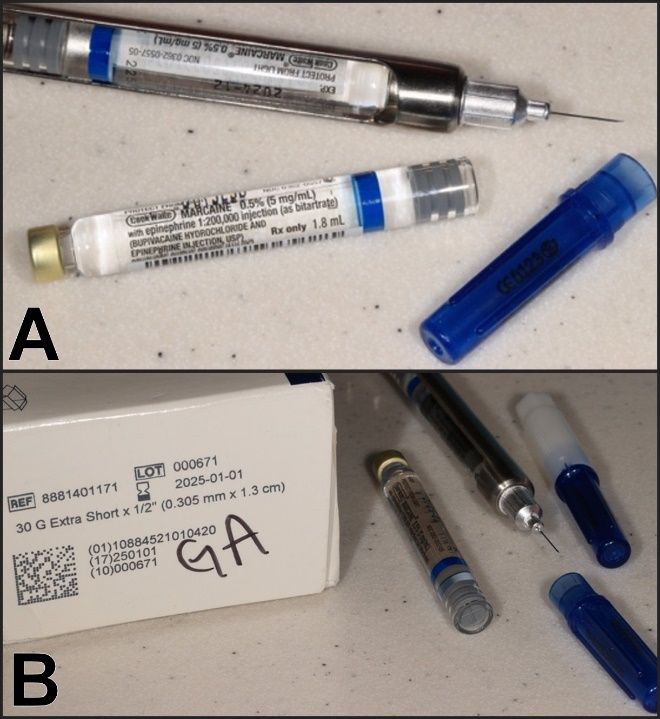
For a description of the sympathetic nervous system as it relates to the sympathetic anatomical pathways to the lateral face & ultimately the dentition.33 See Figure 8.
_the_30_gauge___inch__ultrashort_needle_used_by_the_authors_for_the_gan_block._ultrash.jpeg)

CONCLUSION
The significant temporary reduction in posterior tooth hypersensitivity to ice-cold water swishes within 129 of 194 subjects after local anesthetic injection of the Great Auricular Nerve branch of the Superficial Cervical Plexus supports a possible sympathetic neural system etiology enhancing sensitivity to cold. While 2/3 of the subjects (129) exhibited a sympathetic nerve contribution to their cold sensitivity, for nearly 1 in 5 it was their only factor leading to cold hypersensitivity. The third of this subject group not responding likely suffered from a different mechanism, or more likely, from involvement of the trigeminal nerve instead. The null hypothesis was rejected. It was concluded that, two out of three times, there may be a sympathetic etiologic component in the clinical manifestation of DCH and that Sympathetic Dental Hypersensitivity (SDH) can be a term applied in such instances.
Publication Abbreviations
-
DCH = Dental Cold Hypersensitivity
-
SMP = Sympathetically Maintained Pain
-
DCA = Dental Cold Allodynia
-
DH = Dentin Hypersensitivity
-
CDH = Cervical Dentin Hypersensitivity
-
SDH = Sympathetic Dental Hypersensitivity
-
SCG = Superior Cervical Ganglion
-
VAS = Verbal Analog Scale
-
SCM = Sternocleidomastoid Muscle
-
SCP = Superficial Cervical Plexus
FUNDING
No funding was provided from any source for this activity.
SPECIAL THANKS
To Mrs. Kennedy McDowell for searching the first author’s database and compiling the excel data from that patient pool in this retrospective study.
DISCLOSURE STATEMENT
John Radke who provided the statistical analyses is the Chairman of the Board of Directors of BioResearch Associates, Inc. The remaining authors declared no conflict of interest.