INTRODUCTION
Temporomandibular Disorders (TMDs) include numerous physical diagnoses, which can have significant, negative effects on a patient’s quality of life, such that a reduction in the emotional wellbeing of a patient who lives with chronic pain, has been documented in the psychosocial dental literature.1 One sub-category, myalgia, has been shown to have particularly onerous effects upon life quality.2 Some authors have theorized that myalgia can be Central Nervous System (CNS) mediated, but to date there is no convincing evidence to support that belief. Regardless of the potential etiology, chronic pain of the masticatory muscles has been shown to be associated with negative emotional sequelae.3–5
Some authors claim that painful, chronic and dysfunctional TMD symptoms arise from both physiological causations, and emotional anxiety/depression precipitated by patient’s life stresses.4 The unproven Myofascial Pain Dysfunction Syndrome (MPDS) theory suggested that emotional stress exacerbated physical stressors upon the Stomatognathic system, which led to the appearance of chronic, painful symptoms.6,7
Additionally, psychologists and psychiatrists advocated that TMD patients overreacted emotionally to their chronic pain, whereby the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD)8 avoided the underlying physical pathology and postulated that structure breakdown or dysfunction were secondary to anxiety, depression, and/or somatization. Cognitive Behavioral Therapy (CBT), was then recommended to reduce a patient’s stress, to hopefully reduce clenching and grinding habits that could damage teeth, muscles, and the Temporomandibular Joints.9
Despite the fact that psychological treatment has been continuously promoted for decades, no published TMD treatment studies have shown cognitive behavioral therapeutic success. Furthermore, validation studies have not shown the RDC/TMD criteria as being adequately sensitive and specific to diagnose many physical TMD conditions.10
Another TMD theory advocates TMD is an occlusion-precipitated disorder.11–14 Although neither centric relation bimanual positioning,12 nor Myo-centric muscle-determined occlusal positioning13 have resolved all masticatory muscle TMD symptoms,15 they have had some success in treating TMD symptoms.16–19 One measured, computer-guided occlusal adjustment procedure that advocates the duration of posterior excursive contacts are neurologically responsible for muscular TMD symptoms, has demonstrated in multiple published studies that muscular TMD symptoms have an occlusal etiology. The Immediate Complete Anterior Guidance Development (ICAGD) coronoplasty reduces excursive movement Disclusion Times and significantly lessens masticatory muscle hyperactivity by minimizing periodontal ligament compression durations. Studies repeatedly show that ICAGD resolves many muscular symptoms.16–18,20–23
There is limited literature where psychological testing is used with TMD patients who undergo occlusal treatment.24 The Beck Depression Inventory - II (BDI-II) is a widely used, 21 question mood-measuring, emotional assessment device that reliably detects and scores degrees of depression.25,26 The specific aim of this study was to determine in a carefully selected group of TMD subjects, whether BDI-II scores would be altered by subjects undergoing measured, computer guided occlusal treatment.
METHODS
This study was a four-clinician project, where all treatment providers were ICAGD trained and calibrated by one expert ICAGD clinician (RBK). Eighty-three Occluso-muscle disorder (OMD) subjects (60 females and 23 males, a 2.6 to 1 ratio), elected to undergo the ICAGD coronoplasty for treatment of their pre-existing, chronic muscular TMD symptoms. All subjects were informed of the risks and benefits of all procedures, then filled out a) a Beck Depression Inventory – II scale, b) a 5-point qualitative symptom intensity scale, c) a 4point symptom frequency scale, d) a 4-point functional restriction scale and a 4-point headache frequency scale. Included subjects answered each questionnaire before undergoing ICAGD, 3 weeks later, and 3 months later to assess changes in their Depression Inventory scores and their Occluso-muscle symptoms at two time-points after undergoing ICAGD. The protocol, privacy, and informed consent procedures conformed to the World Medical Association Declaration of Helsinki, as amended in October of 2013 at the 64th WMA General Assembly in Fortaleza, Brazil (IRB # BIRB/99Z/2017). The included subjects agreed to participate after receiving full Beck Depression Inventory and ICAGD occlusal adjustment protocol disclosures.
The inclusion criteria were that these subjects experienced some chronic physical muscular TMD symptoms (such as chewing fatigue, jaw pain, weakness, clenching/grinding habits, morning jaw stiffness, temporal headache, minor non-painful jaw joint noises without locking or dislocating), may have previously used a splint, demonstrated excursive movement Disclusion Times > 0.5 seconds, and had anterior teeth that coupled or nearly coupled.
The primary exclusion criteria were subjects that demonstrated internal derangements of the TM Joint (closed lock, disk displacement without reduction, condylar avascular necrosis, loss of condylar height, or a tumor). Also excluded were any subjects who, after receiving ICAGD and BDIII disclosure, did not choose to participate.
Symptomatic Questionnaires
The Report of Painful Symptoms questionnaire asked about: Jaw Pain (without moving), Jaw fatigue, Facial tension, Clenching and/or Grinding of teeth, Temporal headache, Neck pain, Morning jaw pain, Migraine, Jaw Joint Pain, Ear Pain, Ear noise (tinnitus), Teeth sensitive to cold. These symptoms were scored using a five-point pain scale: (0 = no pain, 1 = mild pain, 2 = moderate pain, 3 = severe pain, 4 = very severe pain).
The Report of Frequency of Painful Symptoms questionnaire included the same chronic pain symptoms scored with a four-point frequency of occurrence scale: (0 = never, 1 = occasionally, 2 = often, 3 = always).
The Report of Functional Limitations questionnaire included: Difficulty chewing tough foods, getting food caught between teeth, able to chew gum, opening wide to bite a hamburger, difficulty swallowing, cheek or tongue biting while eating, cold sensitive teeth, hot sensitive teeth, eating only soft foods, scored with a 4-point scale (Never = 0, Occasionally = 1, Often = 2, Always = 3).
The Report of the Frequency of Various Headache Types questionnaire included
Debilitating headaches requiring a doctor visit, Mild headaches requiring over the counter medication, Light sensitive headache, Nausea when having a headache, Headaches that impact my work/school/fun, Headaches that were intense and throbbed, Upper neck tension/pain occurred with headaches, Headache pain present only in temples, “Mohawk headache”, and being 50 % disabled for > 11 days within 3 months. Each question was scored with a 4-point scale: (0 = Never, 1 = Occasionally, 2 = Often, 3 = Always).
The Beck Depression Inventory (BDI-II) estimates a subject’s level of depression scored on a 4-point scale, where for each question the subject circles their current feeling (question #4 below is “Satisfaction”):
0 I get as much satisfaction out of things as I used to.
1 I don’t enjoy things the way I used to.
2 I don’t get real satisfaction out of anything anymore.
3 I am dissatisfied or bored with everything.
The BDI-II is scored as the sum of all the answers to each question. 63 is the highest possible total, with zero being the lowest total. Total scores are compared to the BDI-II Index to determine a subject’s “Level of Depression.” In the Beck Index a score of 17 or higher indicates depression levels that may require treatment25,26 (scores of 1-10 are considered normal ups and downs; scores of 11-16 are a mild mood disturbance; scores from 17-20 indicate borderline depression; scores from 21-30 reveal a moderate depression; scores from 31-40 indicate a severe depression; scores above 40 are associated with extreme depression).
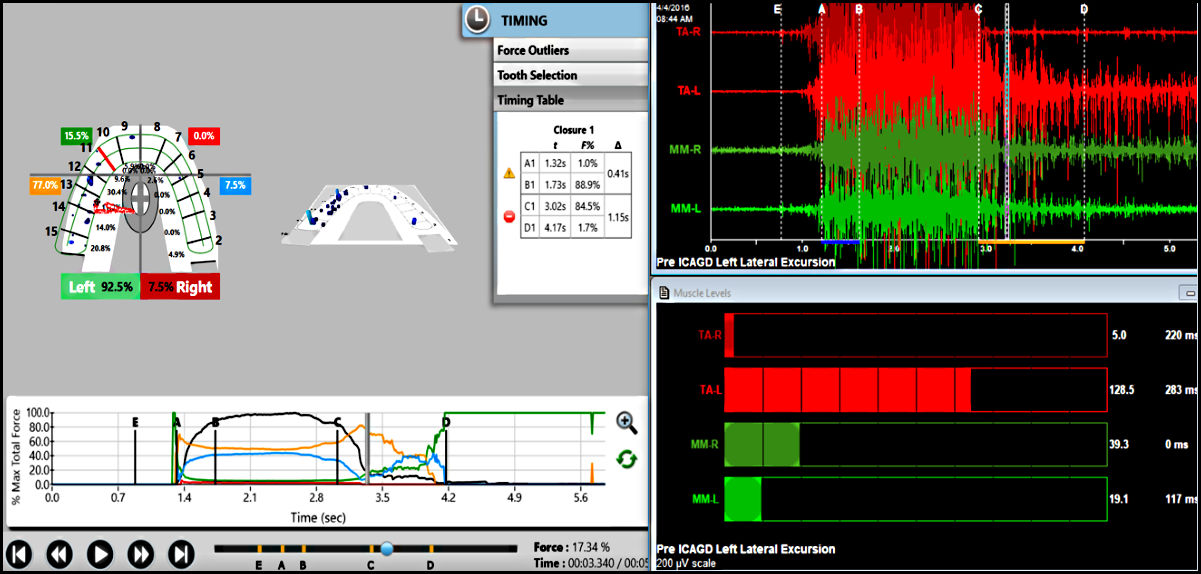
After completing the first BDI-II and the first sets of symptom scales, included subjects underwent the ICAGD computer-guided coronoplasty27 that attempted to resolve their chronic muscular symptoms. Pre ICAGD, each subject recorded two right and two left excursive movements with the T-Scan/BioEMG III (T-Scan 9.1, Tekscan, Inc. S. Boston, MA, USA; BioEMG III, Bioresearch Assoc., Milwaukee, WI, USA). Figure 1. The obtained pretreatment Disclusion Time and muscle activity level data was to be compared to the 3 week and 3-month recordings that followed initial ICAGD.

The ICAGD coronoplasty that was performed has been extensively described in eight previous publications.16–18,20–23,27 These articles explain in detail how ICAGD is properly performed so the authors have chosen to reference prior accounts, rather than explain the ICAGD protocol in this article once again. No counselling, medications, self-treatments, appliances or orthotics were used as part of any subject’s treatment.
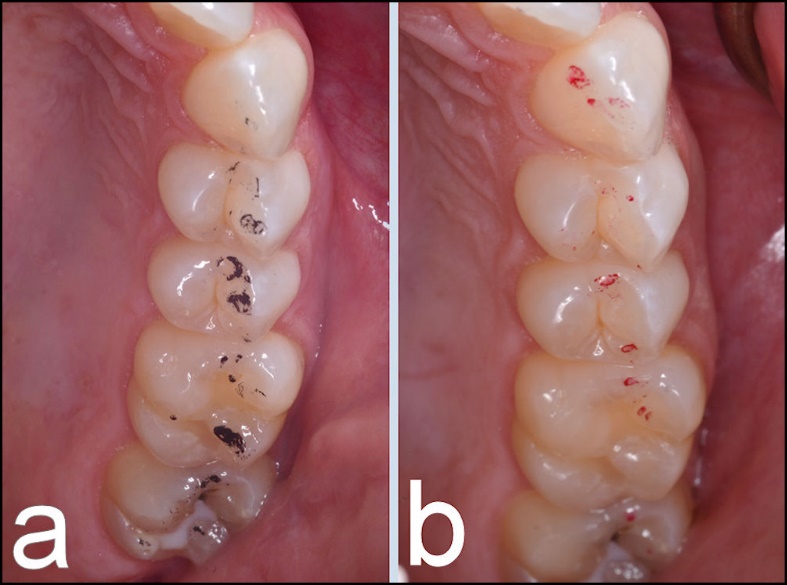
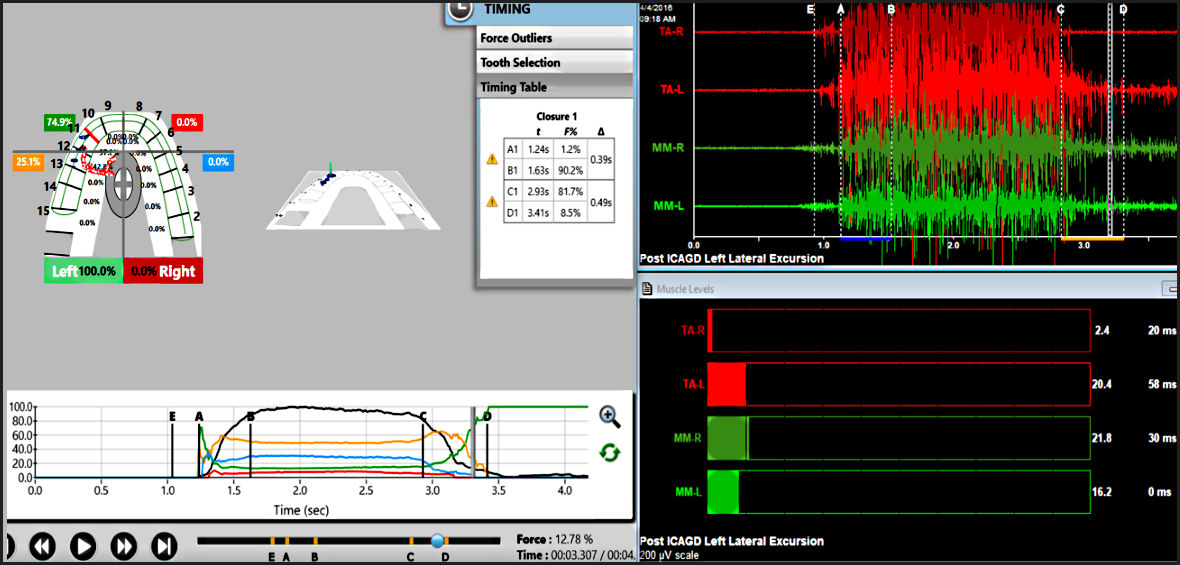
Figure 2a shows the pre ICAGD articulating marks that represent long Disclusion Time. Figure 2b shows the post ICAGD articulating mark changes resultant from ICAGD. After undergoing ICAGD, each subject recorded new right and left T-Scan/BioEMG III excursive recordings (Figure 3). Then 3 weeks and 3 months after ICAGD, new right and left Disclusion Time/muscle activity level data was re-recorded, while the subjects re-answered all symptom and functional surveys, along with the BDI-II.
_pre-icagd_upper_left_quadrant_of_articulating_paper_markings_showing_the_linear_feat.jpeg)

Statistical Analysis
The measured Disclusion Time data obtained pre and post ICAGD was averaged from each recording visit to calculate means and standard deviations (Table I). The pre to post ICAGD data sets were tested for significance with the Student’s Paired t-test. (Alpha was chosen at 0.05).
The pre ICAGD and the two Post ICAGD subjective symptom pain severity, frequency of occurrence, functional restriction questionnaires were all reported as ordinal number total scores, as no two patients exhibited the exact same symptoms. As there are many symptoms associated with (TMD), which accumulate both in The BDI-II answer numbers and severity as the condition worsens, there is no single symptom that is pathognomonic for TMD and the significance of any one symptom varies greatly within individuals. As TMD is a broad disease category, considering the total scores for pain severity, frequency, and functional restrictions, increases the resolution. As such, symptom total scores were tested with the nonparametric Mann-Whitney U Test (Alpha was chosen at 0.05).
Values from the 21 questions were totaled, as no single question alone indicates there is Depression. Considering the total score rather than individual answers again increases the range of depression that can be observed (0 to 63).
RESULTS
Table 1 shows the changes in Disclusion Time at a) pre-treatment, b) at three weeks post treatment, and c) three months’ post treatment. Statistically significant reductions in Disclusion Times were seen at 3 weeks (p < 0.0000) and 3 months (p < 0.0000) compared to pretreatment.
A significant mean Disclusion time reduction also occurred between 3 weeks and 3 months post treatment (p < 0.0109 – p < 0.0106) without an further treatment. Statistically significant and almost complete improvements in all levels of function were observed.
Tables 2-7 contain the results of the symptomatic and depression questionnaires completed pre ICAGD to 3 months’ post ICAGD. Table 2 details the totaled self-reported pain scores for twelve conditions compared from a) pre-treatment to between b) 3 weeks and c) 3 months’ post treatment. Significant reductions in pain were seen at both 3 weeks and 3 months’ after ICAGD treatment (p< 0.00001 in all instances).
Table 3 illustrates the frequency of pains for the twelve conditions scored in Table 2, compared at a) pre-treatment, b) at three weeks, and c) three months’ post treatment. Significant reductions in the reported frequency of painful symptoms were seen at both 3 weeks and 3 months after ICAGD treatment (p< 0.00001 in all instances).
Table 4 describes the levels of functional restriction at a) pre-treatment, b) at three weeks restrictions were observed within the initial 3-week period of observation (p < 0.00001). However, only a small statistical change in the restrictions was noted from 3 weeks to 3 months (p < 0.04364).
Table 5 illustrates the frequency of headaches at a) pre-treatment, b) at three weeks post treatment, and c) three months’ post treatment. Significant reductions were seen at 3 weeks and 3 months after initial ICAGD treatment (p < 0.00001 in all instances).
Table 6 shows the Mann-Whitney U Test of the Beck Depression Inventory total scores at a) pretreatment, b) at three weeks post treatment, and c) three months’ post treatment. Statistically significant improvements were seen in all three comparisons. (p < 0.00001). Pre-ICAGD, the mean and median scores were close, indicating that the distribution was not markedly skewed from treatment.
Table 7 displays the distribution of the totaled BDI-II scores of 83 subjects by time frame. 78 % of the subjects were moderately or severely depressed prior to ICAGD and 87 % were at least borderline depressed before treatment. Only 2.4 % were still at the borderline three months after treatment.
DISCUSSION
The outcome of this computer-guided occlusal adjustment/depression study contradicts all the previous articles where it has been concluded that the physical symptoms of TMD are secondary to agitated emotional states.4,6,8,9,28,29 This is the first publication to establish that reducing the physical pains also improves the emotional states of TMD sufferers. Most of the subjects in this study showed measurable signs of depression prior to ICAGD computer-guided occlusal therapy, but when pain was removed from this group, the level of depression nearly disappeared.
Previous authors have suggested that detrimental emotional states are present in TMD populations and have recommended that the psychological factors be evaluated in addition to assessing the physical factors that affect patients.8 But the theory that TMD is a psychosocially mediated condition, lacks sufficient scientific data to support that contention.28,29 In this group of Occluso-muscle disorder subjects, many physical symptoms improved after undergoing ICAGD. Which then quickly resolved the presence of depression. That outcome would suggest that eliminating frequent and chronic pain and their concurrent functional limitations can improve the emotional states of chronic TMD patients in just a few weeks.
These results do concur with the findings of previous ICAGD studies, where marked and rapid symptom improvements were reported following ICAGD.16–18,20–23 This study tracked symptom intensities and frequencies and the symptoms’ emotional impact on TMD subjects. Many painful symptoms improved 3 weeks after ICAGD was rendered (Tables 2 -5), which led to significant reductions in the subjects’ levels of depression (Tables 6 and 7) over the 3-month period of observation.
The functional restrictions almost completely improved within 3-weeks after initial ICAGD (Table 4). There are known, improved chewing mechanics that immediately follow ICAGD,23 which patients adapt to quickly. But with respect to the self-reported pain, the frequency of pain, and the functional restrictions post ICAGD, the improvements continued to occur at least through the 3-month study duration. The delayed response to treatment suggests that CNS adaptation occurs before the complete treatment benefit is realized.
The subjects’ measured symptom improvements were obtained by implementing two synchronized occlusal technologies, that measured their pre and post ICAGD Disclusion Times and their muscle responses, while clinically guiding four calibrated doctors to perform the same computer-guided treatment on different subjects in different cities.
LIMITATIONS
Some might consider the 3-month period of observation as a Limitation. This timeframe countered the possibility that in a longer study, some subjects could experience a lifestyle emotional trauma, if given more time for life’s events to turn negative (spouse death, contracting a terminal disease, child’s death, job loss, divorce). By limiting the study to 3 months there was less time for a life-altering event to affect a subject’s BDI-II responses, ensuring their responses were more related to the ICAGD treatment.
The inclusion requirement that each subject’s anterior teeth nearly coupled and all TM joints were stable, simplified rendering treatment to the subjects, but were limitations.
Another Limitation was that subjects were their own controls and not compared to any untreated control group. This study attempted to determine a measured treatment effect (changes Depression after ICAGD), by using the subjects as their own controls. To compensate, subjects completed symptom questionnaires and BDI-IIs previous to treatment and at two observations post ICAGD.
CONCLUSIONS
It is more likely that the depressed (88%) TMD subjects’ emotional states resulted from living with chronic painful symptoms and functional restrictions, rather than their life’s stressors causing their painful physical symptoms. When the chronic pain, frequent headaches, and functional restrictions were reduced after undergoing the ICAGD computer-guided occlusal adjustment, the group’s levels of depression dramatically reduced. The maximum physical benefits ICAGD accrued for 3 months after treatment.