

INTRODUCTION
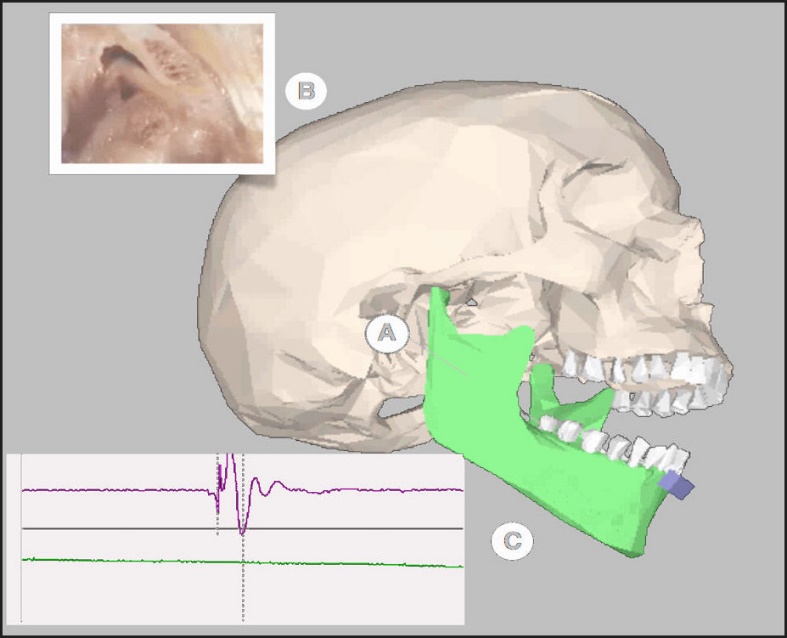
A Joint Vibration Analysis (JVA) system records and analyzes the vibrations resulting from variety of internal temporomandibular joint anomalies. It uses accelerometers to accurately measure the amplitude and frequencies of vibrations emitted from the TMJ’s condyle/disc assembly during cyclic mandibular maximal opening and closing. Figure 1 illustrates the JVA technology placed on a patient’s head as it is recording vibrations.

Figure 2 diagrammatically represents a specific pathology that produces a TMJ vibration that a joint emits when the mandible opens (A) and a disc displaces (B). JVA (C) also detects a vibration’s energy transfer from the ipsilateral to the contralateral temporomandibular joint, which indicates for the clinician the direction that a disc is displacing and reducing from.1
__a_disk_displacing_(b)_and_a_jva_ddr_waveform_(c)._note_the.jpeg)
Moreover, JVA correlates with disease state existence 75-90% of the time, and does not correlate with a disease state when there is no disease present (98% of the time).2,3 Due to its high specificity, JVA is an excellent screening tool for TMJ internal derangements that assists a clinician in determining if a patient possesses bilaterally stable and adapted TM joints.
JVA can also be combined with MRI and CBCT to complete a detailed joint structural evaluation before any occlusal therapy is instituted. Most importantly, detected vibrations illustrate TM joint structural deformities such that differing vibrations correlate to temporomandibular joint specific structural pathologies.4–10
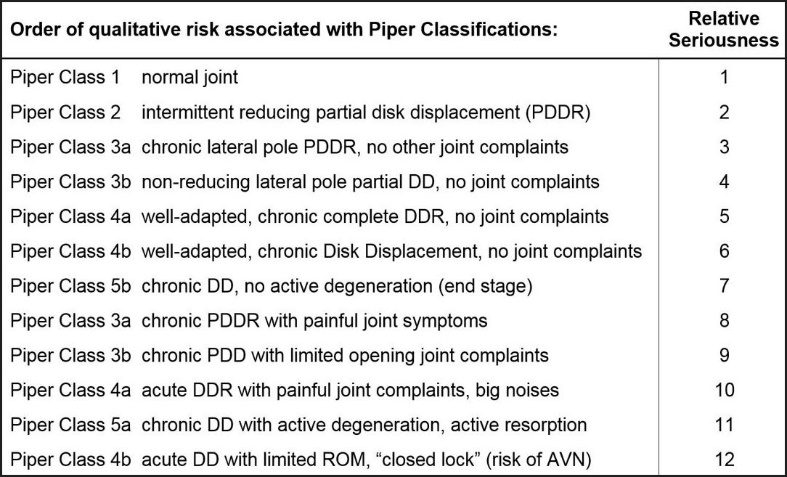
The amplitude of a given vibration and its waveform pattern indicate the energy associated with a particular internal TM joint dysfunctional event.11 When the amount of energy is combined with the location at which the vibration occurs along the patient’s opening and closing pathway, the vibration can be staged for disease progression by the Piper Classification.12
The 7 Piper Stages of Temporomandibular Joint internal derangement and degeneration have previously been described by Droter.12 They represent a progression of conditions that a TMJ may or may not follow. The progression is not always completed and may stop at any point along the progression, when the patient adapts sufficiently at that stage.
Piper* Classes
1 – Normal Temporomandibular Joint
2 – Loose capsule without disc dislocation
3a - Partial disc dislocation, with reduction
3b - Partial disc dislocation, non-reducing
4a - Complete disc dislocation, with reduction
4b - Complete disc dislocation, non-reducing
5a - Disc dislocated, perforation, adapting.
5b - Disc dislocated, bone to bone, end stage.
(*Developed by Dr. Mark Piper, St. Petersburg, FL)
When a substantial portion of a vibration’s frequencies are greater than 300 Hz, there is likely significant Degenerative Joint Disease (DJD) present within a TM joint. These high frequency vibrations result from rough surfaces rubbing together (may or may not be bone-to-bone) during opening and/or closing.5,6
Chronic Occluso-Muscle Disorder (OMD) is a subset of painful Temporomandibular Disorders (TMD) with pain symptoms primarily afflicting the masticatory musculature, whereby the lateral pterygoid is often affected.13 Chronic facial pain, temporal headaches, clenching, and grinding of the teeth, morning jaw pain, eye strain, earaches, tooth pain, and temperature sensitive teeth, are all commonly reported dysfunctional symptoms.14–16 Patients that are suffering from a masticatory muscle disorder exhibit increased tonicity of the elevator muscles, creating an increased intra-articular pressure in the TM joint. This condition is further aggravated by hyperactivity of the superior head of the lateral pterygoid muscle, which is very active during clenching and can accentuate increased clicking,17 whereby loud clicking and popping often accompanies those muscular temporomandibular dysfunction symptoms.
The lateral pterygoid is a short, thick, 2-headed muscle (with superior and inferior bellies), which extends horizontally, posteriorly, and laterally between the infratemporal fossa and the mandibular condyle. The superior belly originates at the infratemporal surface and infratemporal crest of the greater wing of the sphenoid bone, that inserts into the condyle, the TMJ capsule, and the TMJ disc.18–20 The inferior belly originates from the lateral surface of the lateral pterygoid plate and inserts into the neck of the mandibular condyle. The superior belly is essential in pulling the capsule and disc forward during mandibular opening, to keep the disc in a normal relationship in between the mandibular condyle and the eminence. The inferior belly is active for opening the mouth, protrusion, and contralateral jaw movement. The nerve supply to the lateral pterygoid arises from the anterior trunk of the mandibular nerve (V3), and includes the swallow reflex neurologically.20
Hyperactivity of the lateral pterygoid muscle with longstanding anterior disc displacement without recapture, has long been considered a major contributor to the discomfort of a TMJ internal derangement.21 Since the ligamentous attachments of the disc to the glenoid fossa wall are at the condyle’s medial pole, as are the attachments of the disc to the retro-discal tissues,22–25 the lateral aspect of the disc can be more easily displaced than can the medial aspect. An additional factor involved in the easier lateral pole disc displacement are the directional forces the superior lateral pterygoid muscle exerts on the disc.17 Ultimately, if muscle hyperactivity were present, the superior lateral pterygoid would have an even greater influence on the disc position.17
A hypercontracted lateral pterygoid has a foreshortened overall length, that pulls the disc capsule forward and away from the top of the condyle towards its origin on the sphenoid bone. Repeated occlusal microtrauma that occurs during mandibular functional movements in and out of maximum intercuspation can weaken the attachment of the disc to the lateral pole, whereby the torn attachment allows the disc to be pulled antero-medially. This displacement of the disc then repeatedly moves off of and back onto the condylar head, snapping in and out of place during mandibular motion.
Multiple published studies and reports using the T-Scan computerized occlusal analysis system and the measurement-driven occlusal adjustment procedure known as Immediate Complete Anterior Guidance Development (ICAGD),26–36 have shown that rapid and lasting dysfunctional TM Disorder muscular symptom resolution can be accomplished with ICAGD.14 ICAGD is clinically performed today with simultaneously recorded EMG data of the masseter and temporalis muscles.26,30–34 ICAGD represents a computer-guided occlusal adjustment procedure that shortens prolonged Disclusion Times (DT) during lateral excursive movements. ICAGD studies since 1991 have shown that for patients with long DT, lessening the DT to less than ½ second per excursion can effectively lessen the muscular symptoms of occlusal dysfunction commonly reported in TMD patients, while improving chewing mechanics and average chewing patterns.34 The reduction to a less than ½ second DT creates an occlusal scheme where opposing posterior teeth compress their Periodontal Ligament (PDL) fibers for far less time than in the pre-ICAGD condition. Reduced PDL compressions then shorten the contraction time of the Muscles of Mastication, which are also part of the Swallow Mechanism neurologically.20 Post treatment physiologic muscular relaxation is established, by drastically shortening the duration of excursive frictional contacts.14,22,26–34 Once the hyperactivity is decreased, rapid dysfunctional muscular TMD symptom resolution follows, including improved chewing capability.26–34
Although it has been reported in publications that TM joint noises post ICAGD have lessened in frequency and intensity,14 to date, no study has quantified changes in the JVA patterns reflective of changes to the disc/condyle relationship within the Temporomandibular Joint resultant from the ICAGD coronoplasty.
OBJECTIVE
Objective: To evaluate the TMJ vibrations and Range of Motion (ROM) changes in Occluso-muscle disorder (OMD) subjects before and after undergoing the ICAGD coronoplasty. The null hypothesis was no change.
MATERIALS and METHODS
Inclusion criteria
Forty-three subjects that reported non-painful noises in their Temporomandibular Joints were evaluated using the Piper Classification system.12 Three were diagnosed by MRI with unilateral chronic disc displacement with reduction (DDR), but none exhibited indications of advance degenerative conditions. Ten subjects had ROM values prior to ICAGD that were limited (< 40 mm) and were diagnosed with chronic disc displacement without reduction. Using JVA, no subject exhibited a Piper Classification risk greater than 6. (Arbitrary units, see Figure 3.)

In addition to TM joint noises, these subjects reported a variety of additional non-TM joint complaints including chewing fatigue, chewing pain or chewing weakness, ongoing head, neck and facial pain, headaches around the eyes, midface, temples, and frequent jaw tension. Some also reported previous ineffective splint use and chronic pain medication ingestion. For ICAGD to be performed on these subjects in a minimally invasive fashion, the selected patients were required to have anterior teeth that coupled or nearly coupled. Figure 4 shows a typical Class I subject from the presented study who had a dysfunctional TM joint with a displacing disc.
_of_a_class_i_subject_who_has_a_dysfunctional_tm_joint_w.jpeg)
Exclusion criteria
The excluded subjects demonstrated primary internal derangements like closed locking, painful disc displacement with or without reduction, condylar avascular necrosis, loss of condylar height, a present tumor within the temporomandibular joint, or a markedly reduced vertical opening. Anterior open-bite occlusion patients were also excluded because not only could they not undergo ICAGD due to an absence of coupled anterior teeth, but MRI has determined that open-bite occlusion patients often present with serious soft tissue disc displacement events and unstable and maladapted occlusions.28 Lastly, any potential subjects who after receiving full JVA and ICAGD protocol disclosure, did not choose to participate were also excluded.
Over a period of 2 years, patients presenting in the two separate dental practices of two highly skilled ICAGD providers (who were properly calibrated in ICAGD by an alternative author; RK), that demonstrated and reported limited joint noises and chronic painful muscular TMD-like symptoms, and that also elected to undergo the ICAGD enameloplasty for treatment of their existing dysfunctional condition, were recruited for participation. Potential subjects completed a symptom evaluation questionnaire that was used to screen patients for possible study eligibility. The questionnaire detailed each subject’s TM joint and muscular symptoms such that subjects were selected from chronic muscular dysfunction patients (OMD) with minor TM Joint pathology, despite the subjects having previously undergone earlier interventions like splint therapy, soft food diets, TENS, or physical therapy. Ultimately, based upon the Inclusion and exclusion Criteria, 43 muscularly dysfunctional subjects with noisy TM joints elected to participate in the study (15 males, 28 females; mean of 42 (+/- 14) years of age).
Risks and Benefits of JVA and ICAGD
All participants were informed of the risks and benefits of JVA and ICAGD. JVA has minimal patient risks as it is an extraoral recording of TM joint vibration patterns, involving no therapeutic intervention to be performed. JVA’s Benefits are; a) It can quickly and inexpensively assess the health or degree of damage present in the TM joint non-invasively and b) when combined with a detailed history and examination, it can indicate whether MRI or CBCT is necessary to contribute to a more complete and accurate TM joint diagnosis. ICAGD’s risks include experiencing subjective occlusal contact “feels very different” issues, sustaining restoration occlusal surface perforation, lack of symptom improvement, and observing mild increases in temporomandibular joint clicking.13
In the appropriate patient, ICAGD’s benefits include one or more of these reductions in a) chronic muscular TMD symptoms, b) splint dependency, c) night time clenching and grinding habits, d) use of adjunctive therapy (Physical Therapy or Chiropractic Care), e) dependency on medication use, f) temporal headache and facial pain, g) masticatory muscle spasm and pain, h) cervical Frictional Dental Hypersensitivity (FDH), and i) clicking and popping of the Temporomandibular Joints.13,16,21–26 There is also literature demonstrating that ICAGD can significantly improve masticatory capability in muscularly dysfunctional patients.27
Informed consent
Each subject was also informed that the T-Scan 9 /BioEMG III recordings and JVA would be employed before and after ICAGD, to assess any changes within the occlusal contact pattern, masticatory muscle activity levels and TMJ status resultant from ICAGD treatment. Included subjects were fully informed and consent was obtained from all individual study participants. All procedures performed in this study involving human participants were in accordance with the ethical standards of the World Medical Association Declaration of Helsinki and its later amendments. The protocol and procedures for this study were reviewed and approved (BIRB/94Z/2017) by the institutional review board at BioResearch Associates, Inc.
Research Protocol
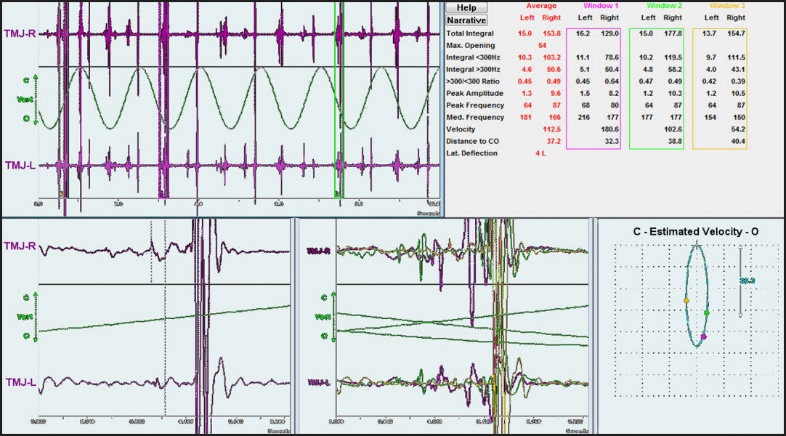
The research protocol specified JVA to measure the Range of Motion (ROM) and TMJ vibrations present during mandibular opening and closing. The subjects performed 2 to 4 JVA recordings of 6 complete open and closing cycles. Figure 5 shows the JVA interpretation of the TM joint vibrations that the patient shown in Figure 3 presented with, prior to undergoing the ICAGD enameloplasty. This large vibration described this subject’s pre ICAGD TM joint pathology.

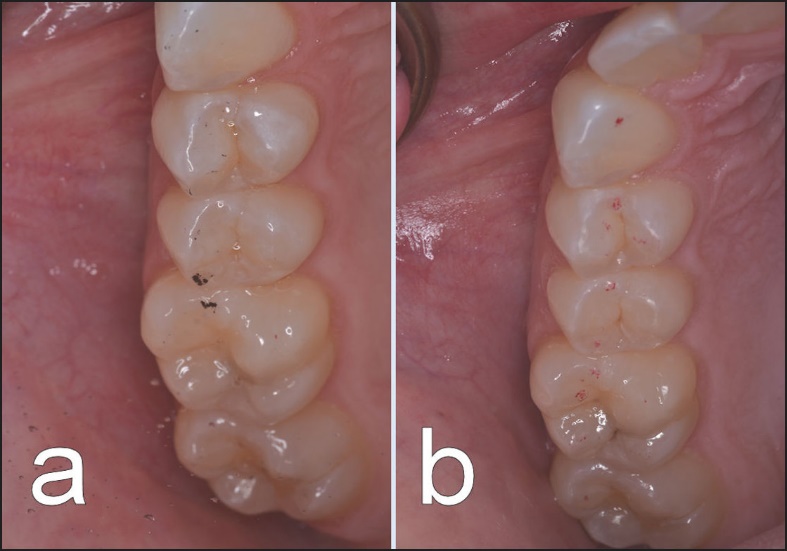
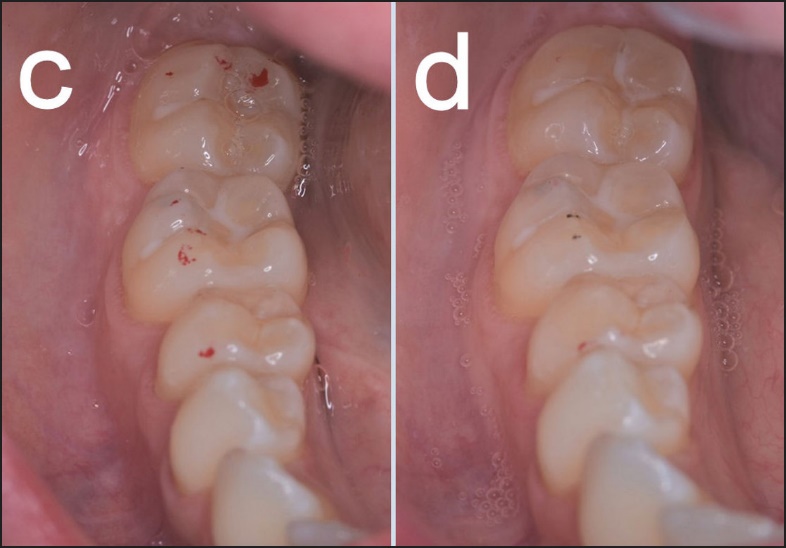
After saving their pretreatment ROM and JVA recordings, each subject underwent the ICAGD enameloplasty using the T-Scan 9/BioEMG III synchronization module (T-Scan 9, Tekscan, Inc. So. Boston, MA, USA; BioEMG III, Bioresearch Associates, Inc. Milwaukee, WI, USA) to shorten their right and left excursive disclusion times down to ≤ 0.5 second per excursion. Since 1991, the ICAGD coronoplasty technique has been extensively described in multiple publications.13–16,22–28,30 For brevity, the authors have chosen to reference prior published accounts of how ICAGD is properly performed rather than explain its protocol once again in this manuscript. Multiple accounts of how ICAGD is properly performed have been available in different peer-reviewed journals for 27 years now beginning in 1991. Figures 6a-d illustrate the occlusal changes to 23 micron-thick articulating paper markings (Accufilm, Parkell, Inc. Farmingdale, NY, USA) of the maxillary and mandibular left posterior quadrants of one subject from before to after ICAGD. The post ICAGD contact patterns show minimal tooth contact representative of minimal occlusal surface excursive movement friction, which induces minimal periodontal ligament compressions.36
_and_post-treatment_paper_marks_(b)_reveal_the_reducti.jpeg)
_and_post-treatment_paper_marks_(d)_reveal_the_reducti.jpeg)
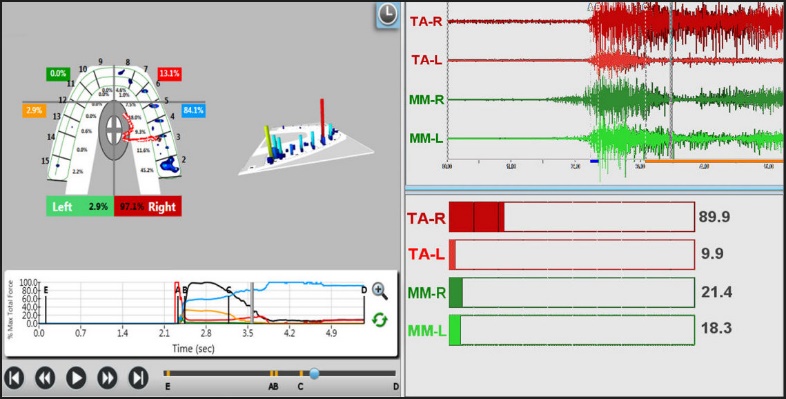
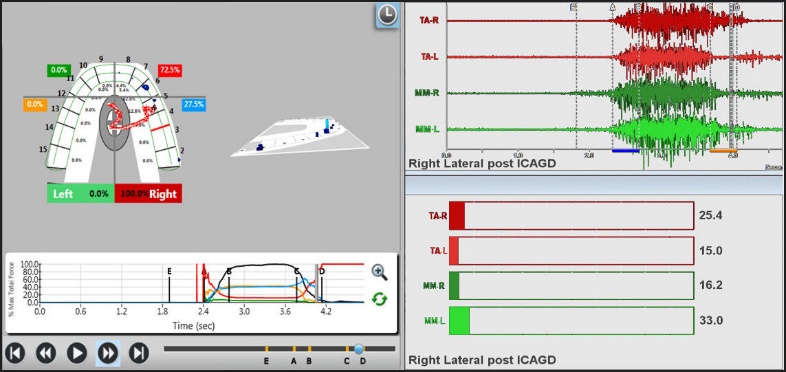
Figures 7a and 7b show the pre ICAGD and the post ICAGD (T-Scan/BioEMG III) data of the subject in Figure 4. These figures illustrate the occlusal and muscular changes resultant from ICAGD that induced less muscle hyperactivity in the simultaneously measured muscles.


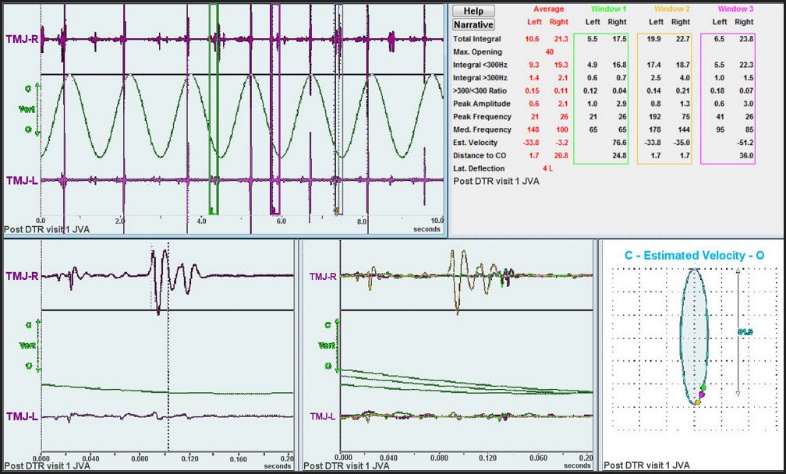
One to two months after initial ICAGD therapy was rendered to each subject, each subject’s ROM and JVA were re-recorded. Figure 8 illustrates the change in the TM Joint vibration observed in the subject shown in Figures 4 and 5, after undergoing the ICAGD coronoplasty.

Included subjects acted as their own Controls by comparing their individual pre-ICAGD ROM and JVA to their post-ICAGD ROM and JVA. Piper Classification “order of risk” assessment (Figure 3) of mean group TMJ conditions from pre to post ICAGD was subjected to the Mann-Whitney U Test.
Additionally, pre and post ICAGD means and standard deviations were calculated for the left and right Disclusion Times, and for seven defined JVA vibration parameters, that were all measured pre and post ICAGD:
-
The Total Integral = the integral of the frequency distribution from 20 to 500 Hz – (A measure of the total amount of energy contained in a vibration causing event, such as a disc popping back onto a condyle)
-
The < 300 Hz Integral = the integral of the frequency distribution from 20 to 300 Hz –(A measure of the amount of energy in the low frequency range below 300 Hz, which is mainly due to disc movements onto or off of the condyle)
-
The > 300 Hz Integral = the integral of the frequency distribution from 300 to 500 Hz – (A measure of the amount of energy in the high frequency range, which is mainly due to degenerative changes and likely osseous contact within the TM joint)
-
The > 300 Hz / < 300 Hz Ratio- this ratio is a better indicator of TM joint degenerative changes than the > 300Hz integral when a vibration is large
-
The Peak Amplitude is the intensity or “loudness” of the dominant frequency – (values greater than 6 are usually audible TM joint noises)
-
The Peak Frequency of the vibration – (the frequency of the Peak Amplitude, which is related to the relative chronicity of the condition. The lower frequencies are associated with more chronic TM joint conditions)
-
The Range of Motion from maximum intercuspation (MIP) to maximum opening – (A measure of any restriction in the ability of a patient to open wide).
Statistical analysis of changes in these 7 JVA measured parameters pre to post ICAGD was accomplished using the Student’s Paired t-test (Alpha = 0.05).
RESULTS
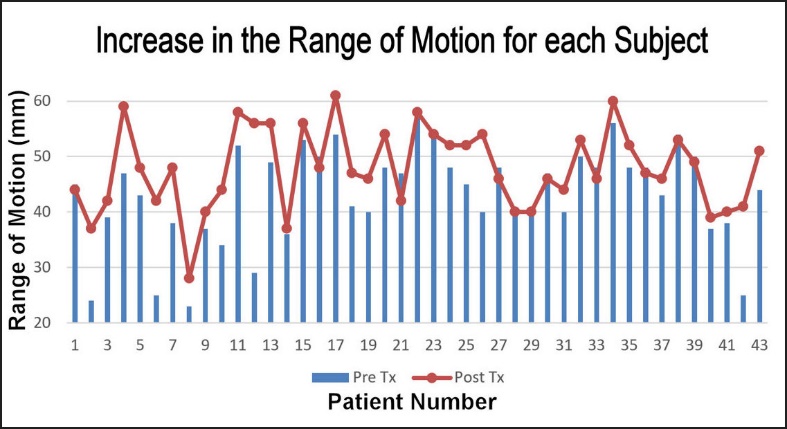
The mean Range of Motion for this group of subjects increased from 43.4 mm pre-ICAGD to 47.7 mm after ICAGD treatment (p < 0.0002). See Figure 9.

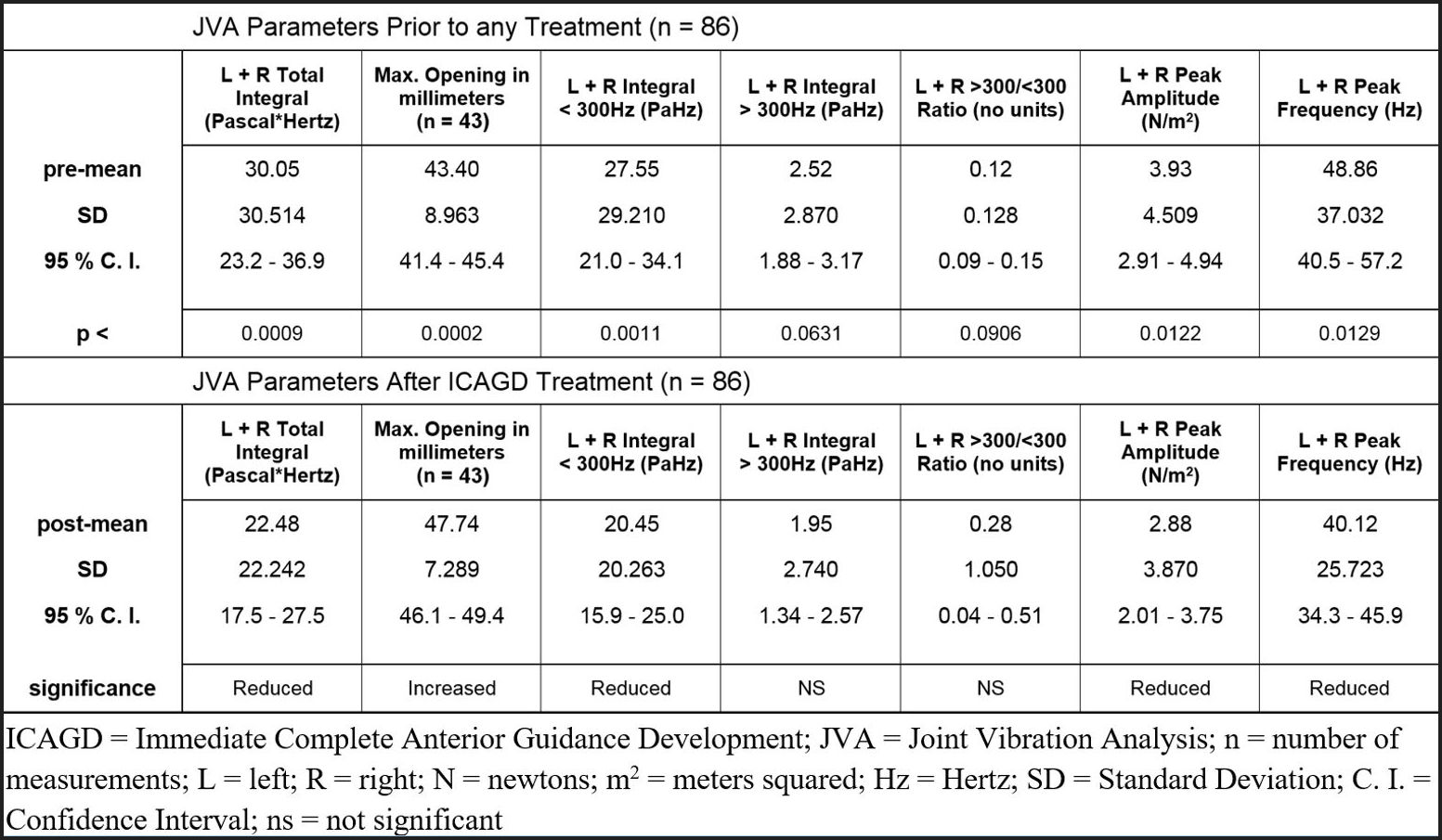
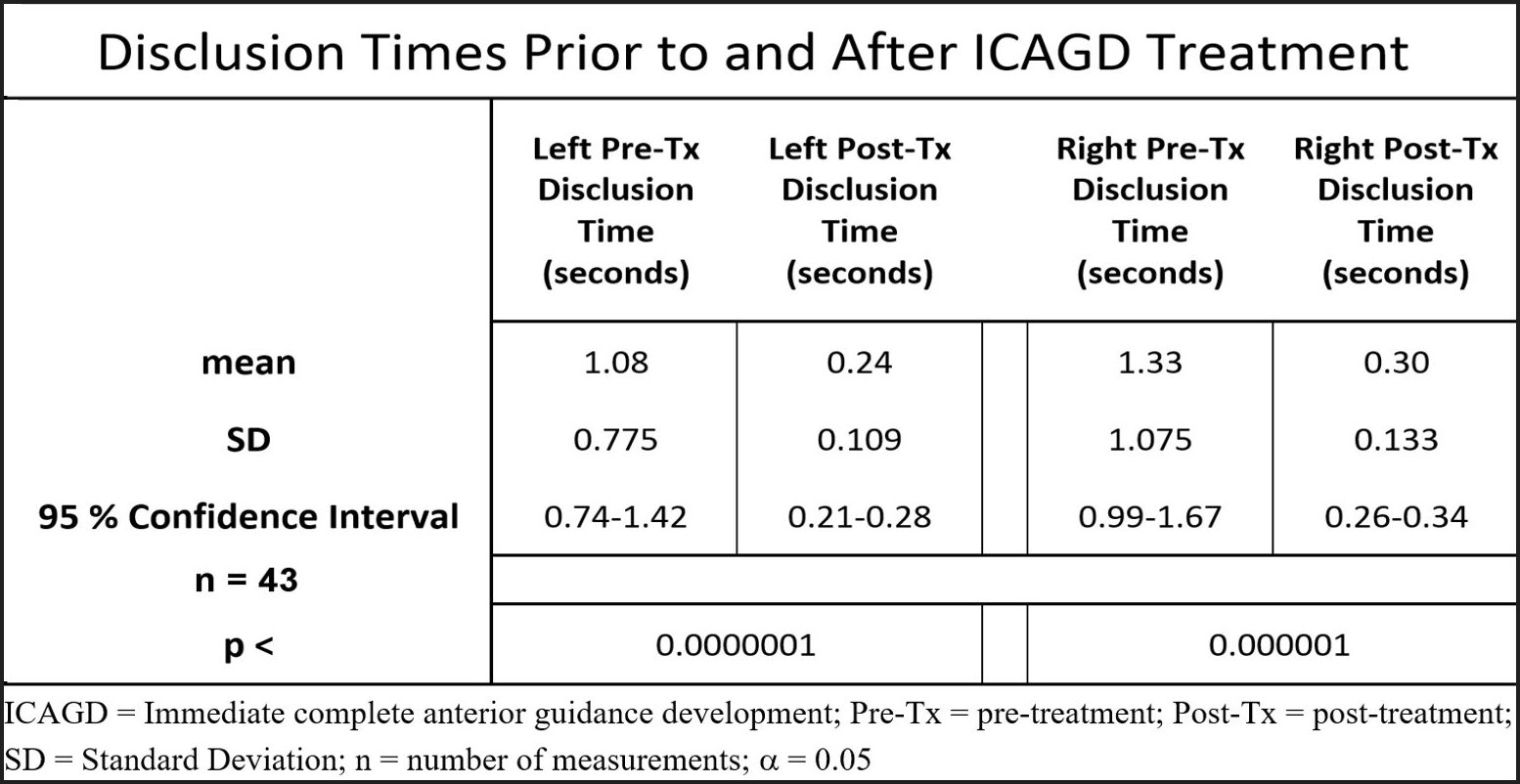
The pre-treatment and 2 - 3 months post treatment separately calculated mean values for each of the six JVA parameters were compared, left-side to right-side, using Student’s t test for 2-tailed distributions with equal variances. All six of the left and right JVA parameters had nearly equal variances and were not significantly different between sides (for all p > 0.05). Therefore, it was decided to use the common statistical tactic of pooling the left and right-side mean values for each JVA parameter at each time-point.37 This was done to increase the n-value from 43 to 86. Then the 6 pre-treatment pooled means were compared to the pooled 2 to 3 months post-treatment means using Student’s Paired t test. See Figure 10. Four of six JVA parameters (Total Integral, Integral > 300 Hz, Peak Amplitude and Peak Frequency) were significantly reduced after ICAGD treatment (p < 0.013). Only the Integral > 300 Hz, and the > 300 Hz/< 300 Hz ratio were not significantly changed. The Disclusion Times were significantly reduced for both the left and right excursions (p < 0.000001). See Figure 11.


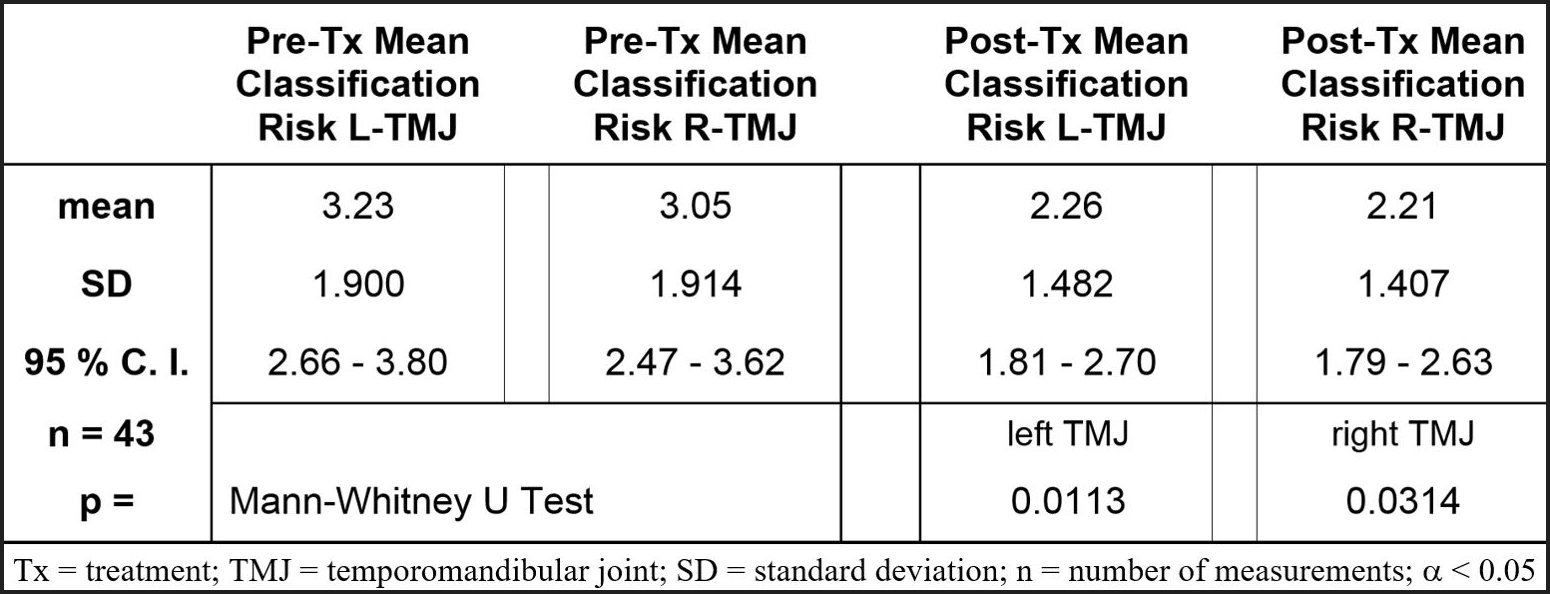
The Mann-Whitney U Test determined that the Piper classification “order of risk” assessment mean values significantly decreased (p < 0.032). See Figure 12. For both the left and right TMJs the measured reductions in joint vibration intensities after ICAGD resulted in significant bilateral lessening in the severity of the TM joint dysfunctions.

DISCUSSION
The Results of this investigation indicate that many mildly pathologic TM joint conditions as observed in this group of dysfunctional subjects improved after their prolonged Disclusion Times were shortened to < 0.5 second per excursion. As this was the first ever-attempted study using Joint Vibration Analysis to assess vibration pattern changes resultant from computer-guided occlusal therapy, these results cannot directly support or refute the findings of earlier studies (there are none). However, these results do support and explain the findings of previously published Disclusion Time reduction/ICAGD studies where TM Joint symptoms were reported subjectively reduced (as self-reported by treated subjects), along with a lessening of many chronic Occluso-muscle disorder symptoms.14–16,26–34 Moreover, the reduced TMJ noises following ICAGD documented within this dysfunctional subject pool, reflect changes towards improved TM joint function similar to those observed in normal subjects when measured with JVA alone.38–40
The significant changes in four JVA parameters illustrate that ICAGD brought about very significant changes to the subject pool’s TM joint structural vibrations (Figures 10 & 12). The reduced vibrations were seen as smaller Total Integrals, less energy below 300 Hz typically due to less disc hypermobility, lowered Peak Amplitudes (loudness) and lower Peak Frequencies, indicated there was likely less aberrant disc movement (disc bouncing around), which is indicative of definite improvements in disc function during mandibular motion.38–40 ICAGD clears the right and left lateral excursive outward from MIP pathways, by creating reduced posterior occlusal surface friction in excursive movements, that then requires lower muscle activity levels to perform.26,30,31 The disclusion pathway is utilized during mastication (but in the reverse direction), making it an important factor in the improvement of a patient’s ability to chew. In a previous study34 it was determined that the number of unexpected/ unavoidable premature tooth contacts during gum chewing was also reduced by 50%.
Reduced muscle activity improved the subjects’ TM joint function in the opening and closing pathways. The lateral pterygoid being less disturbed allowed for freer and smoother joint capsule motion on top of the condyle. It is also possible that shortening of Disclusion Times resulted in decreased sympathetic tone, with subsequent reduced dystonia of the lateral pterygoid muscle lessening tension in both the disc and capsule. A number of studies have shown that sympathetic tone and trigeminal inputs may both jointly influence masticatory muscle hyperactivity.39–41
An additional benefit to this group of subjects was the increase in the mean Range of Motion (ROM) from 43.4 mm to 47.7 mm (p < 0.0002). Figure 9 illustrates graphically the statistically significant increase in the Range of Motion of the subject pool after all of the subjects underwent ICAGD, where the most restricted subjects showed the greatest increase. This increased ROM moved the mean value into the range of what is widely considered normal.38 Only twelve of the 43 subjects initially exhibited what is widely considered a limited range of opening (< 40 mm), but their limitations reduced the mean value significantly. Some of the patients with opening limitations increased a great deal (Figure 9) suggesting there were some possible partial or complete disc re-captures. The six subjects that were most limited in ROM increased their ROM the most post ICAGD.
When the JVA parameters of (> 300 Hz) and the ratio (> 300 Hz / < 300 Hz) are high they are indicators of some degree of degeneration within the Temporomandibular Joint.38,39 As was indicated in the methods, none of the subjects in this study had evidence of degenerative changes before ICAGD (one of the exclusion criteria). Thus, the lack of significant changes in these two parameters after ICAGD supports the contention that the group’s TM joints incurred no significant change in their non-degenerative status.
The statistically significant reductions in the combined post-ICAGD right and left Disclusion Times suggest that ICAGD made lateral excursions easier for the subjects to perform, which likely translated into better lateral pterygoid motion mechanics, resultant from the lateral pterygoid being less disturbed following ICAGD. Although the lateral pterygoid muscle contraction levels were not measured in this study (because it is a subsurface muscle and cannot be readily measured without invasive procedures), the known effect of ICAGD is to relax the masticatory muscles.26,31–34 The reduction in mean post-ICAGD Disclusion Time was significant, (p < 0.000001), and a consistent endpoint for occlusal adjustment. Results can be achieved within patients, between patients, and between two different occlusal adjusters, using computer measurements to guide coronoplasty to its endpoints (Figure 12).
ICAGD is a very different occlusal adjustment procedure compared to traditional, unmeasured Occlusal Equilibration.42–49 No pretreatment appliance therapy, jaw repositioning, bimanual manipulation of the mandible into Centric Relation, or TENS is required to affect its therapeutic action.14–16,26–32,34 All of the excursions that are recorded are produced solely by the patient in a natural way with the only slight influence being the T-Scan wafer. The lack of clinician mandibular control and/or orthosis represents a marked patient treatment advantage over unmeasured occlusal adjusting that attempts to capture a border position that’s rarely if ever involved in the functional movements. Most importantly, ICAGD definitively treats working side group function excursive contacts thereby resolving a significant contributor of high masticatory muscle activity levels compared to balancing side contacts.31 The T-Scan /BioEMG III and JVA technologies are bringing into question a foundation occlusal concept deemed acceptable by Equilibration theory,45,46 that is not highly compatible with neuro-physiology.33 Moreover, the long held “belief” in working side group function that includes premolar guiding teeth being acceptable versus balancing side contacts being the most problematic occlusal contacts, has likely limited the effectiveness of conventional Occlusal Equilibrations,47,50 which requires patients to use splints that are not needed with ICAGD.
The subjects’ physical improvements were observable solely due to the development of and the implementation of three synchronized occlusal technologies that measured, detected, consistently reproduced multiple data sets, and guided the corrections of the subject group’s occlusal contacts (JVA, T-Scan, EMG). This study’s noted improvements occurred despite the fact that no TM joint physical therapy, splint therapy, injection therapy, or other TMJ treatment was given to any subject at any time. Without these three technologies simultaneously measuring several different functional parameters none of these physical impairments could have been predictably detected or predictably and successfully treated.
LIMITATIONS
Despite the reporting of high-level statistical significance of the Disclusion Time changes, and the JVA improvements, there were a number of limitations in the study design. First, an inclusion requirement was that each subject’s anterior teeth couple or nearly couple. Although this simplified rendering treatment to the subjects, it eliminated any potential subject whose anterior teeth were too far apart to use as guiding teeth. Additionally, no subjects with severe internal derangements of the Temporomandibular Joints were included, restricting subjects to those who demonstrated mild TM joint pathologies only. Applying ICAGD to Class II, Class III, anterior open-bite, and patients with severe structural TMJ internal derangements for potential TM joint and lateral pterygoid functional improvement, (that some clinicians might be tempted to extrapolate from this study), should be avoided.
A second limitation was that electromyography measurements of the lateral pterygoid were not undertaken, so no assessment of changes in its hypercontraction levels from ICAGD treatment were possible. The use of surface EMG cannot gather lateral pterygoid muscle activity values, which could only be obtained by inserting a needle electrode through the skin and into the lateral pterygoid of each subject. Needle EMG greatly interferes with the normal function of the muscle it is measuring because a needle sits in the middle of the muscle body. Needle EMG can also render artifacts with every movement of the muscle. An added risk of inserting a needle into specifically the lateral pterygoid is the real possibility of creating a hematoma. As such, it was not possible to observe changes in the functional muscle contraction levels of the lateral pterygoid.
Another potential limitation was that no “control group” or “placebo contingent” was possible in this study. Since the whole point of ICAGD is to reduce the Disclusion Time and since placebo occlusal adjustment does not suffice for that, no placebo method was possible. As the study was designed to determine a measured treatment effect (changes in the JVA patterns after ICAGD), using the subjects as their own controls was necessary. To compensate for this limitation, the Student’s Paired t-test was employed because it can reveal the changes that occurred after treatment within each subject, while ignoring the typically much larger variations between different subjects. While the reliability of the statistical calculations cannot be questioned, the inferences of improved TM joint function are predicated upon the findings of previous studies involving control groups, that assessed the JVA patterns as they related to known TM joint pathologies and control subjects.38,39
An additional limitation was that two properly calibrated ICAGD clinicians made all of the pre-ICAGD and post-ICAGD recordings and performed all of the ICAGD treatments on all of the subjects. Differing clinicians would be expected to produce somewhat different ICAGD endpoints, rather than obtaining exactly the same end-results, subject to subject. ICAGD treatment end-result precision depends on the skill of the clinician performing ICAGD, and his/her skill level working with T-Scan excursive movement Disclusion Time data sets. Varying ICAGD precision could possibly affect the degree of JVA response to ICAGD in a different clinician’s subject pool. Therefore, this study’s results may not be representative of all outcomes by all clinicians who may practice without proper T-Scan/EMG/JVA training, or those that have not undergone definitive Disclusion Time Reduction and ICAGD coursework.
A final possible study limitation was that no protrusive excursions were recorded, analyzed or treated. Despite this exclusion, the JVA vibration patterns were markedly improved, indicating that protrusive movements may not be very involved in the opening and closing movements of the mandible during mastication. This study’s results concur with other ICAGD and Disclusion Time reduction studies where protrusive excursions were also not analyzed or treated, yet muscle physiology and symptom improvements were reported following ICAGD.14–16,26–34
CONCLUSIONS
Significant reductions in moderately pathologic TM Joint vibration patterns and a significant increase in the maximum opening and closing Range of Motion may be obtained by the experienced clinician adjusting occlusal contacts to create short Disclusion Times with the ICAGD coronoplasty. Significantly reduced vibrations of the capsule and/or the disc found within this study’s subject group suggested that ICAGD may have improved the functioning of the TM joint mechanics towards a more normal opening and closing motion. Therefore, the null hypothesis was rejected.
Statement of potential conflicts
RBK is a consultant to Tekscan, Inc. but receives no monetary benefit from sales. JR is the Chairman of the Board of Directors for BioResearch Associates, Inc.
Funding Statement
None.