Introduction
For many years, various etiological factors such as traumatic, bacterial, autoimmune, and occlusal causes were considered for Temporomandibular Joint Disorders (TMJDs).1 Traumatic causes of TMJDs have been mentioned in various literature as a reference to lesions that can occur in the Temporomandibular Joint (TMJ) and includes both hard and soft tissue lesions.1–8 These traumatic events can result from a direct injury as obvious as a blow to the jaw or indirect, such as a sudden and strong dislocation of the mandible or whiplash injury. These injuries may alter the existing balance of the temporomandibular joint (TMJ) and can cause several problems such as effusion, hemarthrosis, dislocation, internal derangement, fibrous adhesion, ankylosis, fracture and limitation or deviation of jaw opening.9–14
When the trauma involves articular disk, it can lead to disc displacement or perforation. Secondary displacement of the articular disk can also occur due to an injury to a ligament as a consequence of trauma. When hard tissue such as condylar head or neck are involved, it might lead to fractures, causing morphological alterations in joint structures, which in turn produces morpho-functional dysfunction15,16 and an altered spatial relationship of the mandibular head within the mandibular fossa of the TMJ. These alterations might also lead to dislocation of articular disc between the two structures, deformation of the shape of the disc, effusion or degenerative changes. These morphological alterations and the spatial position of condyle can now be more precisely observed and studied with the help of diagnostic tools such as Cone Beam Computerized Tomography (CBCT), which is commonly chosen for evaluating bony components. The effect of trauma on the soft tissue component can be studied with the help of Magnetic Resonance Imaging (MRI), being the gold standard method for assessing disc derangements and soft tissue changes.
Objective
The aim of the present study was to identify and measure the spatial relationship of condyle using the cephalometric method on CBCT images in patients with temporomandibular joint traumatism and also to assess and correlate it with MR images from the same patients.
Material and methods
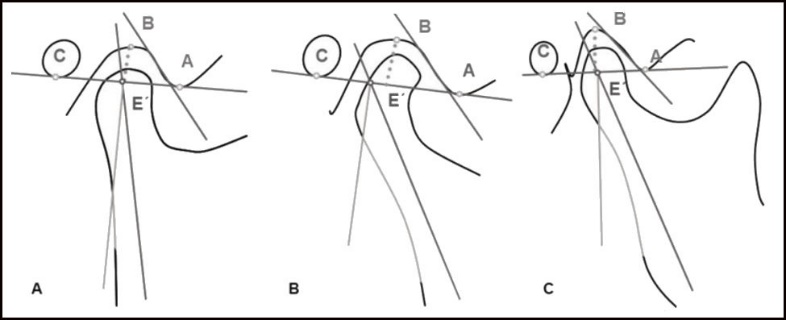
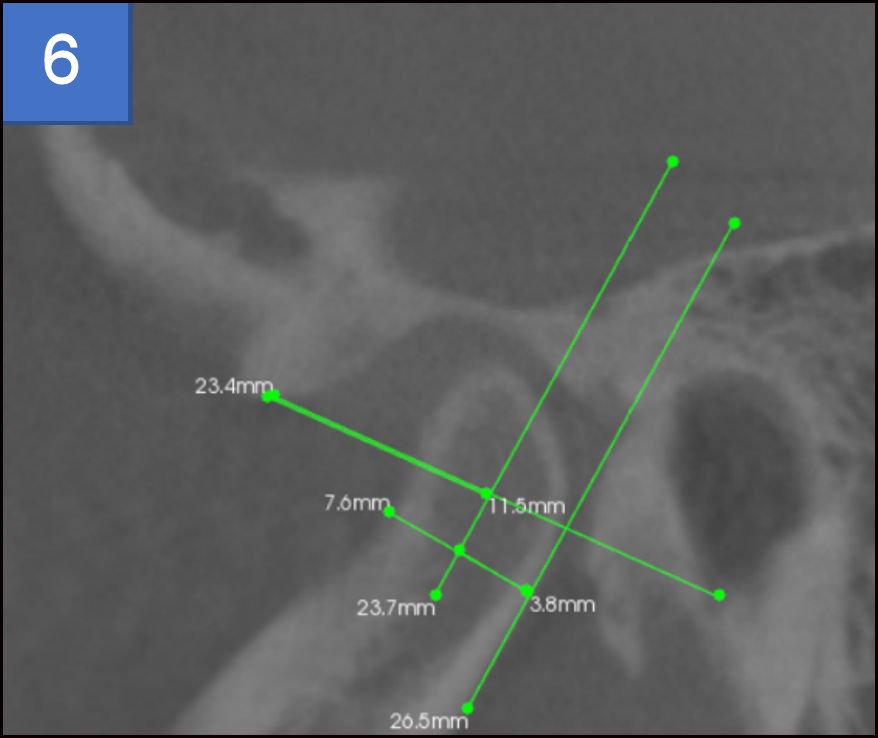
This study included 34 patients, who reported to the Department of Oral Medicine and Radiology, Shri Dharmasthala Manjunatheshwara College of Dental Sciences and Hospital (SDMCDS), Dharwad, Karnataka, India with the complaint of TMJDs along with a historic reference of traumatism in the mandible or TM joint. Patients who had received previous treatments or undergone surgery were excluded from the study. CBCT and MRI were obtained for both TMJs of each patient within a week of the clinical examination. CBCT scans were made with Carestream (Kodak) 9000 machine with exposure parameters of 90 Kvp, 12 mA, 10.8 seconds, with a field of view of 3 x 5 cm. Patients were positioned within the scanner standing straight and were instructed to hold still with their teeth together in maximum intercuspation. All the patients were then encouraged to undergo T-1 and T-2 MRI scans of their TMJs in the open and closed mouth positions with a General Electric (GE) MRI machine of 1.5 Tesla and using dual surface coils designed specifically for the TM Joints. A total of 61 joints were analyzed as independent units (7 joints could not be traced as areas covered during imaging were inadequate for tracing). Anteroposterior spatial relationship of condyle within the mandibular fossa of TMJ was analysed on parasagittal images according to the methodology used in “Application of a Cephalometric Method to the Temporomandibular Joint in Patients with or Without Alteration in the Orientation of the Mandibular Condyle Axis,”17 See Figure 1.

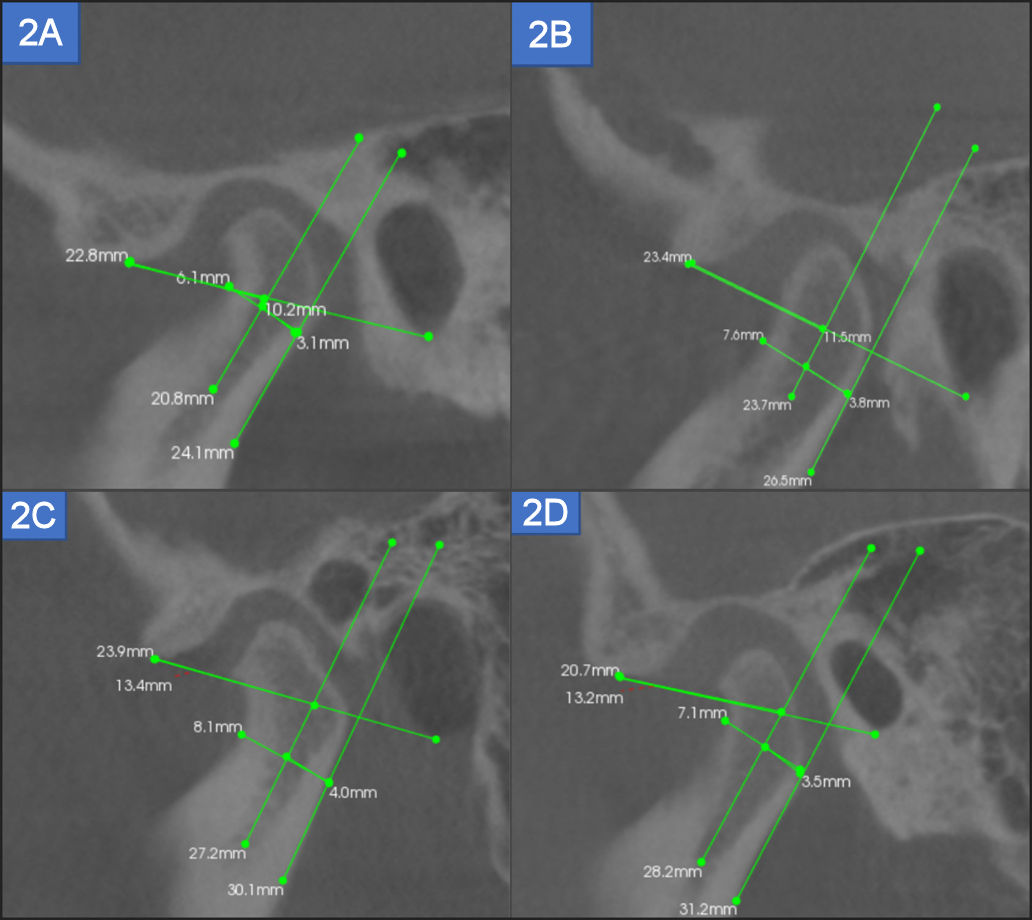
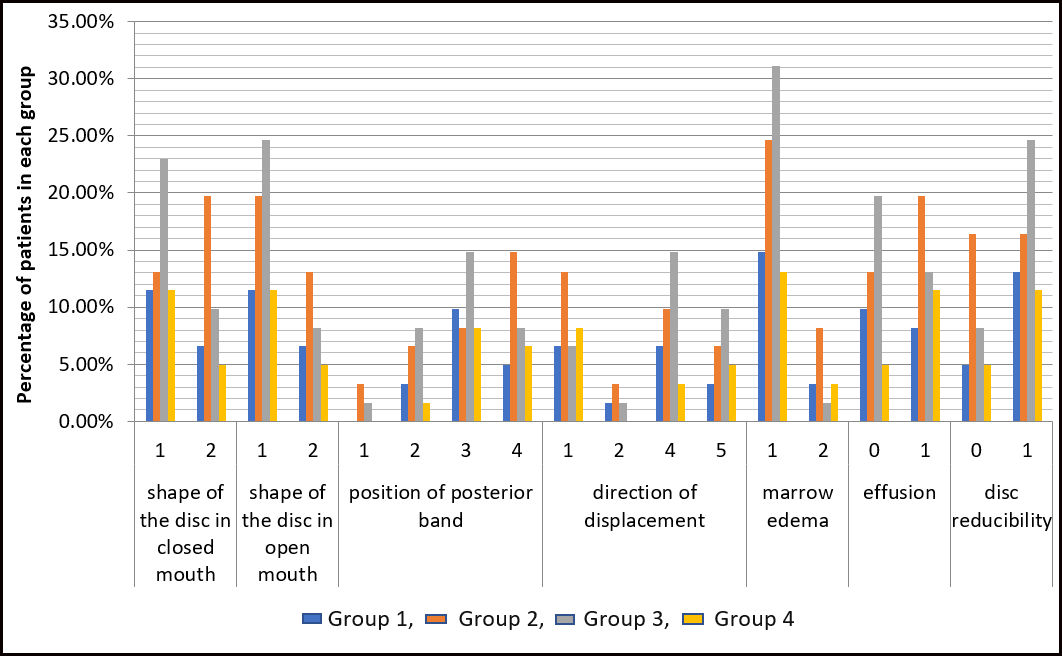
The Anteroposterior Relationship (in %) of total of 61 joints on CBCT were divided into four groups: Group I- <46%, Group II -46-53%, Group III –54-58%, Group IV ->59%. See Figure 2 ABCD. Seven variables on MRI i. e. shape of the i.e., in closed/open mouth, position of posterior band, direction of displacement of disc, disc reducibility in open mouth, condylar marrow edema and effusion were analysed within each group.

Two Maxillofacial Radiologists experienced with interpreting MRI and CBCT scans of the TMJ during their daily clinical practice interpreted all of the CBCT and MRI images. The CBCT interpretations were then correlated with interpretations of MRI images. See Figure 3. All patients provided informed consent and the protocol followed with the World Medical Association’s Declaration of Helsinki.

Statistical analysis
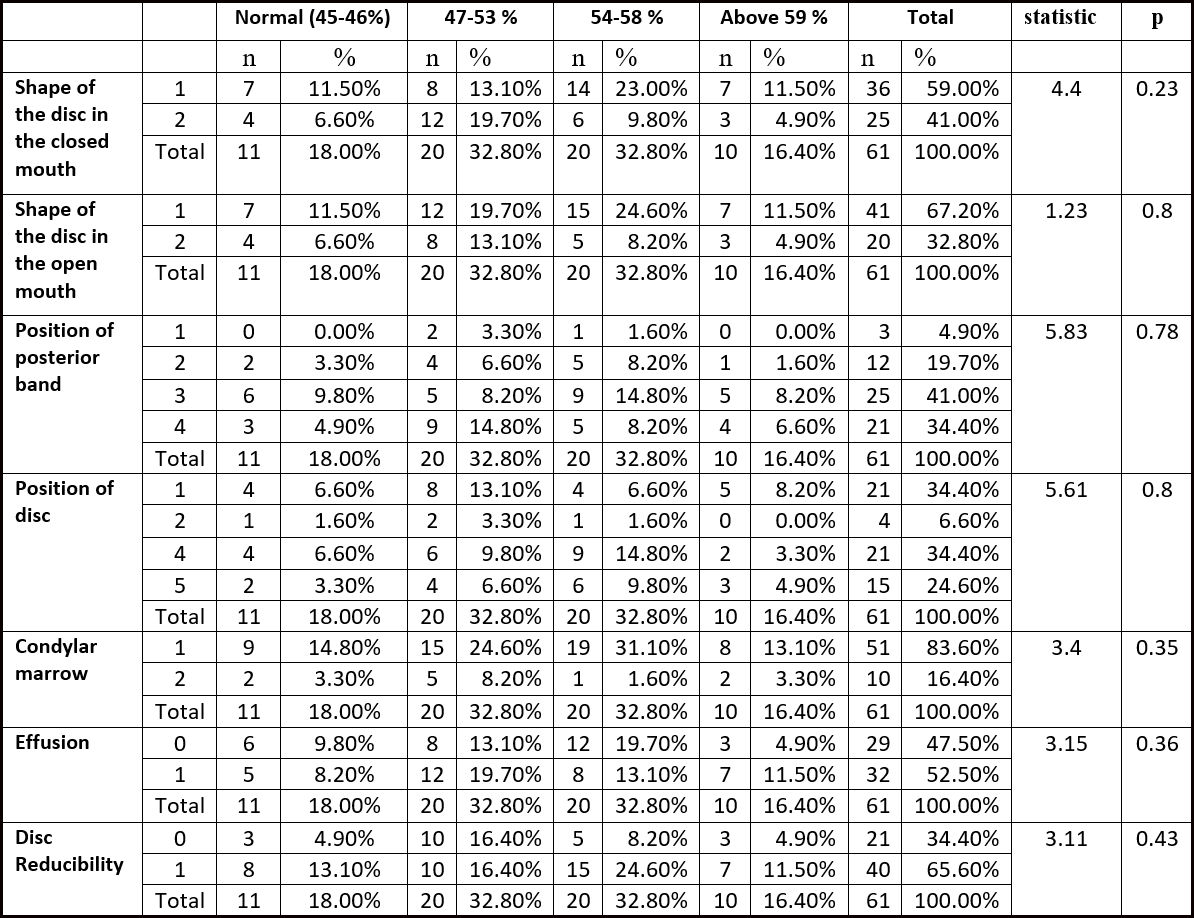
Statistical analysis was performed using a commercially available statistical software program (SPSS 19.0, IBM, Armonk, NY, USA). The correlations between the variables (E.g. CBCT and MRI indications) were explored by using the Fischer’s exact test and the Chi-square test at significance level of P given in Table 2.
Results
In the study, 29 out of 34 (85.3%) patients were female patients with the mean age of 23.1 years. Male patients accounted for another 14.7 percent with the mean age of 22.8 years. A total of 61 joints were analysed and the mean condylar position Anteroposterior relationship was 52.79±5.78 (%). Four groups were formed according to the cephalometric Anteroposterior Relationship: Group I- <46%, Group II - 46-53%, Group III – 54-58%, Group IV - >59%. The numbers of patients in Group 1 to Group 4 were 11, 20, 20, and 10 respectively.
The study demonstrated high frequency of deformed disc in open and closed mouth in Group II followed by group III. See Figure 4 and Figure 5. Partial displacement (identified by position of posterior band) of disc was more in group III followed by group II, while complete displacement was seen more in Group II. See Figure 4 and Figure 5. Maximum discs were displaced either anteriorly or anteromedially. See Figure 4 and Figure 5. Condylar marrow edema and effusion were maximum in Group II. See Figure 4 and Figure 5. Statistical evidence does not support any correlation between the Anteroposterior Relationship and any of the MRI variables. See Figure 4.

_for_different_magnetic_resonance_image_(mr.jpg)
Discussion
Various epidemiological studies have documented greater frequency and severity of TMDs in females.18,19 Most of the patients in this study were females, with male to female ratio of 1:6. This ratio is consistent with previous studies.
Traumatic Intra-articular pathologies of the Temporomandibular joint might involve both hard and soft tissue structures. When it involves hard tissue structure like condylar head, may lead to alterations and manifest as change in shape or position of the condyle. As a consequence of trauma, soft tissue structure such as the articular disk can also suffer a displacement (partial or complete) or a perforation. This could be associated with or without a ligament injury.
Considering the spatial relationship of condyle within the glenoid fossa, according to various studies, centric position of the condyle in the glenoid fossa has been considered an optimal position,20–25 while few authors finds it to be variable.26,27 Hence, alteration in the condylar position in the glenoid fossa may indicate a pathology. A study done by Learreta et al17 on the spatial relationship of the mandibular condyle showed, those joints in a posterior position with alterations in the axis orientation of condyle, had a mean Condylar antero-posterior relationship to be 54.27% as compared to 46.30% in group without alterations in the axis orientation. In the present study, mean of the condylar Anteroposterior relationship was 52.79%. Also, despite having a history of trauma to the joint, only 11 patients i.e. in group I presented with normal antero-posterior relationship of the condyle in the fossa. Rest all the groups had an altered spatial relationship of the condyle in the fossa.
Various studies have demonstrated that patients with asymmetric joint spaces showed some kind of disc disorder, pain or muscle spasms on palpation,20,28,29 while other studies state that, other than trauma to the jaw, potential and significant causes of change in the position of the condyle in the fossa include disc displacement (DD),30 Disc hypertrophy,31 Centric occlusion and centric relation discrepancy at the joint level,32–34 excessive joint effusion,35 and altered osseous morphology of the condyle and eminence due to degenerative joint disease36 as well. This suggests that the position of the disc, (the posterior band of it in particular), has a great bearing on condylar position in the fossa.
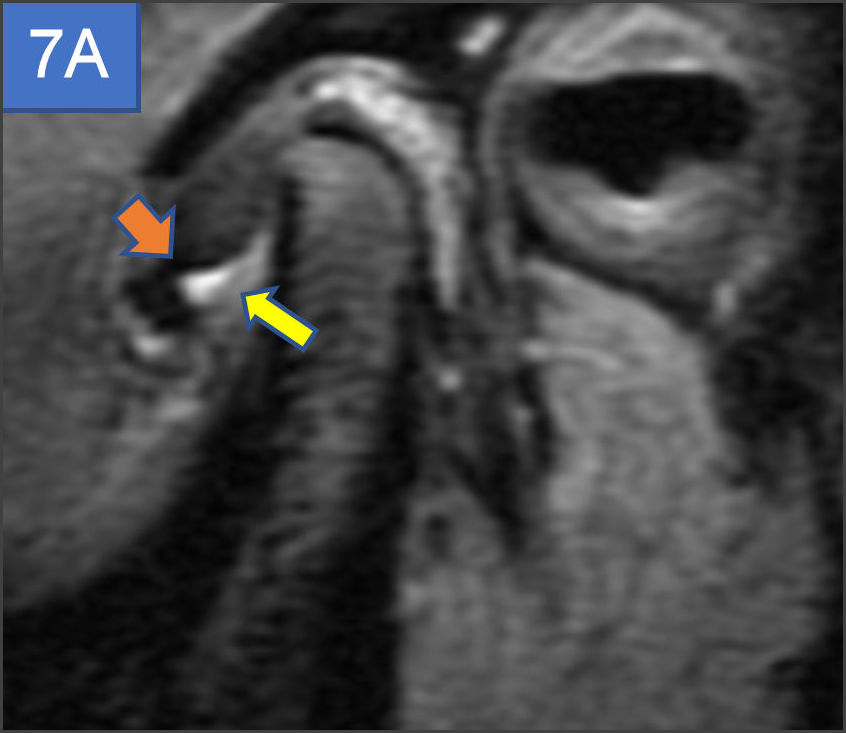
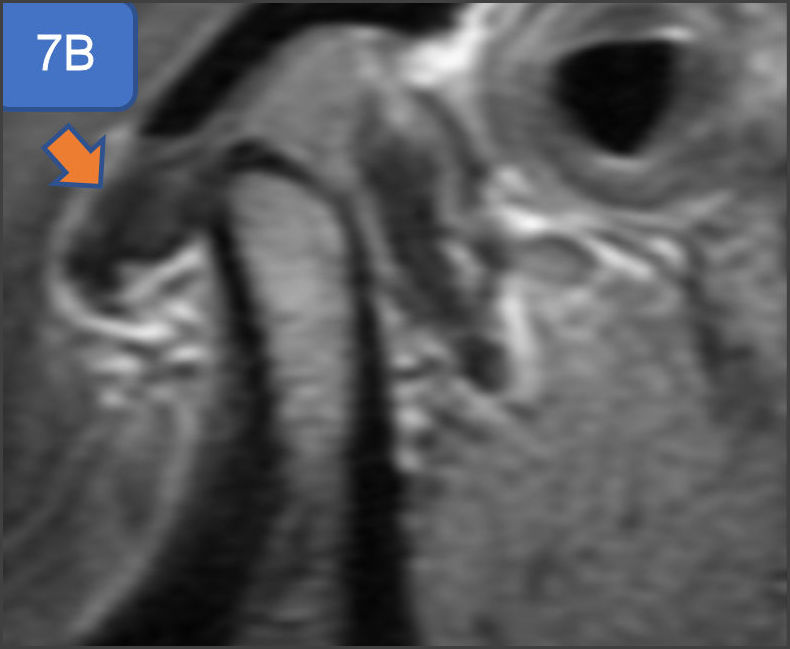
A study done by K Ikeda et al30 which showed that, in case of partial disc displacement(PDD), the condyles were displaced posteriorly in the fossae with a mean anterior space of 2.7 ± 0.5 mm (normal 1.3 ± 0.2 mm) and a posterior space of 1.8 ± 0.4 mm (normal 2.1 ± 0.3 mm). In total disc displacement without reduction (TDDWR), the condyles were displaced not only posteriorly as observed in PDD, but also vertically with a reduced superior space of 1.9 ± 0.4 mm (normal 2.5 ± 0.5 mm). Also, the mean posterior space in case of total disc displacement was further reduced. In the present study, partial displacement (identified by position of posterior band) of disc was more in group III followed by group II, while complete displacement was seen more in Group II (See Figures 6, 7A and 7B) and so was the disc non-reducibility and deformity in open and closed mouth. The inconsistencies in the result might be due to unequal number of joints in each group.

_and_ant.jpg)

Trauma to the mandible can induce joint effusion.37 A study done by Schellhas & Wilkes 35 found excessive joint effusion as an important cause of changes in the position of the condyle in the fossa. In the present study, (32/61), 52.5% of joints with a history of traumatism had effusion on MR Imaging with maximum frequency in group II followed by group III > group IV.
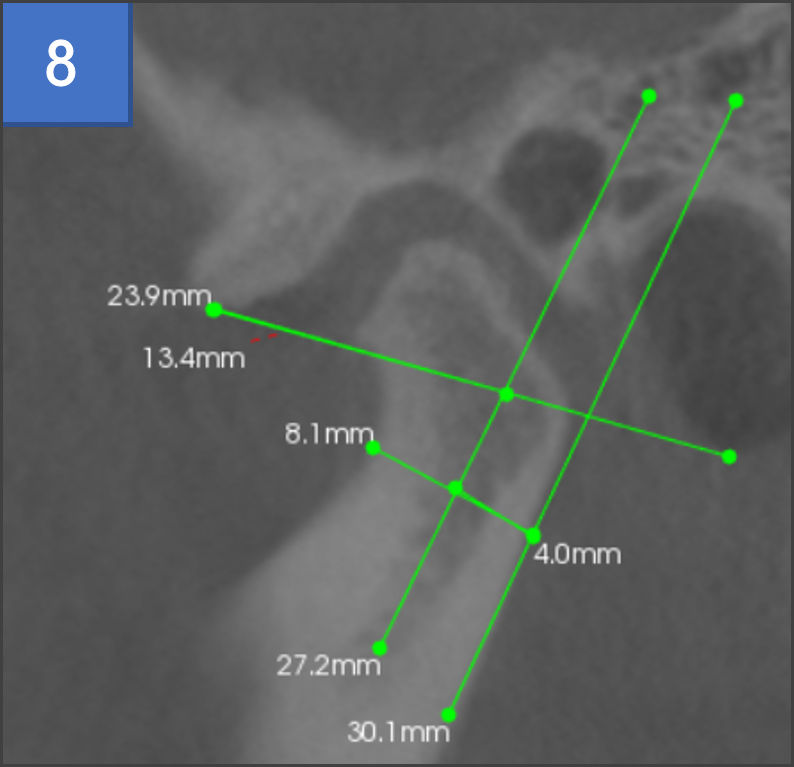
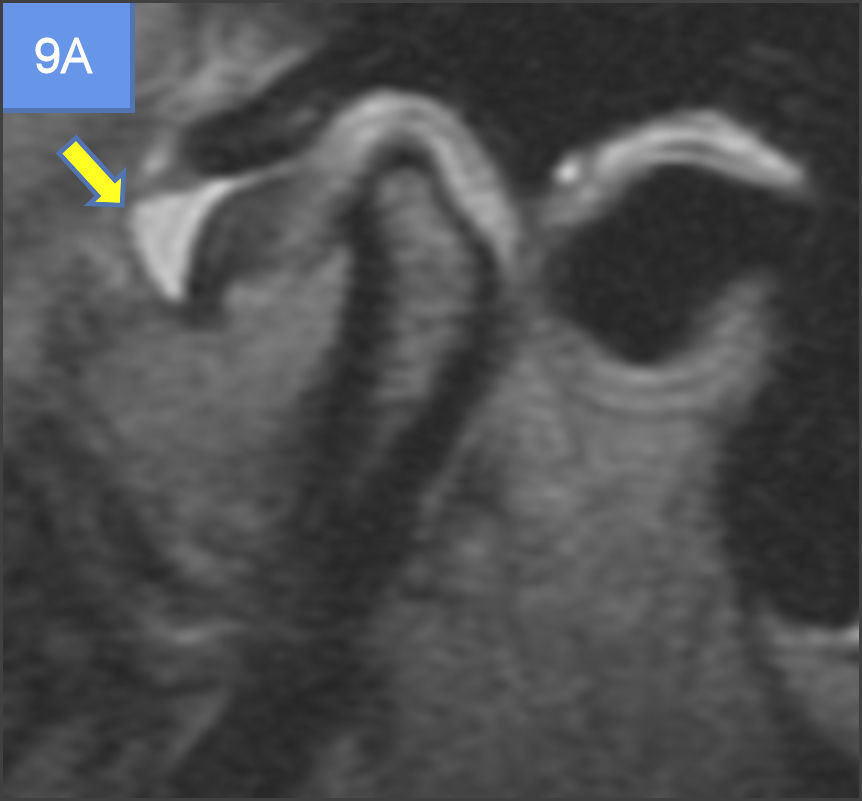
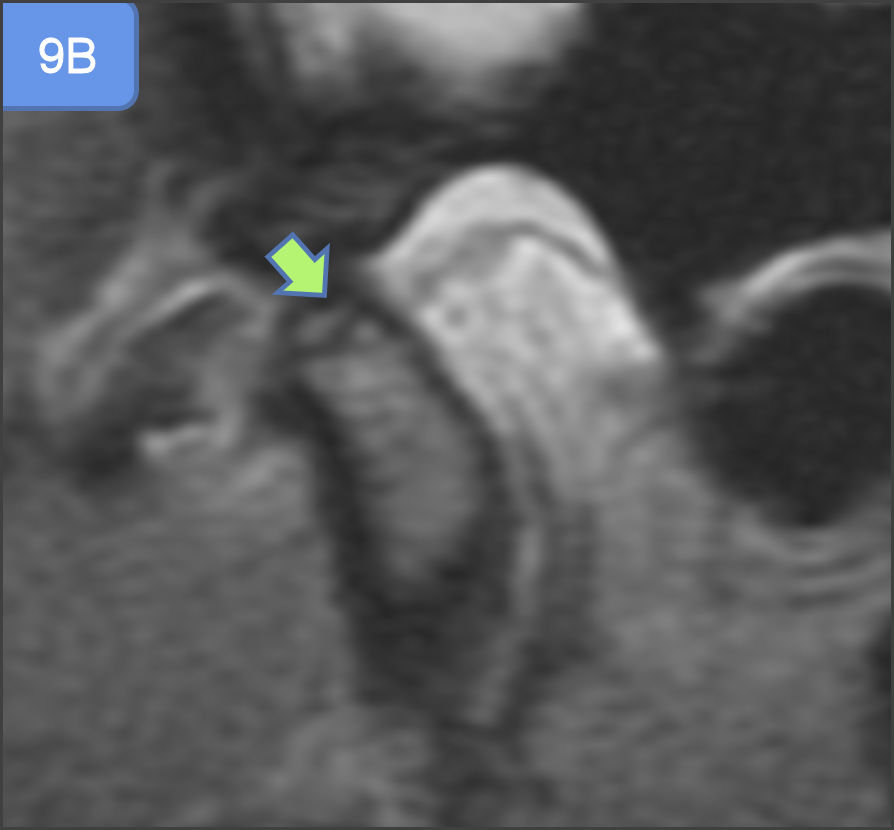
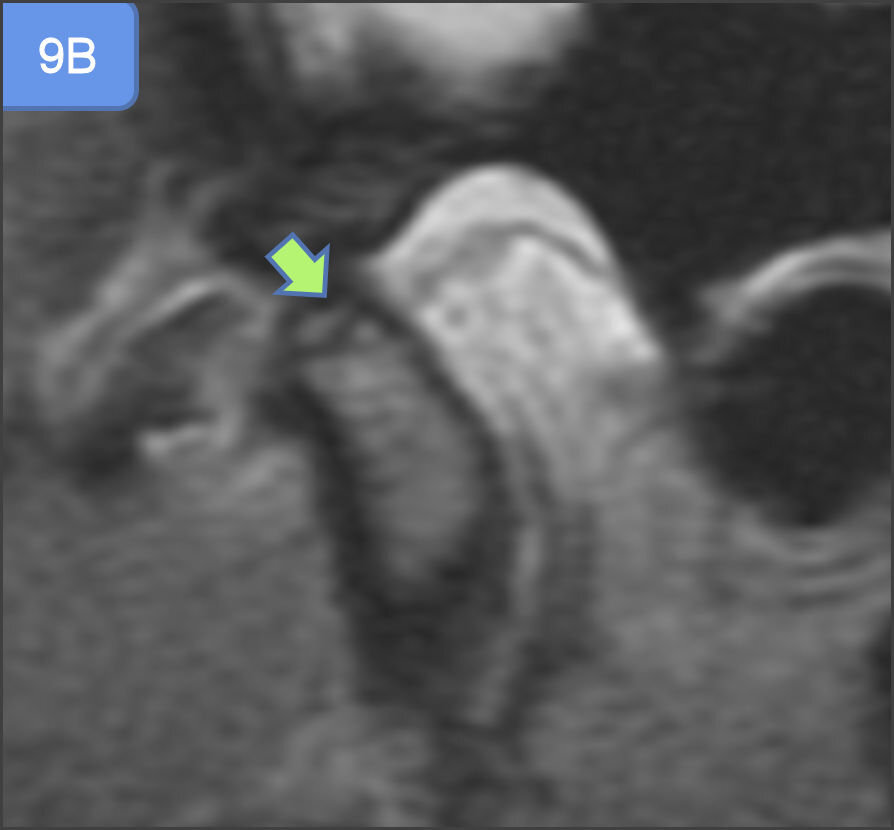
A study done by Emshoff et al,38 revealed, significant relationship between the presence of TMJ bone marrow edema and the MR diagnoses of TMJ internal derangement particularly, disc displacement without reduction and effusion. Although, TMJ internal derangement alone was not always associated with bone marrow edema, it can be present without the evidence of bone marrow edema as well. The association between TMJ bone marrow edema and effusion may be supported by the fact, that the bone marrow abnormalities represent a response to an increased intra-articular pressure in conditions such as synovitis and effusion.39,40 In the present study, Group II followed by Group III (See Figure 8, Figures 9A & 9B) demonstrated highest frequency of bone marrow edema, non-reducibility of disc in open mouth and effusion and hence, was consistent with the findings of previous studies.

_in_supe.jpg)
In the present study, since the CBCT spatial relationship when compared with MR imaging was not statistically significant, it would still justify the need for MR imaging to understand the orthopaedic joint position. As maximum number of patients in the study, presented with an altered spatial relationship of the condyle and had one or the other signs of internal derangement on MR imaging which makes it imperative for the clinician to advice for an MRI scan as soon as they discover an altered condylar axis change on CBCT. Also, clinicians would benefit by understanding the spatial relationship and MR imaging findings in internal derangement cases while planning for complex dental rehabilitation procedures viz full mouth reconstruction, implants and orthodontic corrections.
Limitations
1. The study limitations included a small total sample size and fewer joints in group III and group IV. 2. The sample could have included a more heterogeneous population of TMD patients.
Conclusions
Although, statistical evidence does not support any correlation between the Anteroposterior Relationship of condyle in the fossa on CBCT and any of the MRI variables, the results of this investigation confirm the concept that altered spatial relationship of condyle within the fossa might be related to MRI findings of internal derangement, Osteoarthrosis, and effusion. Patients should be advised of the possibility of the development of osteoarthrosis and osteoarthritis in cases of untreated traumatic TMJ arthropathy.
Statement of conflict of interest
The authors declare no conflict of interest.
Funding sources
No commercial or other funding was received.