INTRODUCTION
For many edentulous patients, the conventional complete dentures have allowed them to eat, to speak and to function in the wider society more easily than they could without any prostheses. Despite this, it is well recognized that many struggles to use dentures, particularly the lower denture, because of mobility and discomfort, and these difficulties have been shown to result from regressive tissue changes or systemic health related conditions.1,2
Clinical studies over the last two decades have been undertaken to determine the benefits to patients from the use of mandibular implants to support the lower denture. Oral function improves significantly after fabrication of implant-supported over dentures and need 1.5 to 3.6 times fewer chewing strokes than conventional complete denture wearers to obtain an equivalent reduction in food particle size. This is because the maximum masticatory force of an implant-retained denture is 60% to 200% greater than that a conventional denture.3–9
The T-Scan III and BioEMG III are two separate computer technologies that have been synchronized together, so that an operator can record their separate diagnostic data simultaneously. The simultaneous recording and playback capacity of these two computer systems allows the operator to analyze and correlate specific occlusal moments to specific electromyographic changes that result from these occlusal moments. This synchronization capacity provides unparalleled evidence of the effect that the occlusal contact arrangement has on muscle function. Therefore, the occlusal condition of an inserted dental prosthesis or the occlusal scheme of the natural teeth (before and after corrective occlusal adjustments) can be readily evaluated, documented, and quantified for both, quality of occlusal parameters and muscular responses to the quality of the occlusal condition.10,11
AIM
To evaluate any changes in force distributions and muscle activities as patients transitioned from complete dentures to implant-supported dentures. A follow-up period of 6 months was chosen to included changes due to the process of adaptation to the new situation. A null hypothesis of no significant changes was postulated as well.
METHODS
This study was conducted within the department of Prosthodontics, Implantology and Oro Facial Pain Clinic Rajarajeswari Dental College and Hospital, Bangalore during the year 2016-17. A Certificate of Clearance was obtained (#RRDC&H/PG-121/2016-2017) from the ethical committee of Rajarajeswari Dental College for this topic of dissertation. The study population consisted of 50-75 years old healthy asymptomatic subjects. All the subjects were examined clinically. The inclusion and exclusion criteria were set to avoid any potential bias. Ten completely edentulous subjects (7 men, 3 female) with existing maxillary and mandibular conventional complete dentures and who had been completely edentulous for at least 1 year were included in the study. The primary complaints among the patients referred to the hospital for treatment were related to poor retention of mandibular denture, instability, denture sores and phonetic problems. Patients selected for the study were evaluated for adequate bone width and height to accommodate endosseous dental implant of diameter of 3.75 mm and length of 13 mm. Patients selected were having normal mandibular function with no mucosal and pathological changes in either maxilla or mandible. The study was conducted in three parts:
Part I
Conventional Complete Denture Fabrication
The treatment modalities were explained to the patient regarding an implant supported overdenture and an agreement was reached to fabricate a conventional complete denture first and follow that up with an implant supported overdenture. The old dentures were evaluated based on vertical dimensions, centric relation, retention and stability. Those dentures which did not fulfill the above-mentioned requirements, were replaced with newly fabricated conventional complete denture.
Bite Force and Muscles Activity Analysis
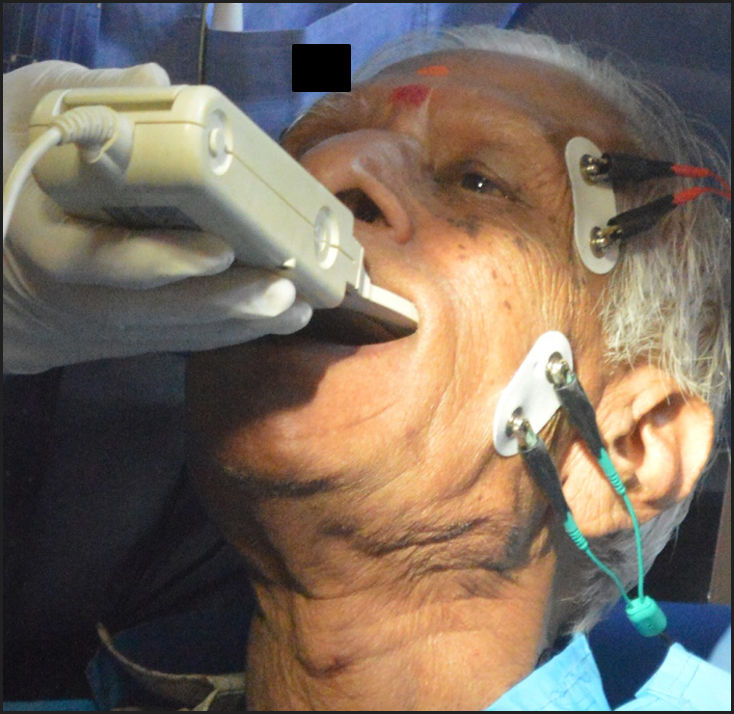
The patients were recalled for the bite force and muscle activity analysis, the T-Scan® III (Tekscan, Inc. ) was used for bite force analysis,
EMG muscle activity analysis, EMG surface electrodes were placed over the regions of the superficial masseter and anterior temporalis muscles bilaterally. The electrodes were connected to the BioEMG III amplifier (BioResearch Associates, Inc, Milwaukee, WI USA). See Figure 1.

Part II
Implant Placement& Denture Loading
Presurgical medical work-up was done followed by analysis of bone with the help of cone beam computed tomography (CBCT). It was decided to place two implants in the lateral regions, which was localized with the help of lead foil markers placed on the denture. An implant size with a diameter of 3.7 mm and length of 13 mm (MIS system) was decided upon. Locator size was selected with a 5 mm collar height.
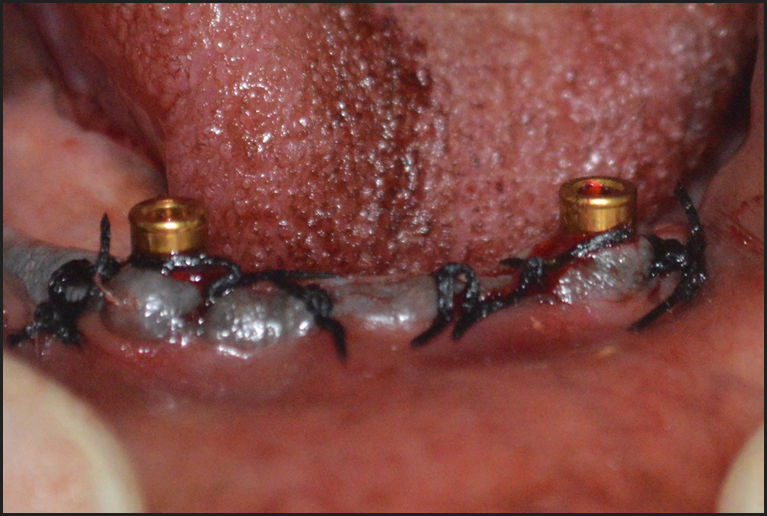
Two implants were placed at lateral regions, using the denture with lead markers as surgical guide, locator attachments were immediately attached. Suturing was done. See Figure 2. Denture loading was immediately done on the same day of implant placement. See Figure 3. Post-surgical instructions were provided and medications prescribed. Patients were recalled after a week for suture removal, occlusal and masticatory analysis.

._a_very_large_force_is_seen_on_toot.jpg)
Bite Force and Muscle Activity Analysis After Loading
After a thorough examination of the surgical site and the implants with the components, T-scan III and EMG recordings were done on implant-supported overdenture.
Part III
Bite Force and Muscle Activity Analysis During Follow-up
After six months the patients were recalled for follow up and the denture was again re-evaluated. Attachments and surrounding soft tissue were examined. T-scan III and BioEMG recordings were conducted on implant-supported overdenture. Occlusal calibration was done wherever it was required.
The T-Scan III & BioEMG Recorded the percentage of the bite force in microvolts in three different intervals for all the ten subjects, which forms the basic data of the study.
The data was subjected to statistical analysis using rANOVA (repeated measures analysis of variance) and Student’s paired t test and presented in the form of tables.
RESULTS
With the CD, a significant imbalance in the force distribution between the right and left side of the jaw, which was brought to balance with occlusal calibration using the above-mentioned technology and that was well maintained with the IOD even after six months follow up. There was a significant increase in the relative bite force in the posterior segment from the transition from CD to IOD. And there was a significant increase in the muscle activity after six months follow up with the IOD.
Evaluation of Bite Force in the Conventional Complete Denture
The bite force was measured in three intervals. First recording was done with the conventional complete dentures. T-Scan III measured the bite force for the right and left side of which the mean difference was evaluated. With every recording occlusal calibration was done. At the first recording with the conventional denture, it showed a significant imbalance between the right and left sides as shown in Table 1.
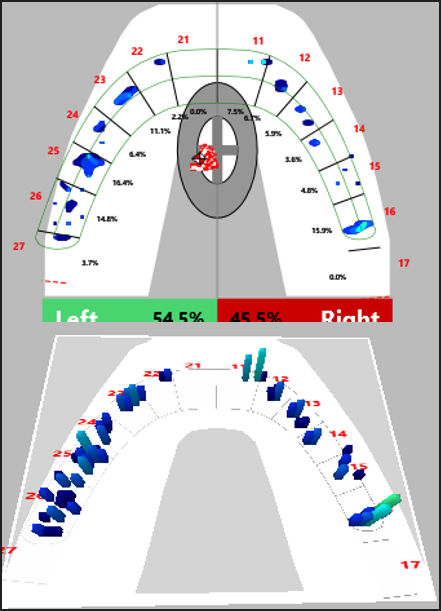
The force load on the left side was 60.2% with a high friction load on the number 25 tooth. On the right side the total force load was 39.8%. The force was diverted more towards the left side. With occlusal calibration and the elimination of the occlusal discrepancies the force distribution was brought to balance between the left and right sides; 54.4% and 45.5% respectively as illustrated clearly in Figure 3.
Figure 3 showed that there was an increased bite force on the anterior segment (top image) for the CD. A significant imbalance of force distribution between the sides prior to T-Scan on IOD (bottom). Final T-Scan III recordings of the same patient is illustrated clearly in Figure 4.

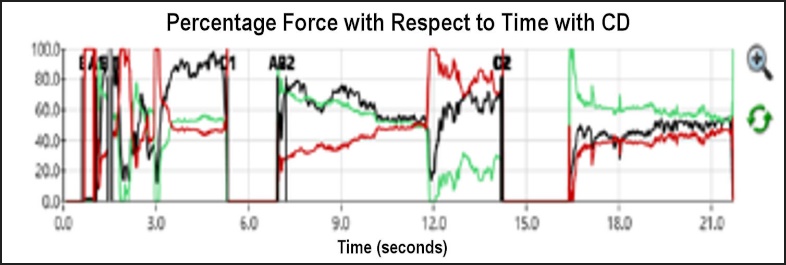
The graphical representation seen on Figure 5 shows the intensity of force against time. The green line represents the total force on the left side, the red line represents the total force on the right side. And the black line represents the total force (Force Line). With the conventional complete denture, the force was exerted more on one side than the other. The lines appeared to be more irregular with increase in the distance between the red and green lines and they did not run parallel to each other. This indicates the lack of balance of the force distribution between the right and left side and more occlusal imbalance. However, after occlusal calibrations the balance was improved and the lines became more even and smoother. See Figure 6.
_and_right_(red)_forces_rather_unstable_with_cd.jpeg)

Evaluation of Bite Force on the Implant Supported Overdenture
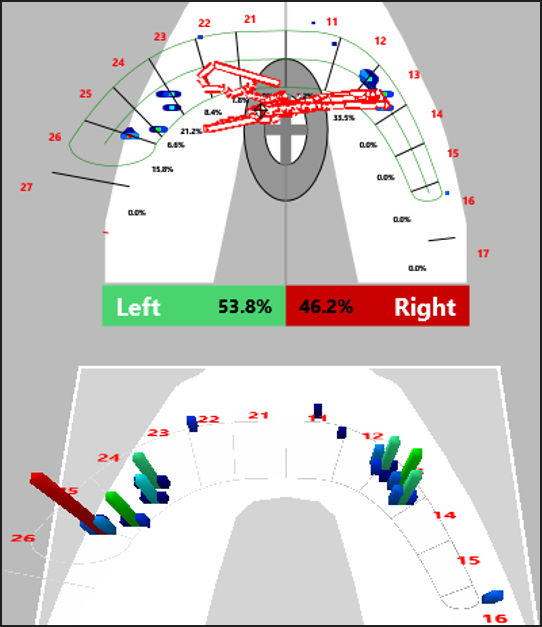
With the implant supported overdenture the balance achieved was well maintained. The 3D presentation on the T-Scan III software showed a uniform occlusal contact with the force directed on the center as seen Figure 4.
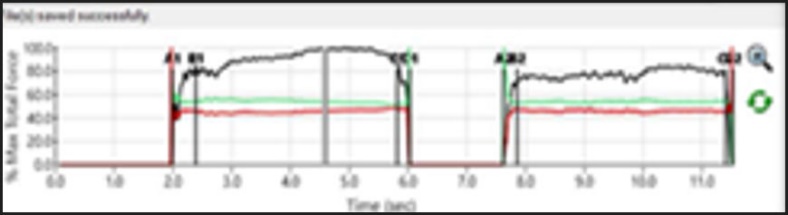
After occlusal calibration and implant placement, the second T-Scan III recordings showed a significant increase of the bite force on the posterior segment. See Table 2. In the graphical presentation recorded by the T-Scan III software the green and red line ran parallel and close to each other, which indicated balance with simultaneous occlusal contact. And the force line appeared to be smoother.
With the reading obtained after six months with the implant-supported overdenture the lines appeared to be even more regular, close and parallel to each other. This indicates the well-maintained occlusal balance with the implant supported overdenture over an extended period of time.
The muscle activity was recorded with bilateral EMG of the masseter and anterior temporalis muscles at pre-treatment, post-treatment and at the follow-up, chewing on both the left and right sides. For both the masseter and temporalis muscles the post-treatment (IOD) activity levels were significantly reduced but recovered fully by the time of the follow-up. See Table 3.
Discussion
For over a century, the accepted treatment for edentulous patients has been to provide maxillary and mandibular dentures that rest on the soft tissues of the alveolar ridges and are not directly connected to them. For many patients, these conventional complete dentures have allowed them to eat, to speak and to function in the wider society more easily than they could without any prostheses. Despite this, it is well recognized that many struggled to use dentures, particularly the lower denture, because of mobility and discomfort, and these difficulties have been shown to be linked with social, psychological and also with functional disabilities, a situation which can deteriorate further as the ridges resorb in height over time.5–7 Kerstein and Thumati conducted a study on force finishing and centering to balance a removable complete denture prosthesis using the T-Scan III Computerized Occlusal Analysis. The study concluded that Force centering of a complete denture prosthesis results in the occlusal forces being directed to eliminate unbalanced side-to-side torquing of the prostheses.7 This desirable prosthesis insertion end-result is accomplished by utilizing the data acquisition and occlusal force display features of the T-Scan III computerized occlusal analysis system. This balanced force distribution improves the tissue seat of the denture by insuring that, while the denture is loaded during mastication, it is seated by the occlusal force summation onto the broadest and most supportive tissue available.
A study was done by Robert B. Kerstein to evaluate the accuracy of using T-Scan III when compared to the use of articulating paper. The study concluded that the marks the articulating paper produces can’t be reliable. And the procedure carried out is completely arbitrary.12
With the reading obtained after six months with the implant-supported overdenture the lines appeared to be even more regular, close and parallel to each other. This indicates the well-maintained occlusal balance with the implant supported overdenture over a period of time. Assunção et al found that Implant-retained overdentures presented increased stress distribution over supporting tissue when compared with conventional complete dentures.13 This finding concurs with the investigation of Sônego et all who stated for the bite force, there was a gradual improvement from the placement of the healing abutments period, which was sustained until the follow-up.14
In the present study it was found that the overall bite force of an individual was increased with the implant supported overdenture when compared with that of the conventional complete denture. A gradual improvement of the bite force was seen in the second visit immediately after the implant placement until the follow up. Statistical comparison (Repeated measures rANOVA) as shown in Table 2 of percent of bite force showed significant increase in the relative bite force on the low side, decrease on the high side.
Comparison of Percent of Bite Force at Three Different Intervals of Both Right and Left Side
Statistical comparison (Repeated measures rANOVA) was made of bite force at different intervals of both right and left side. The mean difference at the pre-treatment recording was 2%, 2.7% immediately after implant placement, and 0.7% at follow up. The significant difference of the relative bite force on the posterior segment, the uniform contact and balanced force distribution with the implant supported overdenture is an important observation of this study. The use of T-Scan III in this study helped in achieving an accurate occlusally balanced prostheses to prevent any extra load, and scientifically supporting a significant difference in the bite force between the conventional complete denture and the implant supported overdenture. This finding is in accordance with many studies using T-Scan III conducted by Kerstein et all.9
Evaluation of Muscle Activity of the Conventional Complete Denture
EMG is a surface electromyography unit that evaluate masticatory muscle group at rest and in function. In this study the temporalis and the masseter muscle activity were evaluated in function. The T-Scan to BioEMG III link software synchronizes the clinical data of T-Scan with EMG. Instantaneous alteration in the muscular output was thoroughly determined. The recordings were done in three intervals; first with the conventional complete denture, then after implant placement with implant supported over-denture, finally after a six-months follow up. A significant gradual increase of the muscle activity was noticed in the transition from conventional complete denture to implant supported overdenture even after six months follow up. Statistical comparison (repeated measures rANOVA) showed that the muscle activity of temporalis and masseter changed at different intervals.
Masseter muscle activity
The comparison of EMG of the masseter and anterior temporalis muscles chewing on both the right and left sides was done using paired sample t test as shown in Table 3 for left mastication. The levels were significantly reduced just after IOD insertion, but returned to pre-treatment levels at the follow-up. The amount of effort needed in chewing is mainly determined by the resistance of the bolus, but is also reduce when the patient is tentative.
The muscle activity with the conventional complete denture showed decrease in the activity of all four muscles. The right masseter 27.3 microvolts (μv), and left masseter 26.0 μv. The amplitude of each muscles showed a noticeable lack of symmetry and synergy that indicates the lack of muscle ability. According to Ina von der Gracht et all, edentulous patients with CDs can achieve a greater degree of muscular activity after rehabilitation with implant supported overdentures during clenching and chewing.15
Temporalis muscle activity
The comparison of EMG of Temporalis muscle on both right and left side was done using paired sample t test. With the conventional complete denture, the temporalis muscle activity was observed to be reduced in both right and left side; right temporalis muscle 13.4 μv, left temporalis 37.6 μv. The amplitudes of the muscles showed a noticeable lack of symmetry and synergy.
Evaluation of Muscle Activity of the Implant Supported Overdenture Along with the Follow Up
Masseter muscle activity
With the implant supported overdenture the muscle activity was significantly improved after six-month follow up. The masseter muscles showed the highest activity right masseter 53.3 μv, left masseter 51.6 μv. The muscles’ amplitudes showed better symmetry and synergy. The statistical comparison of the masseter muscle activity at different time intervals showed a slight non-significant increase in the left side after 6 months follow up. The mean difference of right masseter muscle activity before implant placement; with the conventional complete denture was 3.9 μv and immediately after implant placemen the mean difference was 7.5 μv. after 6 months follow up was 11.4 μv. The Von Der Gracht et all study compared the muscle activity between fully edentulous patients with implant overdentures and a fixed dental prosthesis to subjects with conventional complete dentures and to a group of dentate subjects. They concluded that the edentulous patients with CDs can achieve a greater degree of muscular activity after rehabilitation with implant supported overdentures during clenching and chewing.15 Cardoso RG et all found that the implant overdenture group experienced some statistically significant improvements in masticatory efficiency.16
Temporalis muscle activity
With the implant supported overdenture the activity of the temporalis muscle was slightly increased during the EMG recordings made immediately after the implant placement. The right temporalis showed 16 μv, and left temporalis 36 μv. The activities of the muscles were also significantly improved after six months of follow up; the right temporalis showed 51.9 μv, and left temporalis muscle showed 31.8 μv. The muscles’ amplitudes also showed better symmetry and synergy. Statistical comparison (repeated measures rANOVA) of EMG of temporalis muscle at different time intervals on both right and left side showed a slight increase in the left muscle activity after 6 months follow up. The mean difference of the temporalis muscle activity with the conventional complete denture was 3.9 μv and 17.8 μv on the right and left temporalis respectively. The muscle activity of the temporalis muscle after the implant placement After 6 months follow up the mean value was 11.4 μv and 22.6 μv in the right and left temporalis muscles respectively. The results of this study are in agreement with study conducted by Sonego MV et all found that there was a decrease in muscle activity during rest, during mastication of raisins, and during lateral movements when the overdentures were initially delivered to elderly patients during the adaptation of implant supported overdentures.16 Van Kampen et all stated that temporalis muscle activity was significantly lower when the patient clenched without implant support.14 This study was done to examine the hypothesis; better retention and stability can be obtained with implant supported dentures to improve the oral health with increased bite force and muscle activity.
Conclusions
It can be inferred that as all of these subjects transitioned from Complete Dentures to Implant Overdenture they showed improvements in their bite force as observed with the T-Scan III. Also, there was significant improvement in the muscle activity of each individual, which was evident in the EMG data. We rejected the null hypothesis.
Conflict of Interest Statement
No conflict of interest was reported for this study.
Funding Statement
No source of funding was reported for this study.