


INTRODUCTION
Orofacial pain was incorporated into the author’s institutional dental practice in 2010 to provide healthcare to human beings who have been suffering from symptoms, which include headaches, migraines, early morning facial stiffness, trauma to musculoskeletal tissues (muscles, ligaments, tendons), low back aches, nutritional deficiencies, nervous tension, or stress.1 Besides the diverse etiology, occlusal instability has long been considered an important aetiological factor for orofacial pain.1 Occlusal interferences can induce tooth pain, mobility as well as masticatory muscle hyperactivity; although some authors do not believe occlusal interferences to be one of the causes of orofacial pain.2,3 On the other hand, occlusal adjustments have been advocated by numerous authors as a successful treatment modality for orofacial pain.4–7
Occlusal interferences and occlusal surface friction present during excursive movements are contributory etiological factors for occluso-muscular pain and symptoms observed commonly in temporomandibular disorder (TMD) patients. A measurement-driven, computer-guided occlusal adjustment procedure is known as immediate complete anterior guidance development (ICAGD)13 that’s primary therapeutic goal is to measurably decrease the time required for all molars and premolars to disclude from each other (known as the disclusion time) in less than 0.5 seconds during the right and left mandibular excursions commencing from complete intercuspation in maximum intercuspal position (MIP).8–11 The ICAGD enameloplasty is guided by the time measurement capability of the T-Scan III occlusal analysis system (Tekscan, Inc., South Boston, MA, USA), where specific excursive movement time-duration, numerical end-points are achieved to verify whether the enameloplasty was properly accomplished. ICAGD has repeatedly shown to successfully treat myofascial pain symptoms without requiring the treated patient to wear a splint or deprogrammer.8,9,12–14
Shortening the disclusion time with ICAGD is performed with two synchronized occlusal measurement technologies (T-Scan III Computerized Occlusal Analysis System, Tekscan Inc. South Boston, MA, USA; BIOEMG III electromyography [EMG], Bioresearch Associates, Milwaukee, WI, USA).1,15 Together, these two technologies simultaneously record real-time force movies of mandibular excursive movements and the same movement’s-associated masticatory muscle contraction patterns.16 This case report describes successfully treating a patient with chronic occluso-muscle pain who had prolonged pre-treatment disclusion times by reducing them to short disclusion times by performing the ICAGD enameloplasty. Thereafter, the patient’s occluso muscular pain symptoms began to lessen and completely disappear, without the use of any occlusal appliance, deprogrammer, or splint therapy.
Case report
A 30-year-old female patient reported with a chief complaint of pain with her left jaw region and difficulty in complete mouth opening for the past 3 years. The patient had sought several medical consultations during the 3 years, and used over the counter pain medication for pain relief that was not definitive.
A detailed extra and intraoral examination was performed, followed by the patient responding to both a “symptom and frequency scale questionnaire” along with a visual analogue scale (VAS), which indicated the patient’s symptoms were:
a) Severe pain and fatigue in her left jaw without mandibular movement
b) Severe left sided facial tension that was accompanied by temporal headaches, neck pain, and morning jaw pain
c) Severe left TM joint pain accompanied by incidences of severe ear pain and ear chronic noises (tinnitus)
d) Severe difficulty chewing tough foods limiting food intake to soft texture
e) Severe difficulty in opening the mouth wide
f) Severe cold tooth hypersensitivity
g) Very severe, debilitating, throbbing headaches requiring frequent self-medication
h) Very severe light sensitivity, with accompanying nausea
i) Severe upper neck tension or pain accompanied by headaches
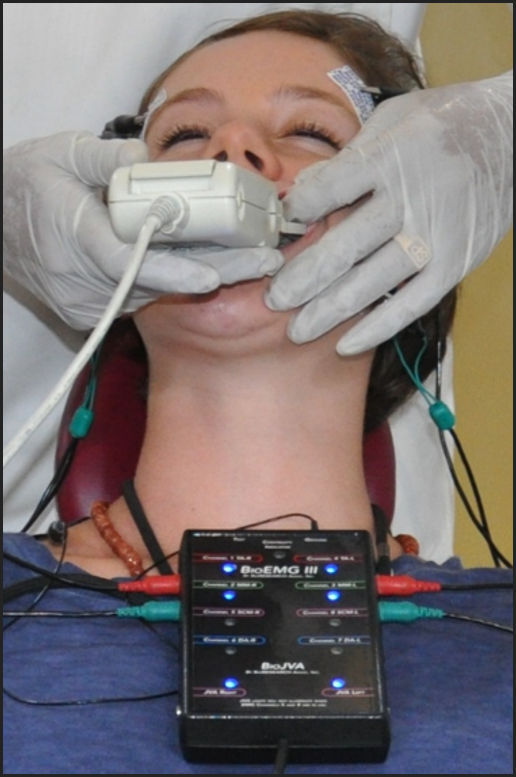
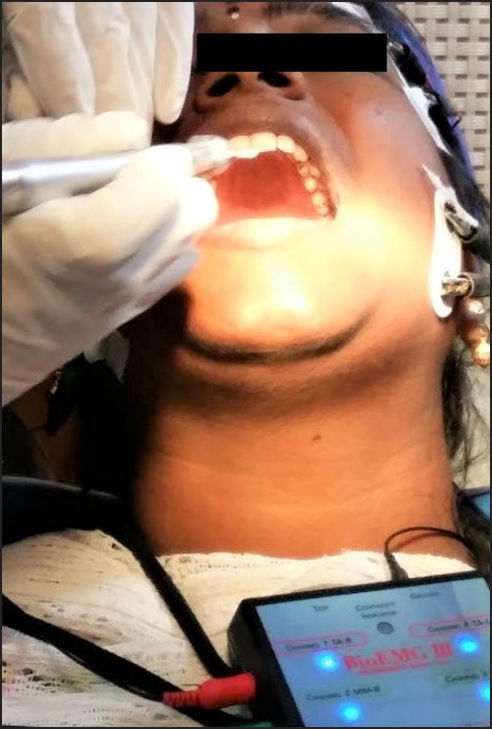
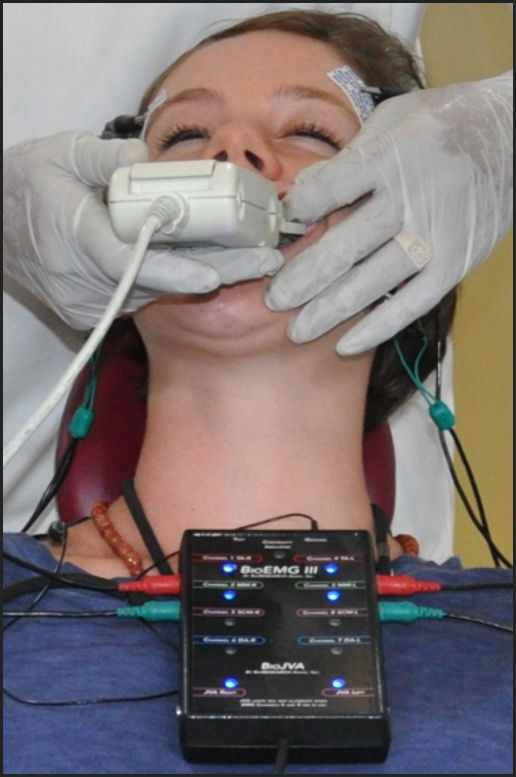
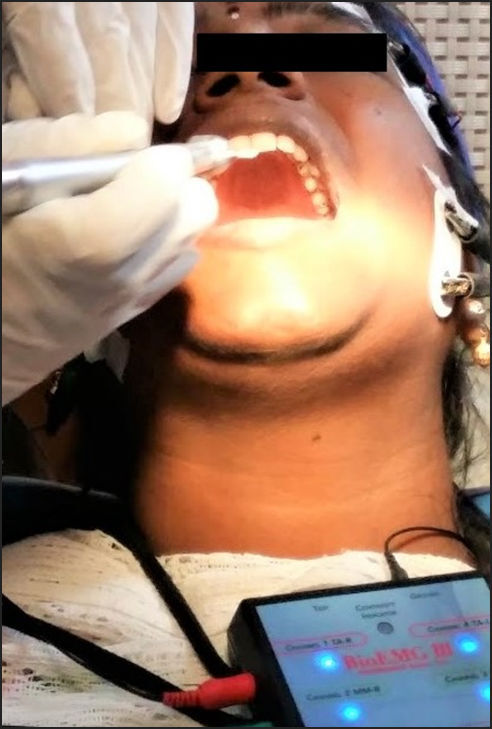
A T-Scan/BioEMG III recording determined her occlusal function and the masticatory muscular contraction patterns related to that occlusal function, to diagnose possible occlusal causation for the reported symptoms. See Figure 1. The patient was asked to bite into the T-Scan sensor after it was inserted it into the mouth. See Figure 2. The sensitivity of the sensor was adjusted to calibrate the sensor for the patient’s bite force range. After the real data was captured when the patient occluded forcefully into the sensor in maximum intercuspation, held MIP for a few seconds and then glided to the left, or right to obtain the Disclusion Time and muscle physiology records See Figures 3 & 4. The assessment determined that the patient had a prolonged left excursive disclusion time of 3.20 seconds, and prolonged right excursive disclusion time of 7.45 seconds. These values were well outside the known physiologic Disclusion Time range (physiologic disclusion times have been shown to average less than 0.5 seconds). Additionally, temporalis and masseter muscle hyperactivity were noted with a prolonged time to muscle shut down in both excursions
_handle__b)_sensor__and_c)_sensor_support.jpeg)


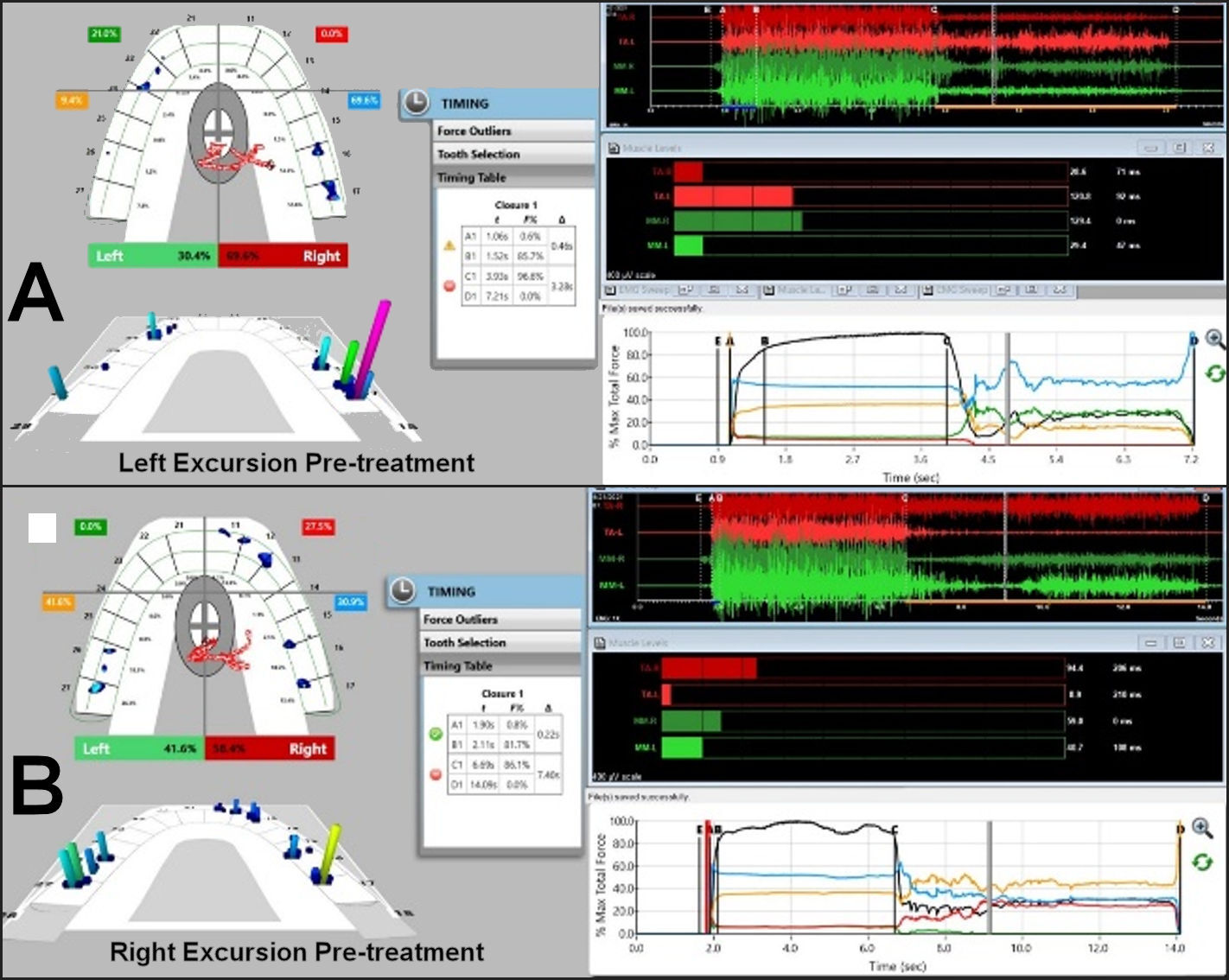
In Figure 5A T-Scan/BioEMG III data showed (left pane), the right posterior balancing forces (#16 green and #17 purple columns) were too forceful for tooth #23 to disclude them. And there was significant excursive muscle hyperactivity in the left temporalis and both masseter muscles (to the right of line C; upper right EMG pane). These 3 muscles contracted for the entire excursion from line C up to Line D. The pre-treatment left Disclusion Time was prolonged = 3.28 seconds (Timing pane).
_pre-operative_left_excursion_disclusion_time_t-scan_emg_iii_data_record._b)_pre-operati.jpg)
In Figure 5B the T-Scan/BioEMG III data record showed many dips in the Total Force line (in the Force vs Time graph; bottom right pane, to the right of line C), indicating there was marked right excursive friction present. In the 2D and 3D Force Views (T-Scan left pane), a right working side group function and left balancing contacts were both present. There was visible excursive muscle hyperactivity in the right temporalis and left masseter muscles (to the right of line C, upper right EMG pane), which worsened as the patient proceeded further into the right excursion. The pre-treatment right Disclusion Time was extremely long = 7.40 seconds (Timing pane).
It was explained to the patient that her disclusion times were too long, which was causing excursive muscle hyperactivity (as detected in the EMG data), which caused her muscular pain symptoms. She was further informed that her pain could likely be reduced or eliminated if she opted to undergo DTR therapy.
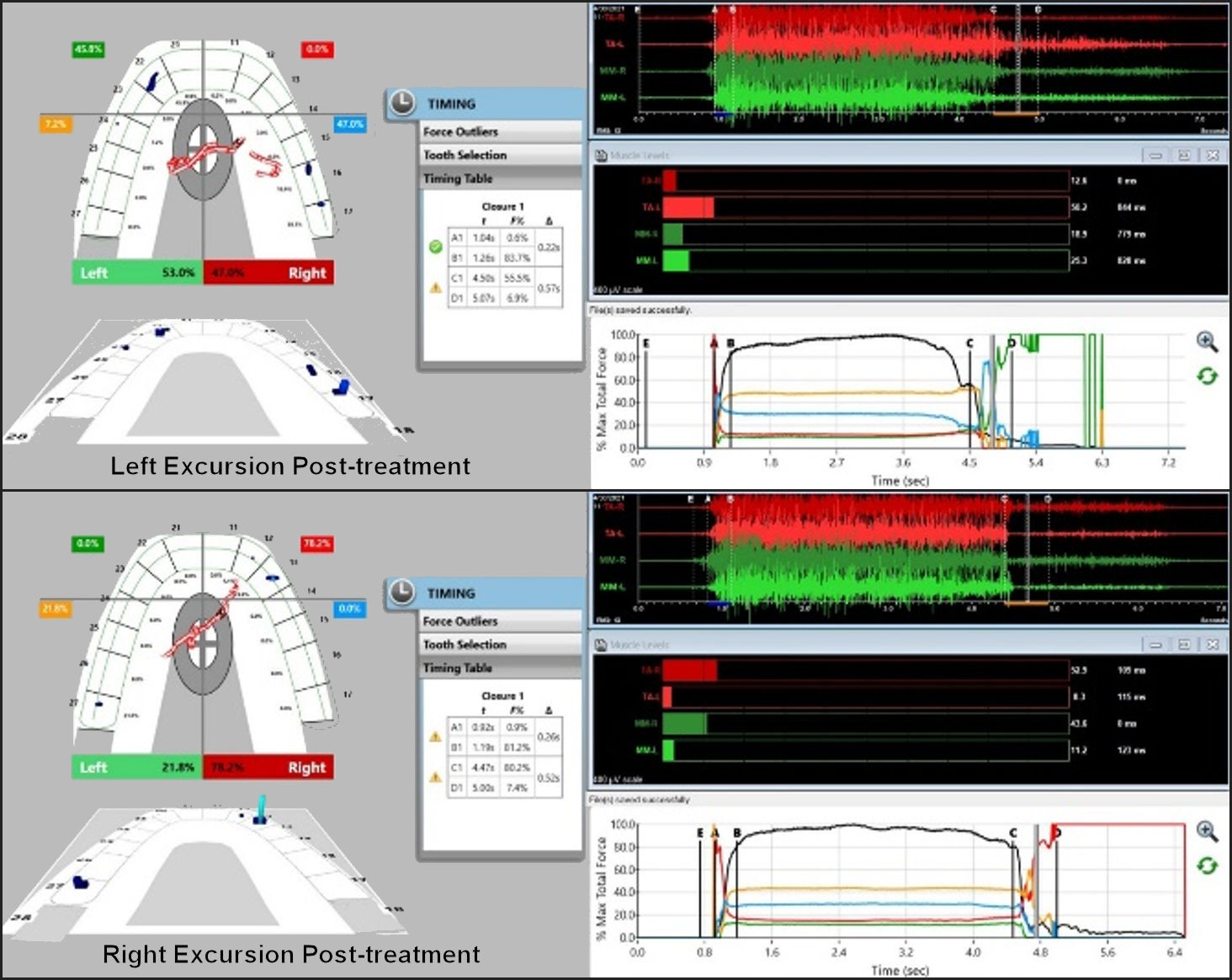
After obtaining patient consent, the ICAGD enameloplasty was performed on her right and left excursive movements to remove the occlusal surface friction and to reduce the DTs to within physiologic durations. See Figure 7A & B. ICAGD enameloplasty corrected the left excursive DT = 0.57 seconds, and the right excursive DT now = 0.52 seconds. When compared with the pre-treatment excursive EMG data in Figure 5A & B, in the post-ICAGD excursive EMG data (Figure 7A & B), the excursive hyperactivity in both treated excursions was markedly lessened from ICAGD.
_left_post-icagd_treatment_excursive_disclusion_time_record._b)_right_post-icagd_excursi.jpg)
Specifically, in Figure 7A the post-ICAGD left excursive Disclusion Time (with T-Scan/BioEMG III) showed markedly less excursive muscle activity to the right of line C than was present pre-ICAGD (See Figure 5A). And the Total Force line (bottom right pane) no longer had visible dips because the excursive friction was removed. The post-ICAGD left Disclusion Time was far shorter than the pre-ICAGD at 0.57 seconds (Timing Pane). And in Figure 7B the post-ICAGD left excursive BioEMG data III showed markedly less excursive muscle activity to the right of line C than was present pre-ICAGD (See Figure 5 B). The Total Force line (Force vs. Time graph, bottom right pane) no longer had visible dips because the friction was removed. The post-ICAGD left Disclusion Time was far shorter than the pre-ICAGD = 0.52 seconds (Timing Pane).
Further, the time to muscle shut down of both working temporalis and masseter muscles was drastically shortened after ICAGD. At the one week follow the patient re-answered the “symptom and frequency scales” which concluded that the severe episodes of jaw pain and fatigue, the temporal headaches, the ear pain and tinnitus, and the teeth sensitivity were all reduced to “mild to moderate” down from “severe” and most symptom frequency were reduced from “always” to “occasionally”. The two week follow up revealed only moderate episodes of jaw pain or ear pain, with “no pain” reported in the neck region, with only occasional episodes of morning jaw pain or headache. At the one month and six month follow ups, the patient reported being content and completely symptom-free.
DISCUSSION
The role of occlusion in instigating myofascial pain symptoms has long been debated. However, some authors have shown occlusal adjustments to be a successful treatment modality for these muscular disorders.6,7,16 Lengthy disclusion time has been shown in several EMG studies to elevate excursive muscle activity levels, and that proper reduction of the disclusion time to < 0.5 seconds can reduce the muscle hyperactivity and related myofascial pain symptoms.8,12–20 Several studies have shown statistically significant reductions pre- and post-treatment disclusion times with significant symptom resolution.1,8,9,12–14,16 These studies prove that ICAGD is effective in treating occluso-muscle disorder symptoms by shortening the contraction times of the involved muscles, thereby allowing for ischemia to resolve and painful muscle fibre reoxygenation and fibre healing to take place. The computer-guided treatment approach lessens hyperactive muscles from within the central nervous system, by controlling the molar and premolar periodontal ligament (PDL) and pulpal mechanoreceptors, which synapse directly with efferent motor fibers that contract the masticatory and the Swallow Mechanism muscles.8 The longer the excursive interferences contact, the longer time the PDLs are compressed and pulpal fibres are flexed, resulting in prolonged durations of masticatory muscle contractions.8,10,11,13 By reducing the length of time that posterior occlusal surfaces contact excursively, the volume and duration of PDL and pulpal mechanoreceptors are reduced, thereby interrupting the PDL/pulpal neurologic muscle hypercontraction cycle. Post-ICAGD, the pulp and PDL no longer hyperfunction the involved muscles into a painful ischemic state, allowing for reoxygenation and muscle fiber recovery, leading to symptom resolution.8. In this particular case, the patient who reported with chronic orofacial pain was subjected to T-Scan-guided occlusal adjustment therapy that involved precise contact timing and force correcting closure and excursive adjustments synchronized with electromyographic recordings of four masticatory muscles. Upon reduction of the disclusion times from 2.3 seconds and 7.40 seconds (for the right and left lateral excursions respectively) to 0.57 seconds and 0.57 seconds, the patient’s muscle hyperactivity was reduced to a minimum, hence leading to symptom resolution.
SUMMARY
This case report described successfully treating a patient diagnosed with chronic myofascial pain by employing DTR therapy to develop immediate complete anterior guidance control over the right and left excusive movements. The patient had been suffering from severe left sided occluso-muscular facial pain for over three years. With a comprehensive dental and occlusal examination, it was discovered that there were underlying occlusal elements that required correction, after which definitive improvements were seen in the patient’s symptoms.
The synchronised T-Scan and EMG system determined the occlusal contact time sequencing and force magnitudes, whereby multiple corrections of imbalanced forces were performed in every segment of the dentition. Properly performed ICAGD offers occluso-muscle disorder patients marked physical improvements from occlusally-generated orofacial pain symptoms, when compared to various unmeasured occlusal adjustments.