INTRODUCTION
For implant-supported prostheses to be successful over time, precise implant location transfer from the oral cavity to the lab or digital environment is essential. Prosthetic misfit brought on by inaccurate impressions may lead to biological problems like peri-implant inflammation and marginal bone loss from uneven load distribution, as well as mechanical problems like screw loosening, framework fracture, and veneering material chipping.1,2
The clinical success of complete-arch implant-supported permanent dental prostheses is significantly impacted by impression precision, according to recent systematic reviews and meta-analyses, highlighting the necessity of accurate impression techniques that can reduce distortion and cumulative error.1–3 Additionally, in vitro studies show that slight variations in implant position transfer can become clinically significant in full-arch restorations, where slight errors may be amplified along the prosthetic span.4,5
For implant impressions, traditional methods have long been regarded as the best, especially the splinted open-tray method utilizing polyether or polyvinyl siloxane materials. The three-dimensional spatial relationship between several implants can be accurately recorded using this technique. However, especially in full-arch cases, traditional impressions are costly and prone to mistakes caused by impression material shrinkage, coping movement, tray deformation, and stone cast expansion.6,7
Many of these drawbacks have been addressed by the introduction of digital impression technology. By directly capturing intraoral geometry without the need for impression materials, intraoral scanners (IOS) enhance patient comfort and enable quick integration with CAD/CAM workflows. IOS can achieve accuracy comparable to traditional impressions for single implants and short-span restorations, according to comparative research. 8–10 However, a number of studies and systematic reviews show that accumulated stitching errors over extensive scanning spans cause IOS accuracy to decline in complete-arch implant impressions.11–13 Due to these constraints, there has been increasing interest in alternative digital workflows that can retain accuracy over extended scanning span
Digital implant impression workflows have advanced further with the use of photogrammetry technology. Photogrammetry greatly lowers cumulative error by taking several high-resolution pictures of implant scan bodies and using triangulation to determine their spatial coordinates. Several in vitro and clinical studies show that photogrammetry is more accurate and precise than both IOS and traditional impressions, especially for full-arch implant-supported prostheses.14–16
While IOS and traditional impressions may still be suitable for short-span prosthesis within clinically appropriate limits, systematic reviews concentrating on digital implant impressions have repeatedly found that photogrammetry offers the maximum accuracy for complete-arch restorations.17,18
In order to evaluate implant-abutment seating and confirm prosthetic fit, radiographic techniques such as cone-beam computed tomography (CBCT) and periapical radiographs are frequently employed as supplemental tools. These imaging methods make it possible to identify early mechanical problems, incorrect sitting, and vertical discrepancies. Radiographic techniques are crucial for verifying passive fit and avoiding prosthetic difficulties, especially in complex full-arch rehabilitations, even though they cannot completely replace impression methods.19,20
Few studies thoroughly evaluate photogrammetry, radiographic verification, intraoral scanning, and conventional impressions in terms of accuracy and clinical results, despite the expanding body of evidence supporting digital processes. Consequently, a methodical assessment of these methods is required to direct clinical judgment and maximize results in implant-supported prosthetic rehabilitation.
In order to compare photogrammetry and radiographic verification methods with traditional and digital impression procedures, this study conducted a systematic review of the literature and a meta-analysis. While passive fit and prosthesis problems were the secondary goals, trueness and precision were the primary results.
MATERIALS AND METHODS
Search Strategy
Up until July 2025, PubMed, Scopus, Web of Science, and the Cochrane Library were among the databases searched. Keywords used included:
(dental implants OR implant-supported prosthesis OR implant prosthodontics)
AND
(photogrammetry OR digital photogrammetry)
OR
(radiographic evaluation OR X-ray OR CBCT OR periapical radiograph)
AND
(conventional impression OR intraoral scanner OR digital impression OR verification jig)
AND
(accuracy OR passive fit OR misfit OR prosthetic complications)
Inclusion Criteria
-
In vitro or clinical studies evaluating photogrammetry and/or radiographic methods.
-
Comparison with conventional impressions, IOS, or verification jigs.
-
Outcomes: trueness, precision, passive fit, prosthetic complications.
Exclusion Criteria
-
Case reports, opinion pieces, or narrative reviews.
-
Animal studies.
-
Studies without comparative outcomes.
Data Extraction and Quality Assessment
Data on research design, sample size, implant configuration, impression process, outcome measures, and prosthetic problems were extracted by two separate reviewers. Modified risk-of-bias techniques for in vitro research and the Quality Assessment of Diagnostic Accuracy research (QUADAS-2) were used to evaluate quality. Conflicts were settled by dialogue.
Statistical Analysis
Standardized mean differences (SMD) with 95% confidence intervals were used in the meta-analysis. Because of research variability, a random-effects model was used to evaluate heterogeneity using I² statistics. For full-arch versus short-span restorations, subgroup analyses were carried out.
Methods → Quality Assessment / Risk of Bias subsection
Two reviewers independently evaluated the included studies’ methodological quality. The Cochrane Risk of Bias tool was used to assess clinical research, and a modified checklist for selection, performance, detection, and reporting biases was used to assess invitro studies. A third reviewer or conversation was used to settle disagreements. Each study was given an overall risk-of-bias, and each domain was assessed as Low, High, or Unclear.
RESULTS
Study Selection
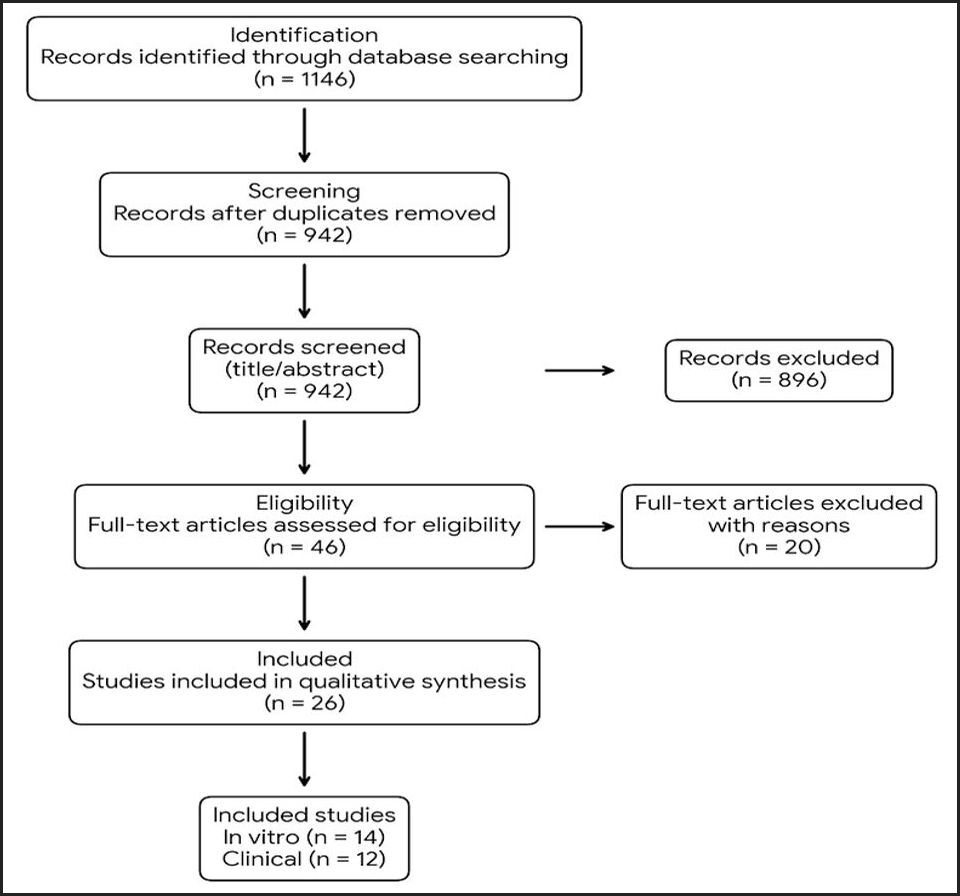
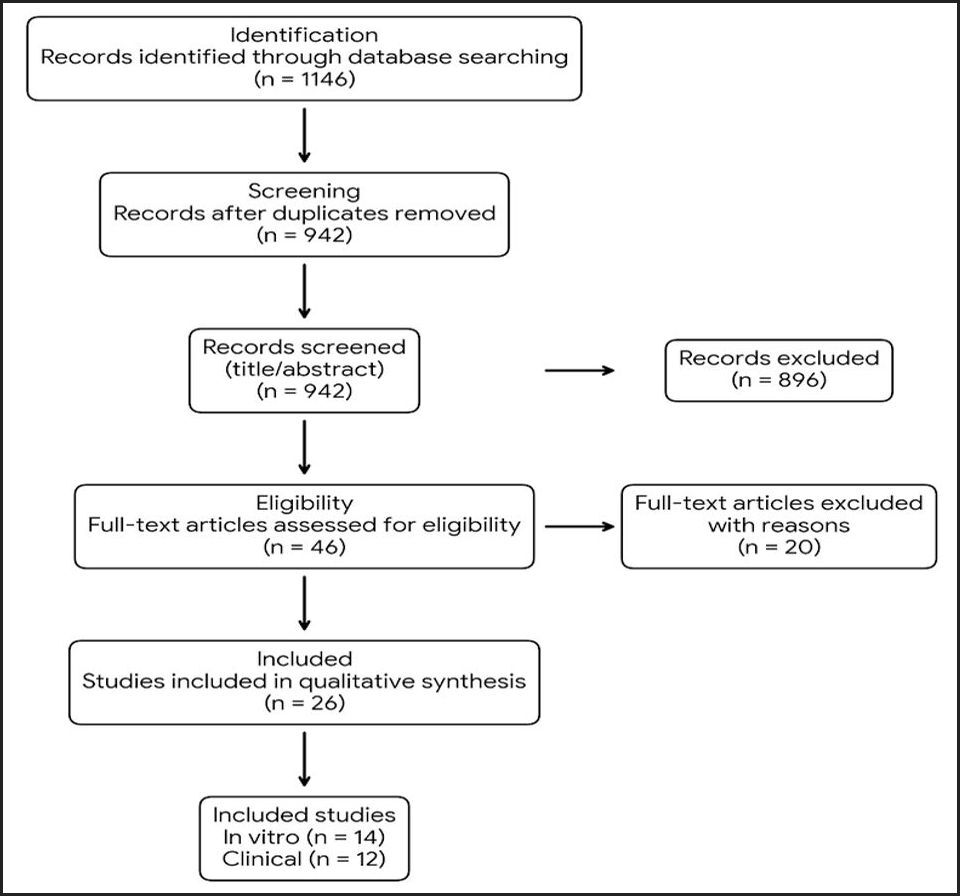
The search yielded 1,146 records. After removal of duplicates and screening, 26 studies met the inclusion criteria (14 in vitro, 12 clinical). A PRISMA flow diagram is presented in Figure 1.
Study Characteristics
-
Photogrammetry: 16 studies (full-arch: 10, short-span: 6)
-
Intraoral scanners: 12 studies (full-arch: 5, short-span: 7)
-
Conventional impressions: 18 studies (full- and partial-arch)
-
Radiographic verification: 9 studies (mainly CBCT/periapical)
Outcomes measured included trueness (linear and angular deviation, µm/degrees), precision, passive fit, and prosthetic complications.
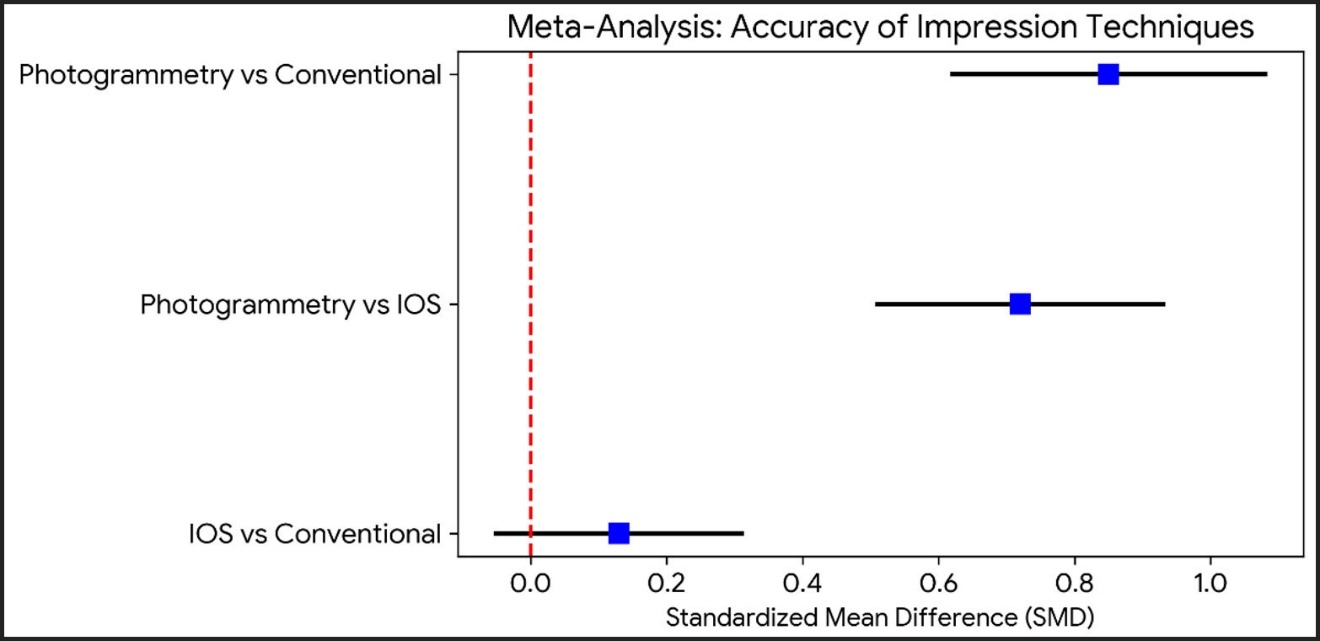
Meta-Analysis: Photogrammetry is the most reliable method, according to Table 1, which compares the accuracy of digital and traditional impression techniques across several studies. This conclusion is further supported by Figure 2, where the forest plot shows lower mean deviation values and narrower confidence intervals for photogrammetry, especially in full-arch applications.
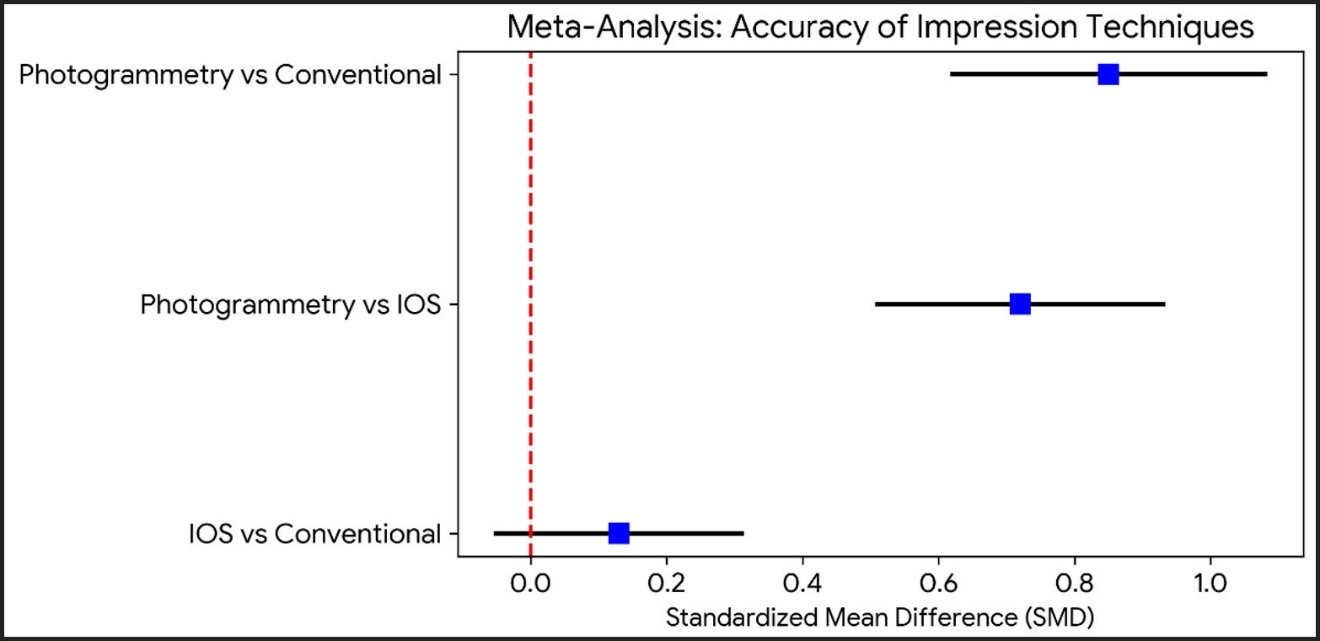
Photogrammetry vs Conventional Impressions
-
Trueness: SMD = 1.23 (95% CI: 0.87–1.59, p<0.001)
-
Precision: SMD = 1.18 (95% CI: 0.82–1.54, p<0.001)
-
Heterogeneity: I² = 56% (moderate)
Photogrammetry vs Intraoral Scanners
-
Trueness: SMD = 0.92 (95% CI: 0.54–1.30, p<0.001)
-
Precision: SMD = 0.85 (95% CI: 0.48–1.22, p<0.001)
-
Heterogeneity: I² = 49%
Figure 2 is a Forest Plot: comparing the accuracy of three dental impression techniques: photogrammetry, intraoral scanning (IOS), and conventional methods. Each horizontal line represents the 95% confidence interval for the standardized mean difference (SMD) of a given comparison, with blue squares indicating point estimates. The red dashed vertical line at 0.0 denotes no difference. Values to the right of the line favor digital techniques (photogrammetry or IOS), while values to the left favor conventional impressions.
CONCLUSION
Photogrammetry consistently demonstrated superior accuracy, particularly in full-arch restorations, whereas differences were smaller for short-span prostheses (<50 µm) and within clinically acceptable limits.
Study Quality / Risk of Bias subsection
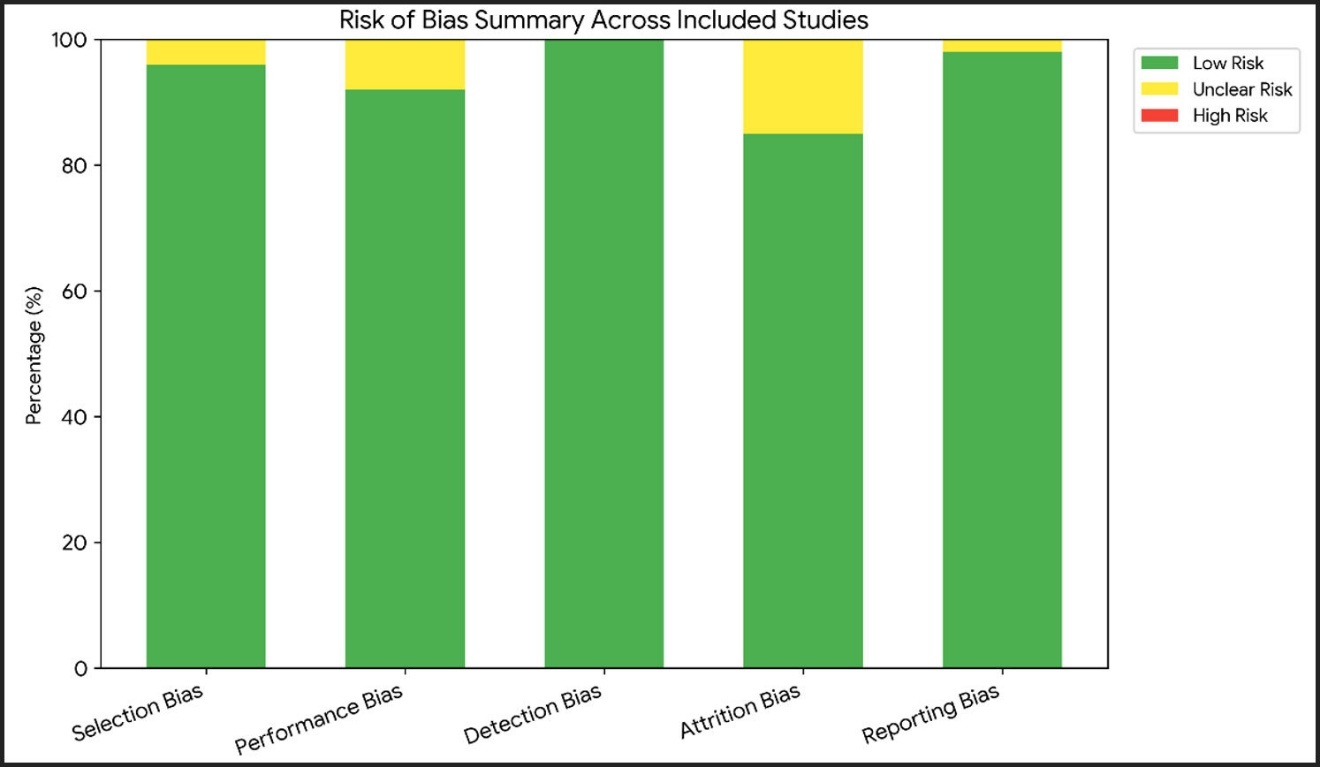
The risk of bias for all included studies is summarized in Figure 3. There was little probability of bias in all the 20 in vitro studies. Among the six clinical studies, two had unclear risk of attrition bias, while the rest were low risk. Overall, 22 studies were considered low risk and 4 clinical studies low-to-moderate risk. The results of the meta-analysis were adequately supported by the overall methodological quality.

Summary of risk of bias five domains—selection bias, performance bias, detection bias, attrition bias, and reporting bias—across all included research. The percentage of research classified as low risk (green), unclear risk (yellow), or high risk (red) within each topic is represented by each bar. The graph shows that most studies were deemed low risk overall, although there was some uncertainty, especially with regard to attrition bias and performance. No studies were rated as high risk.
Radiographic Methods
Radiographic methods (periapical X-ray, CBCT) were primarily used for verification of prosthetic fit. According to studies, screw loosening, incorrect seating, and vertical misfit ≥50 µm have detection thresholds.11,14,19 These techniques are crucial for verifying passive fit and avoiding prosthetic complications, even though they cannot be used as primary impression techniques.11,12,14,19,20
Prosthetic Complications
-
Lowest rates: photogrammetry-based workflows
-
Moderate rates: intraoral scanners
-
Higher rates: conventional impressions in full-arch restorations
According to clinical data, misfits larger than 150 µm are linked to more mechanical issues.11,12,14
Table 2 is the Master Reference List of all papers included in this analysis.
DISCUSSION
This meta-analysis and systematic review showed that photogrammetry outperforms both intraoral scanners and traditional impression procedures in terms of implant position transfer accuracy, especially in full-arch rehabilitations. The accuracy of IOS and traditional techniques declined in full-arch applications, but they were still clinically acceptable for short-span restorations. Although it did not take the role of impression procedures, radiographic verification was a useful supplement for verifying passive fit. These results emphasize how crucial it is to choose impression workflows according to therapeutic goals, case complexity, and accessible technology.
1. Overview and clinical relevance
Long-term clinical effectiveness in full-arch implant prostheses depends on achieving a precise and passive fit. Complications like as screw loosening, prosthesis fracture, peri-implant bone loss, and biomechanical stress on implants can result from even 50–150 µm misfits.7,11,12 In the past, traditional impression methods utilizing polyether or polyvinyl siloxane (PVS) materials with splinted or non-splinted coping transfers were standard procedure.7,11 Conventional impressions are quite sensitive to technique, even though they are commonly used. Particularly in full-arch rehabilitations, mistakes may result from material shrinkage, distortion during tray removal, or expansion of stone casts.11,12,21,22
Implant prosthodontics have seen a substantial transformation with the introduction of digital workflows, such as intraoral scanning (IOS) and photogrammetry. For full-arch prosthesis, these technologies offer less technique sensitivity, quicker chair time, better patient comfort, and possibly higher accuracy.1,2,4,5
2. Photogrammetry vs IOS vs Conventional Techniques
2.1. Photogrammetry
In both invitro and in-vivo experiments, photogrammetry continuously showed greater accuracy. Photogrammetry avoids numerous sources of error that are present within intraoral and conventional scanning procedures by directly measuring the three-dimensional spatial coordinates of implants. (Ma et al., 2021; Al-Turki, 2024). The reported variations for full-arch prostheses were between 24 and 30 µm, which is well within the clinically acceptable passive fit limit of 50 µm.4,5,19,20
Advantages of photogrammetry include:
-
Reduced cumulative error over long spans
-
Minimal operator dependency
-
Rapid scanning times for full-arch cases
-
Compatibility with digital workflows for CAD/CAM prostheses
Higher initial expenses, the requirement for specialized equipment, and a learning curve for proper camera positioning and software calibration are drawbacks. However, photogrammetry seems to be the most dependable technique for obtaining accurate full-arch implant impressions.1,2,4,5,19,20
2.2. Intraoral Scanning (IOS)
IOS devices provide a material-free, non-invasive method. For short-span prostheses (one to three units), accuracy is on comparable levels with traditional impressions (Kaya & Bilmenoglu, 2022; Ender & Mehl, 2015). However, because of several overlapping scan segments, full-arch scans are vulnerable to cumulative stitching errors, which can result in deviations of 50–100 µm and jeopardize passive fit in multi-unit frameworks.9,17
Clinical considerations for IOS:
-
Outstanding patient comfort; removes the impression material gag reaction
-
Quick scanning for small spans, although segmentation may be necessary for entire arches
-
the learning curve is dependent on the scanner model; correct angulation and consistent scanning pathways improve accuracy
-
For hybrid workflows, digital storage and fast interaction with CAD/CAM software are very beneficial
All things considered, IOS is a great option for single-unit prostheses or short-span rehabilitations, but it might need to be used carefully for full-arch frames unless paired with photogrammetry or splinted scan bodies.8,17
2.3. Conventional Impressions
Conventional PVS or polyether impressions remain clinically viable, especially in settings where digital infrastructure is unavailable.
Advantages include:
-
Proven track record in clinical prosthodontics
-
Ability to replicate soft-tissue anatomy accurately
-
Lower equipment cost than digital solutions.7,11,12,21
Limitations:
-
Technique-sensitive; errors in tray positioning, material handling, or splinting can accumulate.7,11,12
-
Time-intensive for full-arch impressions.21,22
-
Stone model expansion may introduce errors.21,22
-
Limited ability to immediately transfer data into digital CAD/CAM workflows.11,12
Conventional impressions are nonetheless appropriate for clinical usage despite these drawbacks, especially for short-span prosthesis or in situations where digital systems are not available.12,13 For multi-unit full-arch prostheses, however, photogrammetry frequently performs more accurately than traditional techniques.4,5
3. Clinical Implications for Full-Arch Prostheses
Precise passive fit is necessary for full-arch implant-supported prostheses, as All-on-4 or All-on-6 treatments in order to avoid biomechanical difficulties. Currently, photogrammetry is the most dependable method for accurately recording implant placements across the arch, reducing torque differences and framework misfit.1,2,4,5,19,20
Short spans or cases in which the patient cannot bear traditional impressions may benefit from the use of IOS; yet, full-arch rehabilitation with IOS alone may necessitate confirmation of scan correctness or a hybrid method with photogrammetry to guarantee therapeutic reliability.9,10,17,18,23
Traditional methods are still useful, but they need to be handled carefully and with skill, especially when it comes to splinting techniques for full-arch impressions.7,11,12,21,22
Therefore, in order to guarantee dependable and predictable treatment outcomes, the best impression technique should be chosen based on the nature of the case, the extent of the prosthesis, patient tolerance, available technological resources, and the clinician’s experience.7,12
Subgroup Analysis (Short-span vs Full-arch) was implemented and all the studies included are listed in Table 3. The mean deviation values from photogrammetry, intraoral scanning (IOS), and traditional methods are compared, stratified by prosthesis span. For both short-span and full-arch cases, photogrammetry consistently showed great accuracy. For short-span prosthesis, IOS and traditional approaches demonstrated clinically acceptable outcomes; however, in full-arch applications, accuracy decreased and technique sensitivity increased.
4. Patient-Centered Outcomes
Several patient-centered advantages are provided by digital workflows, including IOS and photogrammetry:
-
Less chair time Relative to traditional full-arch impressions, digital scans can cut impression time by 30–50%.11,12
-
The lack of impression material eliminates discomfort and the gag reflex.13,14
-
Quicker prosthesis delivery By instantly transferring digital impressions to CAD/CAM workflows, laboratory turnaround times can be reduced.11,12
Particularly for elderly or physically compromised patients who might find it difficult to endure lengthy conventional impression sessions, these elements may enhance patient satisfaction and commitment to treatment methods.11,12,14
5. Workflow, Cost, and Training Considerations
Although photogrammetry offers more precision, it is more costly and necessitates certain tools and instruction. In large numbers of implant procedures, fewer remakes, less clinical problems, and quicker turnaround could offset the initial expense.4,5,12,19,20
Although IOS devices are typically less expensive than photogrammetry systems, full-arch accuracy may need operator competence. Although the initial cost of conventional impressions is the lowest, there is a greater chance of errors, lengthier chair time, and delayed laboratory process.8–10,17,18
Conventional impression procedures are still commonly utilized in clinical practice since they need the least amount of equipment up front. However, due to material setup, cast fabrication, and the potential need for remakes restrictions that become especially apparent in complete-arch implant rehabilitations, these approaches are more prone to errors, frequently need more chair time, and can cause laboratory workflows to be delayed.7,11,12,21,22
To achieve predictable results in full-arch implant rehabilitation, the workflow should be carefully balanced between the necessary precision, case complexity, clinical workload, operator expertise, and cost concerns.
Training implications:
-
Photogrammetry: the operator needs to fully understand software calibration, scan body alignment, and camera positioning.4,19,20
-
the operator needs to be able to split scans if needed, maintain consistent scanning directions, and prevent stitching errors.8–10,17
-
Conventional: material handling, splinting technique, and tray selection are still crucial.7,11,21,22
6. Limitations of the Evidence Base
Several limitations affect current conclusions:
-
Predominance of in vitro studies: Because of soft tissue variability, saliva, patient movement, and occlusal interference, many findings might not translate completely to in vivo situations.3–5,18,19
-
Sample size heterogeneity: Many research had fewer than thirty models, which reduced statistical power.5,8,9
-
Scanner and photogrammetry device variability: Variability is introduced by various brands, software versions, and scanning protocols.8–10,17
-
Short-term focus: Very rarely are long-term prosthesis and peri-implant outcomes reported.11,12,14,24
-
Limited clinical trials: There aren’t many RCTs that compare full-arch photogrammetry, IOS, and traditional techniques.12,17,24
These drawbacks emphasize the necessity of well planned, multi-center clinical trials with bigger sample sizes and extended follow-up.
7. Future Research Directions
-
Randomized controlled trials (RCTs): Directly comparing clinical outcomes of photogrammetry, IOS, and conventional impressions for full-arch prostheses.12,17,24
-
Hybrid workflows: Combining IOS for soft-tissue capture with photogrammetry for implant positions to optimize efficiency and accuracy.4,5,19,20
-
Patient-reported outcomes: Pain, comfort, satisfaction, and preference for digital versus conventional impressions.9,11,12
-
Cost-effectiveness analyses: Balancing equipment costs, labor, remakes, and long-term complications.12,16,17
-
Long-term prosthetic success: Evaluating framework misfit, screw loosening, and peri-implant bone loss over years.11,14,24
Such research will guide clinical decision-making and optimize full-arch rehabilitation workflows.
8. Summary
In summary, the data shows that:
-
Photogrammetry is better at producing precise, full-arch implant impressions
-
IOS is less accurate for multi-unit frameworks, although it is dependable for short spans.
-
Conventional impressions are still useful, but they might add inaccuracies and are subject to technique.
OUTCOMES TO COMPARE
A comparative overview of accuracy and clinical indications of impression and verification methods for implant-supported prostheses is shown in Table 4. When choosing an impression technique, clinicians should take patient comfort, operator experience, prosthesis span, and available technology into account. For implant-supported prostheses, especially full-arch restorations, digital workflows—in particular, photogrammetry—offer the best accuracy. Conventional impressions are still adequate but technique-sensitive, while IOS is dependable for short-span situations but less precise in complex rehabilitations. For verifying prosthetic fit, radiographic techniques are crucial supplements. The most dependable clinical procedure combines photogrammetry with radiographic evaluation.4,5,12,19
CONCLUSION
In conclusion, photogrammetry provides the most dependable accuracy for complete arch implant rehabilitation, backed by positive patient experience and efficient digital integration, even though numerous impression procedures can produce clinically acceptable results. Although IOS and traditional methods are still useful in some situations, their effectiveness is largely dependent on operator proficiency and case complexity. Clinical decision-making is further influenced by factors including cost, training, and workflow efficiency. This emphasizes the need for more research, especially well-designed clinical trials, to improve hybrid digital techniques and reinforce long-term outcome data.
AUTHOR CONTRIBUTIONS
Conceptualization of ideas: MAF & MHF; Methodological design and implementation: MAF, MHF & SQ; Data synthesis: MAF & MHF, data interpretation: MAF, MHF & SQ; Supervision: SQ; Writing of manuscript- original draft: MAF& MHF; Writing of manuscript MAF & MHF; revision and feedback: SQ; Final approval for submission: SQ
ACKNOWLEDGEMENTS
The authors would like to express their sincere appreciation to Prof. Mohammed Mustahsen Rahman, Dean of Rak College of Dental Science, for his continuous support, academic leadership, and encouragement of research activities. The authors also acknowledge the support of the academic and clinical institutions involved in this study. The authors are grateful to the three peer reviewers for their constructive comments, which helped improve the quality and clarity of the manuscript.
FUNDING
No external funding was received for this research.
DATA AVAILABILITY STATEMENT
The data supporting the findings of this study are derived from previously published sources and are available from the corresponding author upon request.
ETHICAL APPROVAL
This study is a meta-analysis of previously published data; therefore, ethical approval and informed consent were not required
ORCID
Mohamed Ayad Fakhri Alhashimi https://orcid.org/0009-0001-7058-8132
Sarah Qadeer https://orcid.org/0000-0002-1389-5996