
Introduction
Research studies in the areas of speech function and dysfunction have mainly focused on the tongue and pharyngeal soft tissues. Searching PubMed for tongue movements during speech found 1,036 titles.1,2 Searching PubMed for acoustic evidence in speech found 3,080 titles.3 However, there have been limited studies of the jaw motions associated with the speech of normal subjects.4–12 Jaw movement has been compared in stutterers and non-stutterers.4 Yoshioka et al have evaluated the relationship between mandibular movements during speech and specific malocclusions.5 Ostry & Munhall have found that the movements during speech and those during mastication were different.6 In mastication the largest amount of variation appears in the frontal plane, but in speech the sagittal plane normally includes more variation.
Kuwahara et al evaluated the envelope of motion and eccentric movements in normal and malocclusion subjects, suggesting that the analysis of jaw motion has diagnostic value in speech function assessment.7 Ostry et al concluded that local factors, such as muscle mechanics and jaw dynamics should also be considered when evaluating coarticulation along with central control.8 This aspect of speech should be of interest to dentistry because local changes are most often introduced with dental procedures. Burnett & Clifford described significant differences between the envelopes of jaw motions during the speech (containing all of the phonemes (sounds) that occur in the English language) of normal subjects and subjects with incisal wear.9 The paragraph “My Grandfather” is an example of a reading that contains all of the English word sounds.10
Pahkala & Laine-Alava after re-examining 187 children (10 – 15 years of age) with and without articulatory speech disorders and TMD symptoms concluded that in adolescent groups the different orofacial dysfunctions are related.11 Eshghi et al concluded that subjects after complete facial transplantation eventually learn how to move their jaws more effectively for the purpose of speaking clearly.12 This suggests that jaw movements are also an important aspect to developing and maintaining all of the proper acoustic properties of speech.
Methods
Recording of speech patterns was accomplished using the JT-3D incisor-point tracker (BioResearch Associates, Inc. Milwaukee, WI USA), which recorded the motion of a small magnet placed in the labial vestibule. See Figure 1. A previous study using the JT-3D incisor-point tracker found that the presence of the magnet did not significantly disrupt normal speech and that the jaw tracker may be used to study jaw movements during speech."13
Thirty subjects (19 F) were sequentially selected from a database of TMD patients with MRI diagnoses of at least one TMJ internal derangement. Each patient’s incisor-point movements were recorded while reading the “My Grandfather” passage, which contains all of the phonetic sounds of the English language. See Figure 2. A separate age and gender matched group of thirty subjects (19 F) with Joint Vibration Analysis (JVA) recorded bilaterally normal TMJs also had their movements recorded while reading the same passage. All TMD patients and control subjects were informed of the purpose of their recordings and consented. An IRB exemption no. BIRB/101Z/2020 was received.

Inclusion Criteria
-
One or two TMJs with internal derangement
-
The ability to read the English language passage “My Grandfather”
-
Consented to participate in the study
-
TMD patients had at least one TMJ classification of Piper 3a to 5b
-
Control subjects had either bilateral Piper 1 TMJs or at most one Piper 2 TMJ.
Exclusion criteria
-
Any form of a speech impediment
-
Excessively painful TMD symptomology
-
Patients with deep bite occlusion preventing the placement of the magnet in the labial vestibule
-
Patients with open bite occlusion without any anterior tooth coupling
The Incisor-point tracker was applied to each subject and tested for proper alignment with a range of motion recording from centric occlusion to maximum opening. The following sequence was recorded:
-
The subject was instructed to bring the teeth together in centric occlusion
-
The JT-3D motion tracking was initiated
-
The subject was instructed to slide the mandible forward to the edge-to-edge position
-
The subject was instructed return to Centric occlusion,
-
The subject was instructed to go to the rest position
-
The subject was signaled to start reading the passage.
-
After finishing reading the passage, the subject was instructed to return to centric occlusion and then the recording was terminated and saved.
This sequence included centric occlusion as a reference point that the movement could be related to. See Figure 3.

Analysis of Recorded Data
Data were tested for normalcy using the Shapiro Wilk test. In cases where all data were normally distributed Student’s t test was used to compare means. In cases where the data were not normally distributed, the Mann-Whitney U test was used instead. Comparisons were made between the patient group and the control group, and also between the measurements of the male and female subgroups within each group. The measurements evaluated for each group were:
-
Mean age of each group
-
Mean range of motion to maximum open position
-
Mean amount of deflection at maximum opening
-
Mean maximum protrusive excursion
-
Mean vertical extreme point of speaking
-
Mean maximum opening velocity in speech
-
Mean maximum closing velocity in speech
-
Mean most anterior point in speech
-
Mean maximum right excursion in speech
-
Mean maximum left excursion in speech
IRB approval was obtained number BIRB/101Z/2020.
Results
The mean age of the Internal Derangement (ID) group was (34.7 +/- 14.5) years. The mean age of the control group was (36.8 +/- 11.9) years (p = 0.2843). See Table 1.
The range of motion (ROM) of the control group (50.0 +/- 11.9) was significantly larger than the ROM of the ID group (34.7 +/- 14.5). The vertical range of speech of the control group (11.5 mm) was significantly larger than for the ID group (9.6 mm). The mean maximum opening velocity of the control group (88.4 +/- 26.6 mm/sec) was significantly greater than the mean opening velocity of the ID group (68.4 +/- 25.1 mm/sec). The mean closing velocity of the control group (82.4 +/- 20.8 mm/sec) was significantly greater than the mean closing velocity of the ID group (65.1 +/- 25.5 mm/sec). See Table 1.
The mean most anterior point of speech with respect to the centric occlusion position was significantly anterior in the ID group (2.4 +/- 2.4 mm) compared to the control group (1.0 +/- 1.2 mm). The mean length of the right excursions of the control group (10.0 +/- 2.9 mm) was significantly greater than the mean of the ID group (7.8 +/- 2.1 mm). The mean length of the left excursions of the control group (10.0 +/- 2.6 mm) was significantly greater than the mean of the ID group (7.2 +/- 2.4 mm). The mean maximum protrusion of the control group was significantly greater (7.4 +/- 2.2 mm) than the maximum protrusion (5.5 +/- 1.90 mm) of the ID group. Yet the ID speech was more anterior. The extent of lateral deflection at wide opening of the control group was significantly less (1.4 +/- 0.9 mm) than the lateral deflection (2.4 +/- 1.8) at wide opening of the ID group. See Table 2.
Discussion
Tables 1 & 2 describe both the characteristics of the speech pattern and contrast the mobility of the TMD patients compared to the mobility of the control group. As expected, the range of mobility of the TMD group was reduced when compared to the control group likely due to limitations in the condylar translations. When the limitations of condylar translations observed were unequal bilaterally a deflection was recorded at maximum opening and different left and right lateral excursive ranges were found.
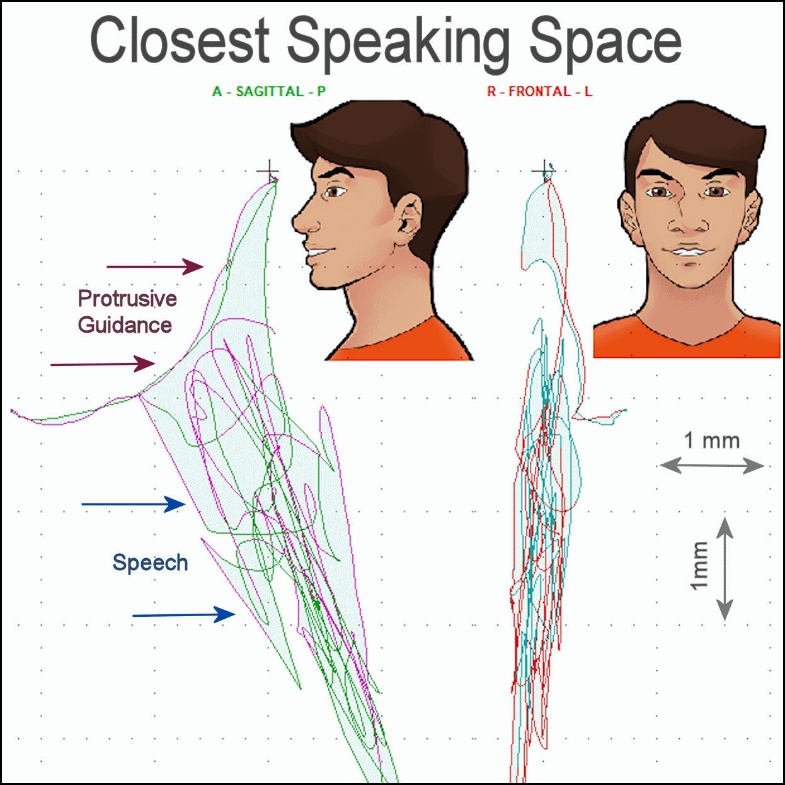
The typical ID patient exhibited a distorted envelope of speech movement as the example shown in Figure 4.

Patients with TMJ Internal Derangements cannot move their mandibles in the same way as normal control subjects primarily due to the interference of their displaced disc(s).14–16 However, the significance of the increase in the most anterior point of speech seen within this group could also be related to a difference in the average maxillo-mandibular relationship of the group (Angle’s Class), specifically the anterior tooth relationships rather than only limited to the disc displacement.9,17 This difference could also have contributed to their propensity to develop an ID condition. Another theory suggests the maxillo-mandibular skeletal relationship is more of a factor in the propensity to develop internal derangements.18 This difference in the most anterior position was found to be significantly greater in the females of the internally deranged group than in the males (p < 0.0166).
The significant reduction in lateral excursive range is also due to the disc interference with condylar translation as is typically seen on MRI images. This also reduced the protrusive range of the ID group, since even with very well adapted ID some limitation in range is seen.14
The reductions in velocities and vertical range may also be a subconscious attempt to limit the motions due to some level of discomfort. A protective response is common with injury to reduce discomfort and further damage. Since the actual range of speech movements was less than the most restricted ROM of an ID subject, the differences recorded in this group may have been due to protective responses.19
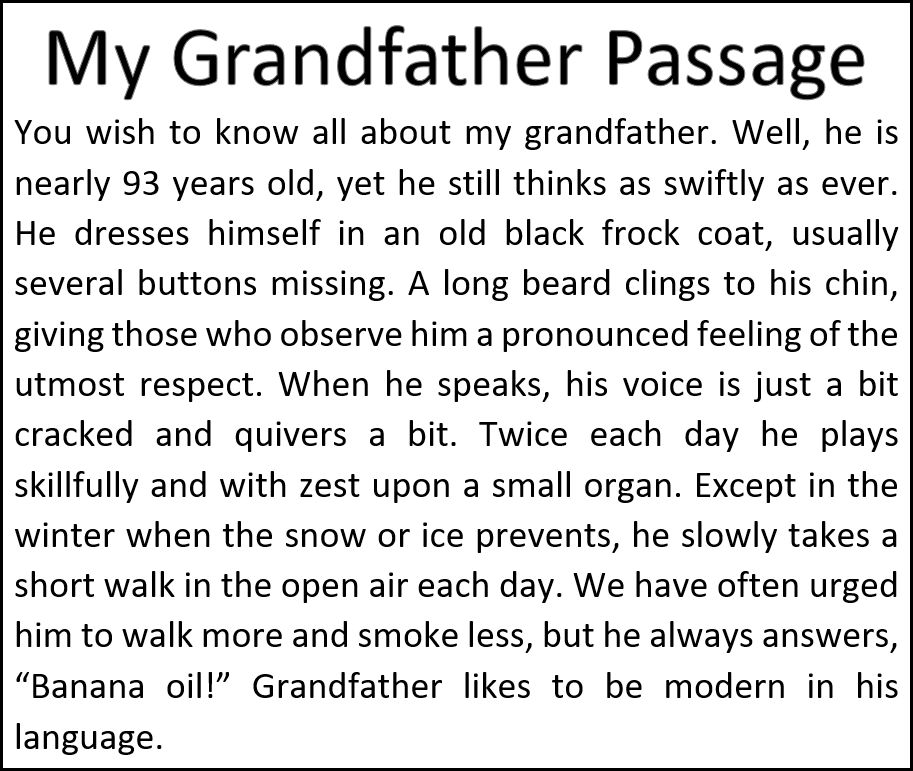
A characteristic of speech in the control group was a greater range of sagittal motion than frontal motion within the envelope. See Figure 3. This difference lead to more variation in sagittal jaw position of the control subjects as all 44 of the English phonemes are produced.6 In an ID patient with restricted condylar translation (Figure 4) the variation in the sagittal plane motion was reduced and the sagittal angulation appears flatter. In this example the amount of lateral motion within the frontal movement pattern was increased and offset to the patient’s right (the whole pattern is shifted to the right). An increase in lateral deviations during speech has been previously reported in patients with painful TMD, especially in the presence of internal derangements.20
Limitations
The question of the antero-posterior relationship of the speech to centric occlusion might have been answered more conclusively if the Angle’s classifications of the two groups had been precisely matched and the differences in anterior occlusion were evaluated. The application of EMG to this group of subjects could have enhanced the understanding more fully of the effects of internal derangements upon their speech movements.
Conclusions
The presence of a TMJ internal derangement reduced the vertical size of the speech pattern, slowed the incisor-point speech movements while the ID subjects spoke in a position more anterior with respect to centric occlusion. This last finding may have resulted from additional factors besides the conditions of the TMJs that were not tracked in this study.
Statement of funding
No funding of any kind from any source was received.
Statement of potential conflict
John Radke is currently the Chairman of the Board of BioResearch Associates, Inc.