



Introduction
Cold Sensitive Teeth are classically described as Cervical Dentin Hypersensitivity (CDH), which is as a sharp, acute pain of short duration, arising from open dentinal tubules in vital teeth. Typically, CDH is diagnosed through a process of exclusion after a thorough dental screening, examination, and history.1 CDH occurs in cervical regions of teeth with abfractions, on the occlusal surface where occlusal microtrauma, erosion, abrasion, and/or attrition has exposed dentinal tubules. Hypersensitivity may occur in vital teeth with or without open dentinal tubules, as a common response to thermal, air, osmotic, and mechanical stimuli.2
Much research has been conducted to explain why teeth experience bouts of Cervical Dental Hypersensitivity. The proposed mechanisms range from the widely accepted Hydrodynamic Theory, to the less accepted Odontoblastic Transducer Theory, to the least accepted Direct Innervation Theory, but no theory to date has found a sole etiology.2 Importantly, these 3 theories do not recognize the occlusion as a factor that induces and/or exacerbates cold sensitivity, but instead suggest open dentinal tubules and receded gingiva that exposes cementum to oral fluids, are likely causative.2 However, studies show that most treatments only temporarily and sporadically lessen cold sensitivity, because the complete etiology has yet to be adequately defined.2
Periodontal recession, abfractions, open cementoenamel (CEJ) interfaces, and exposed dentinal tubules, have been previously correlated to tooth hypersensitivity.2 The association with abfraction lesions suggests that cold sensitive teeth may result from excessive parafunctional or functional occlusal stresses,3 whereby the exposed dentin tubules could lead to increased stimulation of the pulp.3,4 One study reported that working and non-working excursive forces produced 10-20 times greater flexure to teeth than did vertical loading forces, such that flexural stresses appear to contribute to both cold sensitive teeth and abfraction lesions.5 With abfractions being implicated in occlusal disturbances,1,6,7 some authors have proposed occlusal contacts are etiologic for cold sensitive teeth.7,8 Additionally, a few long term studies by Coleman have documented that occlusally adjusting air indexed sensitive teeth, markedly reduced their cold air sensitivity response.3,9,10
One specific study employed the Cold Water Ice Swish Test,11 combined with the measured T-Scan 10 (Tekscan, Inc. South Boston MA USA) / BioEMG-III (Bioresearch Associates, Inc. Milwaukee, WI USA) guided occlusal adjustment procedure known as Immediate Complete Anterior Guidance Development (ICAGD)12,13 and a Visual Analog Scale (VAS) of self-reported pain levels, to document rapid post-ICAGD reductions in pain level responses to swishing ice cold water.11 This previous study’s findings further indicate that excursive posterior occlusal contacts can contribute significantly to many patients’ tooth sensitivities to cold.11 Additional measured occlusal adjustment studies involving Disclusion Time Reduction (DTR) with ICAGD, performed together with Electromyography, have documented the resolution of muscular TMD symptoms, improved emotional well-being, and lessened cold tooth sensitivity.14–18
As only one ICAGD treatment study has focused solely on cold sensitive teeth for analysis,11 the Objective of this patient treatment study was to replicate the earlier Cold Ice Water Swish study,11 to see if in a different patient population, cold sensitivity changed after patients underwent ICAGD. The null hypothesis is that measurably changing the occlusion with computer-guided high-precision occlusal adjustments will not change cold sensitivity pain levels.
Method and Materials
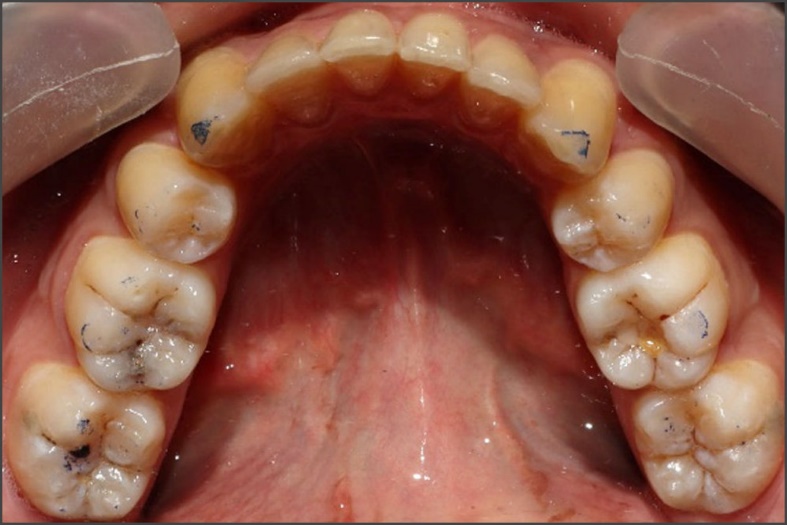
Thirty patients whom were referred to a Prosthodontic dental office with a chief complaint of sensitive teeth, for a digital occlusion evaluation. In addition to experiencing cold sensitivity, many of the referred patients also demonstrated other common Occluso-muscle disorder symptoms (chewing fatigue, chewing pain, chewing weakness, headaches, neck and facial pain, jaw tension), and some wore splints that were unsuccessful in arresting their symptoms. All of these patients had anterior teeth that coupled or nearly coupled, and presented with relatively normal occlusal relations. (Figures 1a, 1b, and 1c). Further examination with Joint Vibration Analysis (JVA) and patient consultation determined that these patients did not present with substantial temporo-mandibular joint structural compromises. However, no additional testing was employed to further diagnose any potential TMJ pathology.
__with_adequate_anterior_ov.jpeg)


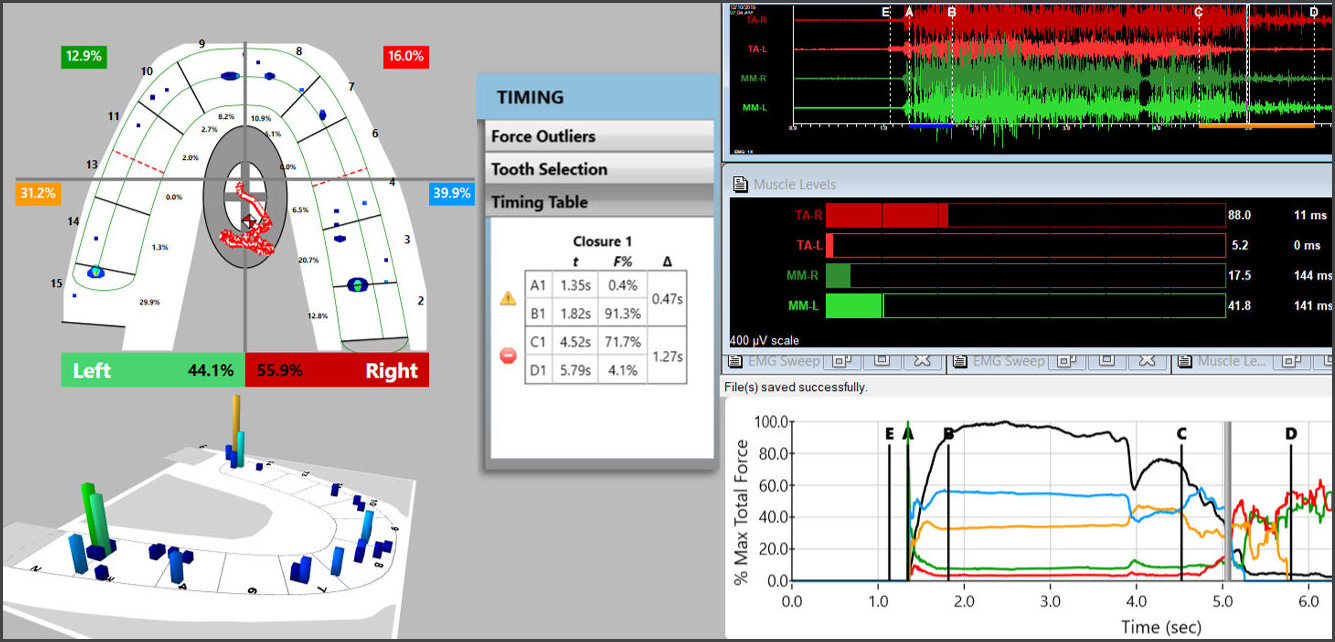
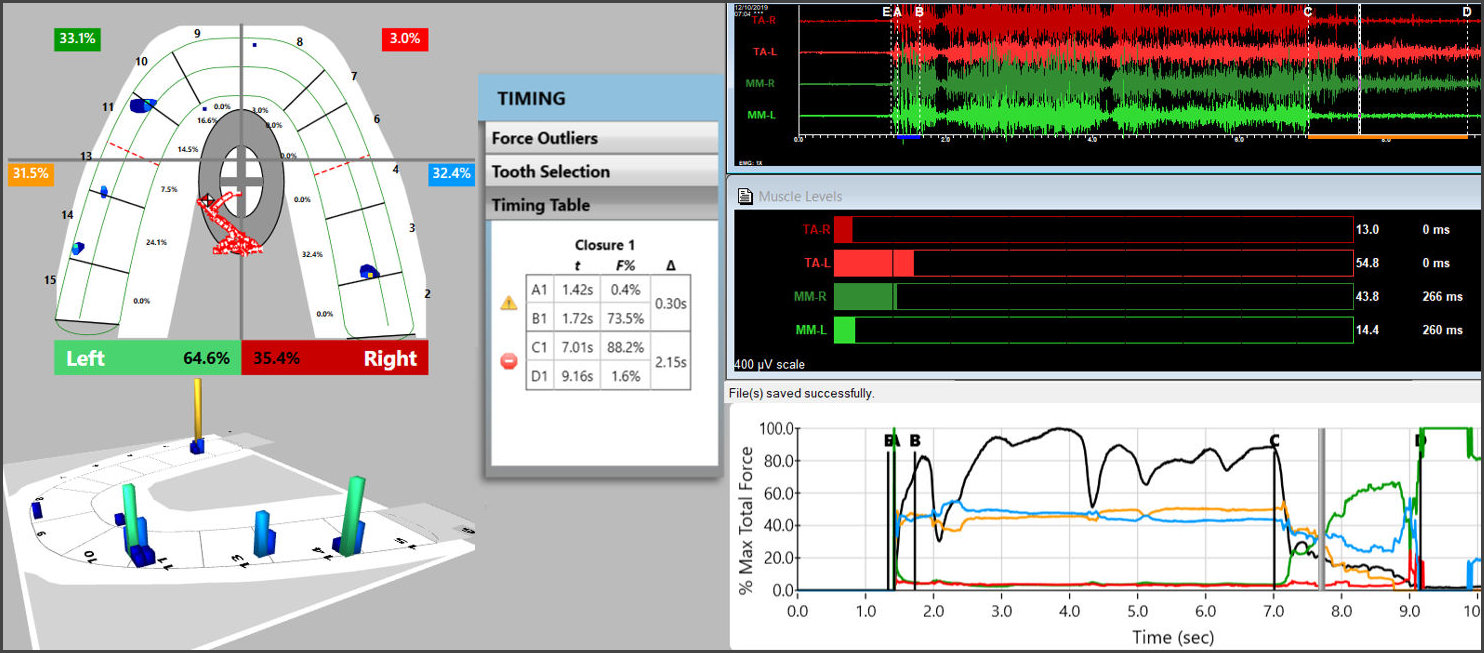
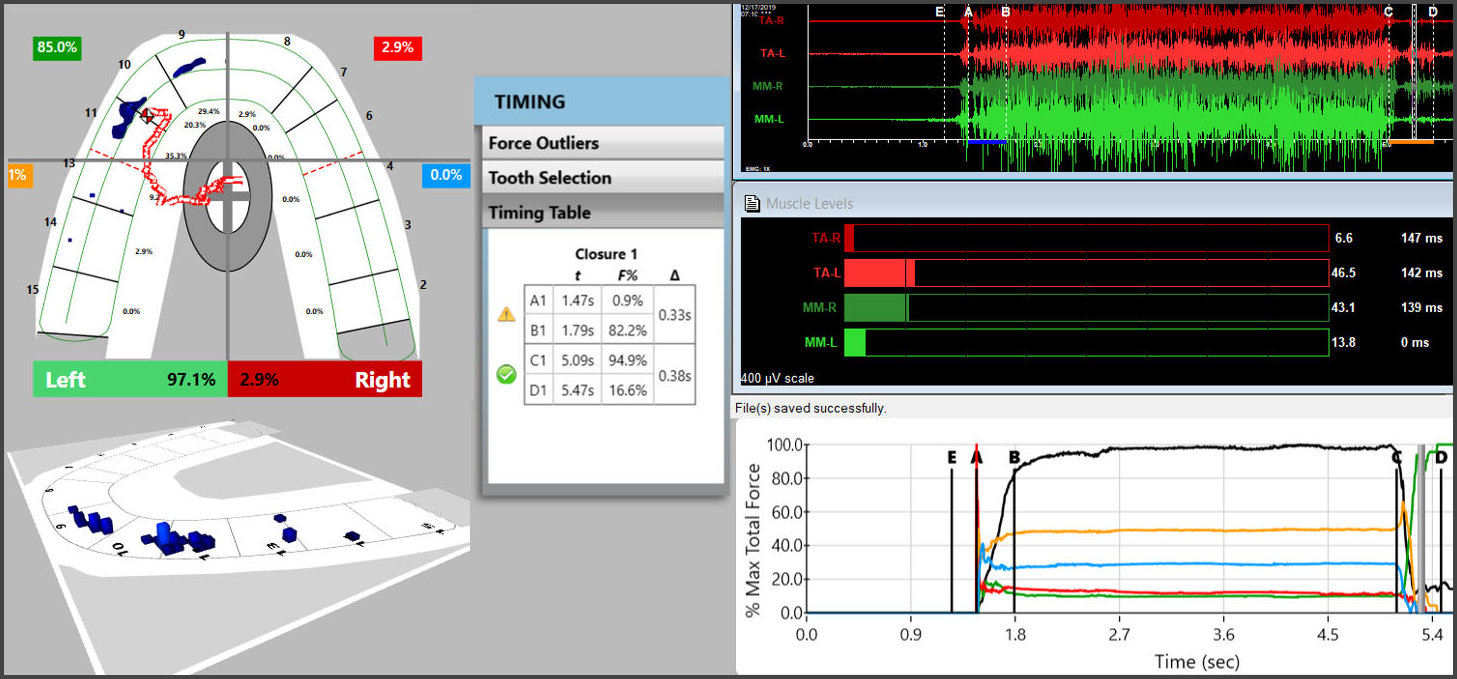
Thirty patients with cold sensitive teeth were diagnosed using the T-Scan 10 and BioEMG III synchronized technologies (Figures 2a and 2b). Each patient’s right and left excursions were recorded by having each patient close firmly into their Maximum Intercuspal Position (MIP), hold their teeth together intercuspated for 1-3 seconds, and then to commence a right or left excursion until only anterior teeth were in contact. This specific recording method ensured that high quality Disclusion Time and EMG data was obtained from each patient.19


The T-Scan was used to measure the time duration of posterior tooth contacts present during excursions, while the BioEMG III measured the intensity of muscle contractions. These combined measurements provided a neurophysiologic occlusal diagnosis before ICAGD and guided the outcome precision of the corrective occlusal adjustment process with measured numerical endpoints.
Each patient performed the Cold-Water Ice Swish Test9 (swishing ice water intraorally for approximately 5-10 seconds) to self-report (from 1-10 on VAS), their perceived pain response to the ice water. The ice water was created by adding room temperature water to a cup filled with ice, which was allowed to sit for three minutes. The temperature of the ice-chilled water was approximately 32 - 34° Fahrenheit (0 to 1° Celsius).11 The patient exhibited a generalized pain perception, rather than a single tooth pain reaction. Each patient’s initial VAS score was recorded, along with their pre-ICAGD Disclusion Times values and their excursive electromyography levels. These measurements would be compared to each individual’s post-ICAGD Cold Water Ice Swish Test VAS score, Disclusion Times and EMG levels recorded immediately after ICAGD was complete at visit 1, and then again 1 month later.
The cold sensitive patients were fully informed they were to receive ICAGD and have their enamel adjusted and polished, guided by the T-Scan/BioEMG synchronization. Next The ICAGD definitive occlusal adjustments were accomplished as previously described many times since 19916,7,14–18,20 but summarized here. The cold sensitive patient’s teeth were air dried. Then they were asked to close into their Maximum Intercuspal Position (MIP) with articulating paper (Bausch, Arti-Fol® blue 8μ, Germany) interposed between their teeth. Next, they were instructed to commence a right mandibular excursion out to the edges of their canine teeth, slide back into MIP, make a left mandibular excursion out to the edges of the left side canine teeth and back into MIP (Figures 3a and 3b).


The pre-treatment T-Scan/BioEMG recordings (Figures 2a, and 2b) guided the clinician to the areas to adjust in the ink patterns on the occlusal surfaces as the patient moved in and out of MIP excursively. Definitive corrections were made on one side of the mouth using pear-shaped finishing burs (Mani Dia-Burs, Japan ISO no-237/021), to all the excursive frictional contacts located on inclined planes and on inner/outer aspects of the molar and premolar buccal cusps (Figure 3a), leaving the central fossa, cusp tip, and the marginal ridge contact points intact (Figure 3b). These same molar and premolar excursive contacts were then eliminated on all involved surfaces on the opposite side of the mouth. In patients who experienced sensitivity during the adjustment procedure, adjustments were concentrated on opposing teeth to avoid inducing patient discomfort. No anesthesia was used (or needed) while performing all of the ICAGD occlusal adjustments.
ICAGD was considered completed when all Class I, II, and III lateral posterior excursive interferences had been visually removed, disclusion of all posterior teeth in the right and left excursions were visible, with the patient experiencing easier lateral movements than pre-ICAGD. The remaining habitual closure contacts were located on cusp tips, fossae, and marginal ridges only (Figure 3b).
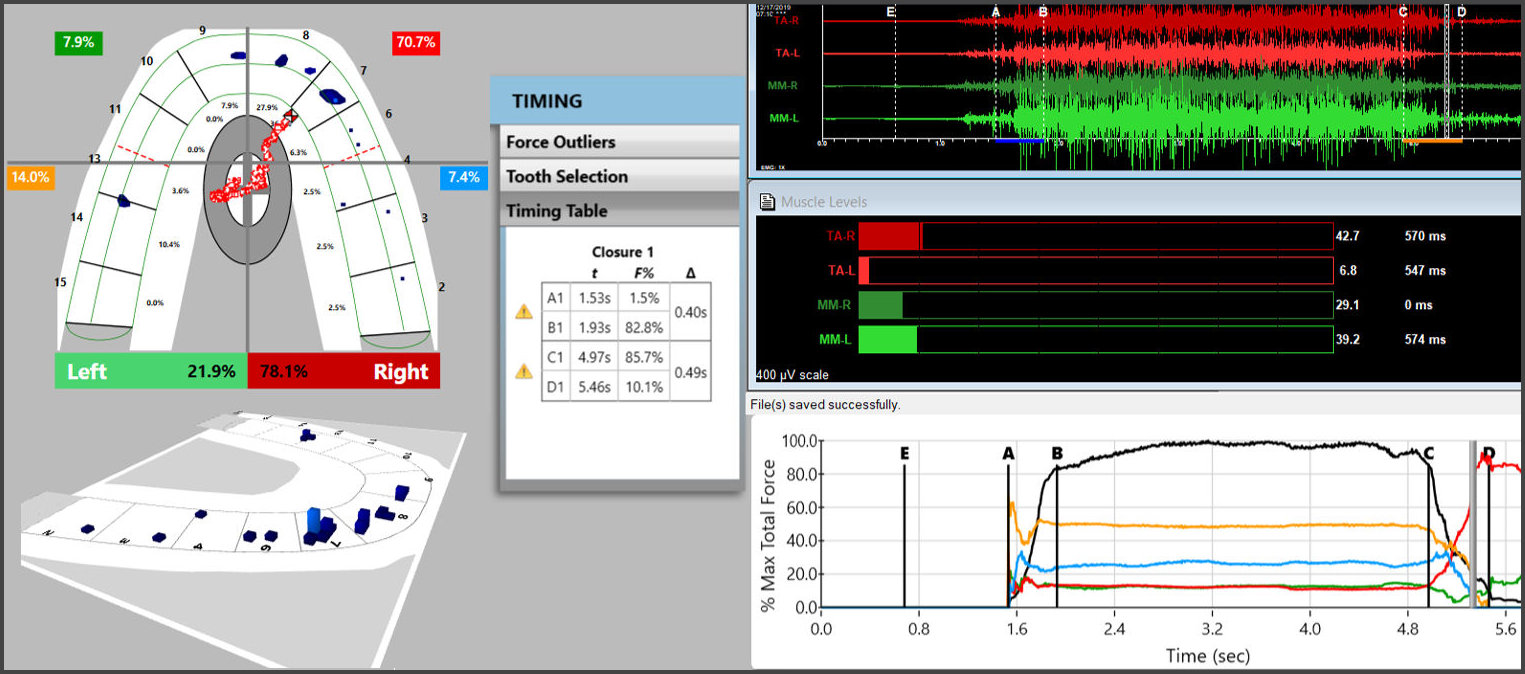
When only solid areas of contact in MIP remained, new excursive recordings were obtained to verify the Disclusion Times had been reduced to < 0.5 seconds in each excursion. Any remaining prolonged excursive contacts were adjusted until each excursion’s Disclusion Time was less than 0.5 seconds (Figures 4a and 4b).


The patients then re-performed the Cold-Water Ice Swish Test with a newly made cup of ice water, to report any changes in their perceived pain response. One month later, new excursive T-Scan/BioEMG recordings were made and a 3rd Cold Water Ice Swish Test was performed to assess any changes/no changes to their cold sensitivity response.
Results
Prior to ICAGD, the subject groups’ mean Disclusion Times were prolonged (2.25 right excursion; 2.43 left excursion), but after ICAGD the Disclusion Times means were significantly lessened (0.33 right excursion; 0.32 left excursion; p < 0.05). This was expected, since that was
the main criteria for treatment. The Disclusion Times were further significantly reduced at one-month post ICAGD (0.29 right excursion; 0.29 left excursion). See Table 1.
The VAS data revealed that the mean tooth sensitivity to the Cold-Water Ice Swish Test was immediately significantly reduced post-ICAGD treatment. See Table 2. A second significant reduction was observed at one-month post-ICAGD without any further treatment. The final median VAS value for the group was zero, with only a few patients indicating minor residual sensitivity to Cold Water in Ice Swish.
Discussion
The Results of this Cold Sensitive Teeth pilot study corroborate the findings of the earlier Cold Water Ice Swish Test study,11 wherein the cold sensitivities of teeth were reportedly reduced following ICAGD, along with other TMD symptom improvements.11,14–18,20 In these 30 patients, the perceived cold sensitivity levels were reduced immediately after ICAGD was rendered, which continued to improve over the 1-month period of observation. The repeated VAS scaled self-reporting of Cold Sensitive Teeth pain (Table 2) determined there were significant reductions in perceived cold sensitivity levels after the long Disclusion Times were significantly reduced to short Disclusion Times (Table 1). This study’s findings suggest that a lack of posterior excursive disclusion (Disclusion Time > 0.5 seconds),12 when patients’ posterior teeth excursively engage for long durations, can induce cold sensitivity. Importantly, the results of this study directly support the studies from earlier authors who found occlusal contacts were causative of, or contributed to cold sensitivity.11,14–18,20
A possible explanation: How prolonged excursive contacts contribute to chronic tooth sensitivity to the Cold-Water Ice Swish Test
The key factor in cold sensitivity appears to be that lateral occlusal surface frictional interactions leads to excessive Periodontal Ligament (PDL) compressions which directly increases muscle contractions that increase the latero-flexion of tooth structure, which activates a pulpal and/or periodontal neurologic response.21 The post ICAGD pain level reductions resulted from reduced tooth latero-flexion following minor alteration of the posterior occlusal surfaces to shorten the prolonged excursive contacts on the Cervical Dentinal Hypersensitivity (CDH) sensitive teeth to a level that has been shown in many studies to improve the occlusal neurophysiology (< 0.5 seconds per excursion).11,12,14–18,20 Cold sensitivity likely results from strain and deformation of the involved teeth. The physical deformation of the dentin triggers nerve impulses that bio-mechanically activate the intra-pulpal and omnidirectional A-beta myelinated nerve fibers.22 This study’s findings therefore closely align with The Direct Innervation Theory of Dentinal Hypersensitivity.
It is also possible that autonomic inputs resulted in intra-pulpal vasoconstriction following repetitive occlusal microtraumas from ongoing excursive frictional contacts that bend and flex teeth repetitively thousands of times per day. It is well known that tissues that sustain microtrauma exhibit restricted blood flow. With ongoing tooth microtrauma, the pulp likely vasoconstricts, whereby reduced warm blood volume within the pulp chamber leaves the pulpal nerve fibers exposed to respond to the cold ice water, as it washes over the micro-traumatized tooth. A worsening factor to the tooth flexure, which would also worsen microtrauma and the vasoconstriction, is that excess muscular forces overload the teeth when PDL mechanoreceptors are compressed from the flexure for prolonged excursive contact durations.23 The rapid cold sensitivity resolution clinically observed within these thirty patients, suggests that most of the blood flow quickly returned to the pulp (vasodilation), once the muscularly induced torsional strain deformation of the involved teeth was eliminated by the ICAGD measured occlusal adjustments. However, as additional cold sensitivity improvements were recorded at one-month post-ICAGD, some additional time was required for the cold sensitivity to fully resolve.
ICAGD removes the occlusal surface friction from the subject’s mandibular excursions, so the posterior teeth disclude in very small distances and very rapid time durations (≤ 0.5 seconds). See Table 1. This frees the posterior teeth from lateral excursive engagement, whereby the treated subjects can function muscularly at or near their resting levels of muscle contraction.12,23 This drastically reduces posterior tooth flexure, which then lessens the microtrauma, which restores pulpal blood flow and minimizes the neural pulpal response to tooth flexure. These physiologic changes are neurologically mediated within the Central Nervous System24 because the time-duration and volume of posterior teeth pulpal nerve fiber flexures and PDL nerve fiber compressions are both drastically reduced by ICAGD.14–18,23
Limitations
Although this group of subjects showed significant reductions in tooth sensitivity to the Cold-Water Ice Swish Test, this study’s limitations were that there were only a small number of subjects, (30), there was no control group of subjects to compare the treated subjects’ outcomes against and the follow-up period was only 1 month. However, the repeated use of a VAS helped to overcome these limitations, as each repeated VAS acted as its own control comparison to the pretreatment self-reported levels of cold sensitivity over the 1-month period of observation. Further, considering that the median VAS group score reached zero at one month, it is unlikely that any further testing could have produced any additional significant reduction.
Conclusions
In this 30-patient pool, excursive occlusal contacts played a causative role in tooth sensitivity to the Cold-Water Ice Swish Test and the measured long Disclusion Times. ICAGD and DTR treatment significantly reduced the frequency and intensity of cold sensitive teeth. This result indicated that an Occlusion-Cold Sensitive Teeth interrelationship physiologically exists, whereby Trigeminal nerve afferent input from occlusal contacts that bend, compress, and flex pulpal and PDL fibers, contribute to the initiation and perpetuation of cold sensitivity. Once removed via ICAGD, the cold sensitivity of the teeth was markedly reduced. A Cold Sensitive Teeth DTR Randomized Clinical Trial study would be needed to further document occlusion’s primary role in tooth sensitivity to cold.
Potential conflict of interest statement
The 3rd author (R.B.K) is a consultant to Tekscan, Inc., but receives no monetary or other gain from the sale of product. The 4th author (J.R.) is the Chairman of the Board of BioResearch Associates, Inc., receives no commissions from sales.
Funding Statement
No funding was provided for this study from any source.