




Literature Review
Facial Asymmetry (FA) is a universal human characteristic that contributes to individual facial uniqueness. Its’ etiology is diverse, encompassing congenital conditions, acquired pathologies, traumatic injuries, and developmental abnormalities.1–8 The facial musculature consists of numerous subcutaneous muscles that govern facial expression, that are essential to both aesthetic harmony and emotional communication. Alterations or imbalances in muscular activity may result in not only compromised facial appearance but also in functional deficits.9–16 This Case Report describes three patients with unilaterally altered facial asymmetry that developed from longstanding occlusally induced muscular imbalances.
A search of Google Scholar and PubMed using the term “malocclusion-associated facial asymmetry” yielded no published papers. However, the absence of existing literature does not preclude the occurrence of or the clinical observation of this condition. The presented three patients were selected to increase professional awareness of this under-recognized patient presentation, a proposed etiology, and potential treatment considerations.
FA has been observed in patients with functionally displaced mandibles, neuromuscular imbalances, and with Temporomandibular Joint pathology.16–20 Reviews and clinical investigations report that mandibular and condylar asymmetries frequently coexist with Temporomandibular Disorders (TMDs), suggesting that functional disturbances induce adaptive bone remodeling that contributes to asymmetric craniofacial development rather than asymmetry causation resulting from abnormal skeletal gtrowth.15,20–28 Imaging and multivariate analyses have further linked altered condylar position and TMJ internal derangements to asymmetric muscular loading patterns, reinforcing the role that functional factors play in manifesting facial asymmetry.29,30 Further, biomechanical studies demonstrated that functional asymmetric occlusal loading can differentially deform the mandible, providing a plausible mechanistic explanation for progressive asymmetry perpetuating in the presence of a chronic occlusal imbalance.31
Disclusion Time Reduction (DTR) therapy with Immediate Complete Anterior guidance Development (ICAGD) coronoplasty32–34 specifically reduces prolonged posterior tooth excursive movement contacts, which have been repeatedly shown to increase elevator muscle hyperactivity and contribute to muscular TMD pain and functional mandibular shifts.32–34 When recorded with computerized occlusal analysis synchronized with electromyography, prolonged Disclusion Times often occur with asymmetric muscle recruitment patterns from which occlusal timing discrepancies directly influence TMJ loading and mandibular position.32–34
Traditional subjective occlusal assessment methods have been repeatedly shown to be unreliable in identifying these timing-based, prolonged frictional excursive contacts,35–39 which underscore the diagnostic importance of objectively measuring the micro-occlusion when evaluating patients with facial asymmetry. Within the broader clinical framework of TMD treatment, persistent occlusal and neuromuscular imbalances are recognized contributing factors to mandibular displacement and facial asymmetry, supporting the rationale for DTR (ICAGD) as a therapeutic approach that restores functional occlusal symmetry while reducing asymmetric TM joint loading.40
Comprehensive Facial Asymmetry Diagnostic Patient Evaluation
Three adult female patients who presented with near-normal Angle’s Class I occlusions demonstrated clinically obvious, yet different facial asymmetries. All three were referred to the author’s practice after unsuccessful resolution of their ongoing Temporomandibular Disorders symptoms with other providers. Two patients (LM and TA) presented with 28 teeth, while the third patient (TT) presented with 24 teeth from childhood bicuspid extraction orthodontics. And despite each presenting with opposing contacting or nearly contacting anterior guidance surfaces, bilaterally the molars and premolars visibly maintained frictional contact during both right and left excursive movements.41
Each patient underwent a medical and dental history, a comprehensive clinical examination, standardized 3D-CBCT imaging, (Figure 1 & Figure 2) to confirm TMJs were stable and well adapted.


Also, pre-treatment right and left excursive movements for Disclusion Time duration/muscle hyperactivity evaluations, using the synchronized T-Scan 10/BioEMG III technologies (Tekscan Inc., Norwood, MA, USA; Bioresearch Assoc., Inc. Milwaukee, WI, USA). This analysis confirmed each patient’s facial asymmetry presented along with excursive friction and prolonged right and left Disclusion Times (Figure 3). Patients closed firmly into their Maximum Intercuspation Position (MIP), clenched their teeth together for 1-3 seconds, and then completed a single-movement excursion (right or left) until only their anterior teeth were in contact.42 Two (right and left) excursive recordings were made pre-treatment, to more accurately assess each patient’s pre-existing muscle activity levels and Disclusion Time durations.

Standardized digital frontal photographs of each patient were obtained pre and post ICAGD treatment for symmetry comparisons.
After consultation, during which all available treatment options were discussed along with their associated risks and benefits, each patient elected to undergo computer-guided Disclusion Time Reduction (DTR) with ICAGD.43 The 3 patients provided informed consent for ICAGD and authorized that their clinical photographs could be used for research and publication.
Description of the DTR Therapy
The ICAGD Coronoplasty has been described repeatedly elsewhere in definitive detail.32–34,42,44 Briefly, maxillary and mandibular teeth were dried on one side of the mouth, then the subjects closed into their Maximum Intercuspal Position (MIP) with 21-micron thick articulating paper (Accufilm, Parkell, Englewood, NY, USA) interposed between their teeth. Then, each patient excursed right all the way out to the right canine tip and then back into MIP, and then the patient excursed left to the tip of the left canine, and then back into MIP. The pre-treatment T-Scan 10/BioEMG III recordings then guided the author to correctively adjust the occlusal surface ink marks on the prolonged excursive frictional contacts. All posterior working and non-working lateral interferences were completely reduced, and the remaining centric stops were reshaped from broad markings into small pinpoint contacts, located on supporting cusps, marginal ridges and in central fossae. When performed effectively, one side of ICAGD could be completed in 3 passes that obtained definitive visual posterior disclusion. When the first side was completed, the same procedure was performed on the patient’s opposite side posterior teeth.32–34,42,44
ICAGD visit 1 therapy was considered complete when42,44:
-
All lateral posterior excursive interferences and muscle hyperactivity were reduced
-
T-Scan revealed that the Disclusion Times had been measurably reduced to < 0.5 seconds in both right and left excursive movements.32
-
Habitual MIP closure contacts were located solely on cusp tips, in fossae and on marginal ridges
-
T-Scan revealed that patient self-closure into MIP achieved bilateral simultaneous force rises around the arch
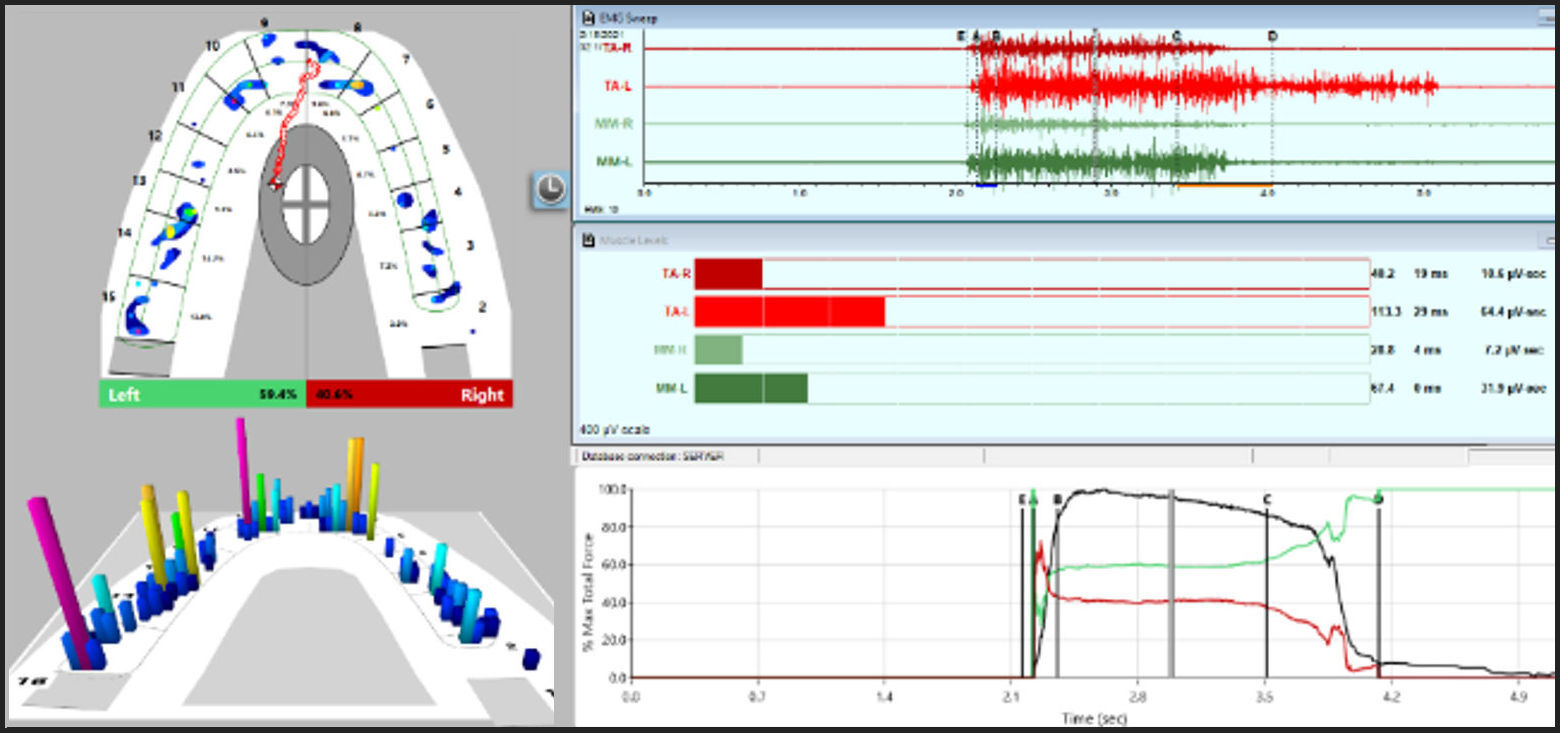
Figure 4 illustrates one patient’s facial asymmetry pre-ICAGD T-Scan 10/BioEMG III data when self-closing into MIP. The muscle asymmetry between the right and left anterior temporalis muscles (upper right pane; red EMG waveforms) and masseter muscles (upper right pane; green EMG waveforms) is readily apparent. The left muscles demonstrate more fiber recruitment than do the right muscles, with the left being the asymmetric side observed in all three patients.

With a similar recording method, post ICAGD recordings were obtained to confirm the Disclusion Times were correctly shortened to < 0.5 seconds/excursion. Patients were seen at day 1, one month, and 4 months to refine and optimize the occlusal force levels, the closure and excursive timings, and the force % balance improvements developed with visit 1 ICAGD. The few months after initial ICAGD allowed for muscular healing and reoxygenation. Post DTR photos were obtained at the same time intervals, except with patient 2 (TA), who shot her own post DTR photos at home.
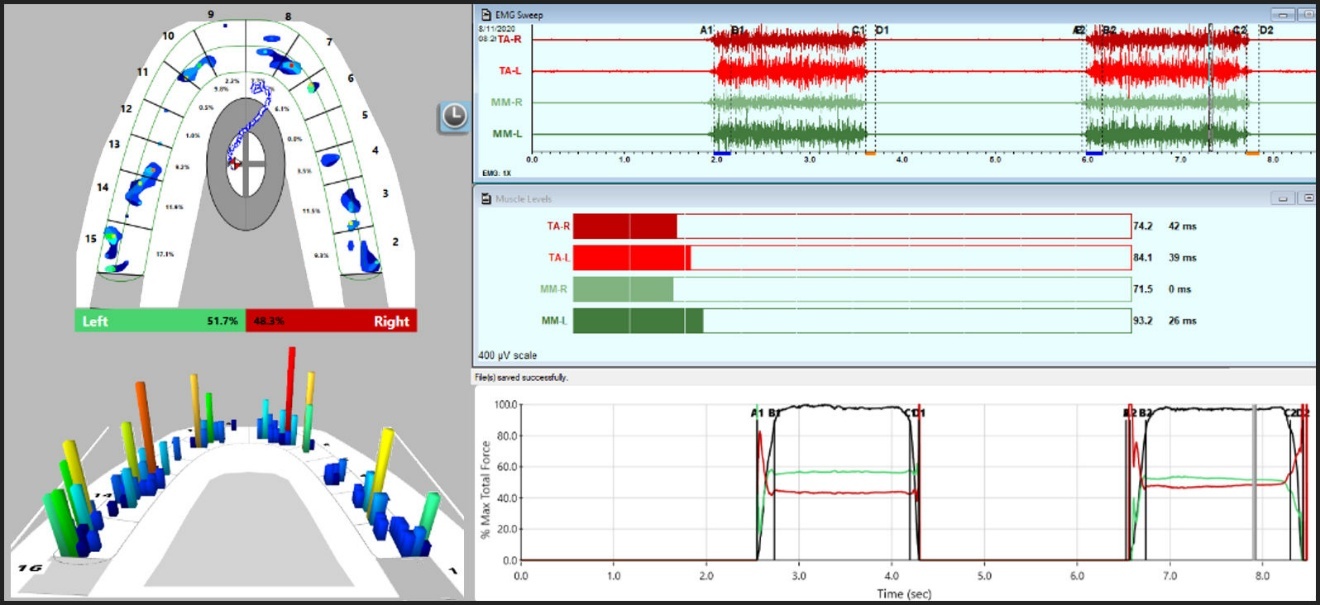
The post ICAGD T-Scan 10/BioEMG III recording (See Figure 5) revealed muscle activity levels became more symmetric compared to those in Figure 4. While not perfectly symmetrical, the patient’s muscles demonstrated a bilaterally stronger, more equal bilateral fiber recruitment, which coincided with the improved right-to-left occlusal force balance (51.7% right to 48.3% left). This was an 82 % reduction in the force imbalance seen preoperatively in Figure 4 (18.8 % reduced to 3.4 %).

Photogrammetric Analysis
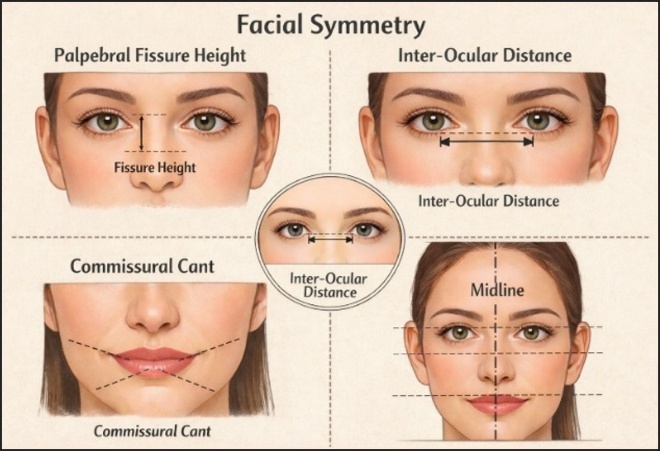
Standardized photogrammetric analysis was used to quantify facial soft-tissue morphology and symmetry (Figure 6). Images were acquired with natural head posture, neutral facial expression, and consistent camera-to-subject distance. Anatomical landmarks were identified based on established craniofacial anthropometric definitions, and linear, angular, and symmetry-related measurements were extracted using validated photogrammetric software.
Palpebral fissure height is depicted as the vertical distance between the upper and lower eyelid margins for each eye, reflecting eyelid position and neuromuscular tone.
Inter-ocular distance is the horizontal distance between the medial canthi, with bilateral comparisons evaluating inter-ocular differences.
The Commissural cant is the angular deviation of the oral commissures relative to true horizontal, indicating asymmetry in perioral muscle activation or skeletal alignment.
Facial symmetry is assessed using a vertical facial midline and horizontal reference lines, enabling visualization of left–right proportionality across the upper, mid, and lower face. Dashed reference lines and measurement arrows indicate the orientation and magnitude of each parameter, facilitating standardized qualitative and quantitative comparisons across subjects or time points (Figure 6).

Photogrammetric validity and reliability were established in prior studies demonstrating strong agreement between two and three-dimensional photogrammetry, and direct anthropometry, laser surface scanning, and stereophotogrammetric reference standards, with reported intraclass correlation coefficients exceeding 0.90 for most linear and angular facial measurements.43,45–47 Measurement reliability was further supported by evidence showing high inter-rater and intra-rater reproducibility for stable craniofacial landmarks, with expected variability in regions characterized by greater soft-tissue mobility, such as the perioral and periorbital areas.46,47
Given the sensitivity of facial soft tissues to neuromuscular tone, photogrammetric methods were selected to allow non-invasive detection of asymmetric and positional change that may reflect altered muscle recruitment patterns. Prior investigations have demonstrated that facial asymmetry indices derived from photogrammetry correspond with functional asymmetries in masticatory and cervical muscle activity, supporting its use in studies examining temporomandibular disorders and neuromuscular adaptation.48–50
Patient 1 (LM)
A 37-year-old female presented with several years of chronic migraines, despite seeking help from multiple health care providers (dentists, an ENT, and her primary care physician who referred her for physical therapy). Pre-treatment facial asymmetry (Figure 7A) was assessed with an open-source software program (OpenFace51 Lake Placid, NY, USA) using two-dimensional (2D) frontal facial photogrammetry. Quantifiable asymmetry was detected in the palpebral fissure heights, an 85% reduced left eye aperture compared to the right eye, a 3.5 mm soft tissue chin point deviation away from the facial midline, and an asymmetric lip posture. Improvements in facial symmetry were seen post-DTR (Figure 7B).

At one-month post-ICAGD, repeat photographs illustrated improved facial symmetry. The palpebral fissure height asymmetry was reduced, with the previously smaller left eye aperture now opened approximately to 96% of the contralateral eye aperture. The soft-tissue chin deviation decreased to 1.2 mm, accompanied by improved resting perioral musculature balance. The patient underwent no surgical, cosmetic, or any pharmacologic facial interventions during the observation period, such that the magnitude and rapidity of the symmetry improvements coincided only with the occlusal therapy that resolved the neuromuscular inflammation responsible for pre-treatment facial asymmetry.
PATIENT 2 (TA)
A 24-year-old female who had completed orthodontics twice, was previously diagnosed with migraine headaches and Temporomandibular Disorders (TMD) and had sought out unsuccessful help from her orthodontist and primary care physician (Figure 8ABC).

The pre-treatment facial photogrammetric analysis detected a unliterally reduced palpebral fissure height, and an 82–85% smaller right eye aperture than the left eye. With the patient at rest, the soft-tissue midline analysis detected a 4.0 mm chin point deviation away from the facial midline, an asymmetric perioral posture, and increased facial muscle tension (Figure 8A).
At four-month post-treatment (Figure 8B), facial symmetry showed measurable improvements. Palpebral fissure height asymmetry was reduced, with the previously smaller eye aperture measuring approximately 92–94% of the contralateral side. The soft-tissue chin deviation decreased to approximately 2.0 mm, and the perioral musculature appeared more balanced at rest.
At six months post-treatment (Figure 8C), further facial asymmetry improvements were observed. The palpebral fissure heights approached symmetry, with bilateral eye apertures approaching 97–99% equivalence, and the facial midline soft-tissue chin deviation lessened to approximately 1.0 mm. Overall, the resting facial musculature appeared relaxed and symmetrical, with improved lower facial balance. No surgical, cosmetic, or pharmacologic facial interventions were reported during the observation period. Again, the progressive nature of these changes over time was consistent with the neuromuscular adaptation associated with the improved occlusal function.
PATIENT 3 (TT)
A 35-year-old female previously diagnosed with left side Trigeminal Neuralgia (TN) and right-side Occipital Neuralgia had been suffering for 4 years, despite seeing a neurologist, an ENT, a chiropractor, an acupuncturist, a massage therapist, and a few physical therapists. She also sought help from several dentists including one who over a 2-year period, made 4 different unsuccessful GneuroMuscular orthotics (GNM).51
Figure 9ABC documents TT’s facial changes from pre-treatment (left), to with a GNM orthotic seated intraorally (center), and following computer-guided ICAGD treatment (right), with the images illustrating progressive facial symmetry improvements from stage 1 to 3.

The Observed Facial Changes Across Treatment Phases are detailed below:
-
Pre-DTR Treatment (A):
Facial asymmetry is visible in the unequal palpebral fissure heights, the mild canting of the commissural line, and the facial midline deviation relative to the interpupillary line. Periorbitally, the soft tissue fullness appears asymmetric, consistent with an underlying neuromuscular imbalance. -
Pre-DTR Treatment with VDO opened GNM orthotic (B):
Partial symmetry improvements can be observed following the increased vertical dimension. The palpebral fissures appear more balanced, and lower facial height was increased. However, residual asymmetry remains, particularly in the middle and lower facial thirds, suggesting there was incomplete neuromuscular stabilization. -
Post-DTR (C):
Facial symmetry has been substantially improved. Palpebral fissure heights appear more equal, the facial midline aligns more closely with the interpupillary line, and the lower facial third demonstrates improved proportionality. Overall, the soft tissue balance indicates reduced neuromuscular strain following computer-guided occlusal adjustments.
Photogrammetric comparisons* of the pre-to-post DTR photographs (excluding the GNM orthotic image) yielded the following observations:
1. There were significant improvements in facial symmetry.
2. Palpebral fissure height asymmetry decreased from approximately 8–10% (≈1.5–2.0 mm inter-ocular difference) to less than 3% (≤0.5 mm) post-treatment.
3. The Soft-tissue facial midline deviation away from the interpupillary midpoint was reduced after DTR by 3–4 mm to ≤1 mm.
4. The commissural cant decreased from approximately 3–4° (≈2–3 mm vertical inter-commissural discrepancy) to ≤1° (≤0.5–1 mm), with concurrent improvements in the lower facial third proportionality.
* All measurements described relative proportional changes rather than absolute craniofacial dimensions, being image-based estimates derived from calibrated two-dimensional frontal photographs.
DISCUSSION
This Clinical Report presents 3 patients all with malocclusion-associated facial asymmetry, whose demonstrated progressive improvements followed computer-guided occlusal therapy. Periorbital balance, soft-tissue midline alignment, and lower facial muscular symmetry both visually and measurably, improved in each patient. Proportional photogrammetric analysis objectively compared facial asymmetry/symmetry across 3 differing time points, which minimized relying on subjectively assessed esthetic facial changes.
A consistent pattern emerged in all 3 patients, where measurable asymmetry in the palpebral fissure heights, in the 15 % - 18 % inter-eye aperture discrepancies, and in 3.0 – 4.0 mm soft-tissue chin deviations, all demonstrated asymmetric reductions following computer guided occlusal therapy, The similar directionality and magnitude of the observed changes were consistent within the 3 patients, suggesting a shared functional causative mechanism, rather than causation resulting from an isolated or incidental variation (Table 1).
The relatively short time frame during which these changes occurred (ranging from 1-6 months) argues against structural skeletal remodeling as the primary explanation. Instead, the changes were more likely resultant from neuromuscular adaptation and altered mandibular positioning following occlusal contact timing and force distribution modifications. Prior studies demonstrated that prolonged posterior tooth contact and delayed anterior disclusion can increase elevator muscle activity and promote mandibular displacement during functional closure, contributing to asymmetric loading of the Temporomandibular joints and surrounding musculature.40,52–62 Reducing the Disclusion Time decreases masticatory muscle hyperactivity and improves neuromuscular coordination, providing a plausible mechanism for the observed facial balance changes.52–62
The periorbital changes observed in all three cases are particularly noteworthy. The facial musculature responsible for eyelid position is highly sensitive to neuromuscular tone and sympathetic input, while asymmetric eyelid aperture has been associated with altered craniofacial muscle activity.63–65 Palpebral fissure symmetry improvements following computer-guided occlusal therapy indicates that the three patients’ facial asymmetry was in part, functionally mediated rather than purely morphologic. Similarly, progressive perioral posture symmetry and chin midline alignment normalization also indicates there was lessened resting state asymmetric muscle recruitment. These findings align with previous studies linking Temporomandibular Disorders, condylar asymmetry, and malocclusion to facial asymmetry, while corroborating prior studies that demonstrated temporal changes followed by computer-guided occlusal intervention.56–71
Unlike orthodontic or surgical approaches that primarily address structural discrepancies, occlusal therapy targets functional loading patterns, the volume of fibers recruited for muscle function, and overall neuromuscular coordination. The improvements observed in these 3 patients indicate that functional occlusal factors likely play a substantial causative role in certain presentations of facial asymmetry, that is often poorly appreciated.
Acute muscular sprain or strain elicits a protective increase in EMG activity, characterized by heightened baseline activation, early motor unit recruitment, and antagonist co-activation.72–77 This response reflects adaptive motor control to pain rather than to muscle weakness. Decreased EMG activity emerges only in chronic or secondary contexts, including central inhibition, prolonged unloading, or neural injury.78–85
The 3 presented patients’ facial asymmetries reflected chronic muscular injury, where its’ evaluation and treatment occurred well after the acute injury phase had been replaced with an ongoing muscular hyperactive condition. Definitive electromyographic changes have been observed in both hyper and hypo functioning masticatory muscles, paralleling the findings of a previously published T-Scan/BioEMG III data-driven Disclusion Time Reduction (DTR) occlusal correction Case Report.78 That report detailed when uniform hyperfunction from chronic injury was detected in the 4 masseter and anterior temporalis muscles, there was a Vicious Cycle Model physiologic response. But when the same 4 muscles were in uniform hypofunction, it reflected a Pain Adaptation Model physiologic response.78 Irrespective of injury response physiology, all three patients presented in this Case Report demonstrated distinct chronic muscular injury adaptation patterns characterized by intermuscular asymmetry.
Although this report describes a small number of patients and measurements were derived from two-dimensional photographic analyses rather than from three-dimensional imaging, standardized photographic protocols were instituted to offset the photogrammetric measurement estimations that can be impacted by head position, lighting, and facial expression. However, the consistency of findings within these 3 patients strengthens the clinical relevance of the observations. The reproducible facial symmetry improvements following computer-guided occlusal therapy require further investigation with multiple patients placed in 2 groups, such that mock ICAGD and real ICAGD can be compared for their facial asymmetry corrective capabilities, while further defining the roles that occlusal forces, contact timing, and neuromuscular imbalances can promote in the clinical expression of facial asymmetry. Future studies should incorporate larger cohorts, objective three-dimensional imaging, and T-Scan synchronized electromyographic data, to better define the relationship between prolonged Disclusion Time, Temporomandibular joint loading, and facial asymmetry.
CONCLUSION
This three-patient Case Report demonstrated that malocclusion-related facial asymmetry can be measurably improved in a short time following computer-guided occlusal therapy, whereby the physical changes progress in a consistent direction. Functional occlusal factors and neuromuscular adaptation contribute meaningfully to certain facial asymmetry presentations, requiring that occlusal force and timing metrics be considered during an asymmetric patient’s clinical evaluation and treatment planning.
Funding Statement
The author received no financial support for the authorship, and/or publication of this manuscript.
Conflict of Interest Statement
The author declares that he has no conflicts of interest regarding the publication of this article.