


INTRODUCTION
Clinical experience confirms the fact that most edentulous patients are not satisfied with complete removable dentures as the best dentures are a poor substitute for the natural dentition. Many patients who wear complete dentures encounter difficulty adapting to their prostheses. Other patients may have adapted to dentures for several years but may have become maladapted as a result of regressive tissue changes (e.g. mandibular ridge resorption) or systemic health related conditions.
Mastication is the initial step in the digestive process and necessary for effective nutrition, health and a quality of life. An understanding of mastication is very important and the treatment of all the edentulous patients necessitates considerable efforts.1 Of the various modalities of treatment available to improve that experience, the present emerging trend is the placement of implant supported overdentures. The present case study uses the combination of EMG, T-scan and Jaw Tracking to evaluate the quality of masticatory function. It documents the subsequent changes in an edentulous patient, transitioning from edentulousness to a conventional removable complete denture and finally, to an implant supported overdenture.
In the 1970’s the introduction of titanium implants facilitated the implant-supported prostheses, and in the 1980’s implant-retained overdentures appeared. Subjectively, oral function appears to improve noticeably after the placement of implant-supported overdentures and need 1.5 to 3.6 times fewer chewing strokes than conventional complete denture wearers to obtain an equivalent reduction in food particle size.2 This is because the maximum masticatory force of an implant-retained denture is 60% to 200% greater than a conventional denture.3 Many studies have been conducted using traditional methods, which show implant-supported overdentures providing better masticatory efficiency and oral health-related quality of life than conventional dentures.4,5
There are several factors determining the chewing result. The teeth are important in the masticatory system. They form the occlusal area where the food particles are fragmented. This fragmentation depends on the total occlusal area and thus on the number of teeth. Another important factor in mastication is the bite force. The bite force depends on muscle volume, jaw muscle activity, the coordination between the various chewing muscles, the quality of the occlusion, the motion of the mandible and the functional condition of the temporomandibular joints (TMJ).6–8 The neuromuscular control of chewing also plays an important role in the fragmentation of the food.9
Large differences in oral function exist among various groups of subjects, such as dentate subjects, partial and complete denture wearers, and subjects with multiple implant retained overdentures.10 Both maximum bite force and masticatory performance are very significantly reduced when dentures replace natural teeth.11 Several studies have shown that masticatory function is reduced in people who have lost post-canine teeth, and in those who wear removable dentures.12 It is expected that implant-supported prostheses should improve the oral function and satisfaction in edentulous patients.13
OBJECTIVE
This case study was undertaken to evaluate and compare the masticatory motion, muscle function and relative bite force (EMG activity & T-Scan) between a conventional complete removeable denture and an implant supported overdenture.
METHODS & MATERIALS
A 72 old fully edentulous male with an ill-fitting lower denture who reported to the department of prosthodontics was selected to receive an implant supported overdenture. With his consent, this case represented an opportunity for the evaluation of any differences in relative bite force and timing using the T-Scan III. Additional muscle activity, masticatory timing, motion, velocity, and jerkiness during mastication were extracted from simultaneous EMG and incisor-point motion tracking recordings. Edentulous recordings were made, the implants placed, the conventional complete dentures made, at 3 months the denture was modified to fit the implants and recorded.
Medical history
No past medical history of dental disease or complaints of orofacial pains. Other than his ill-fitting denture the patient appeared to be in good health.
Edentulous history (Patient edentulous 1 year)
The treatment modalities were explained to the patient regarding an implant supported overdenture and an agreement was reached to fabricate a conventional complete denture first and follow that up with an implant supported overdenture. A primary impression was taken utilizing the muco-compressive technique using impression compound. The primary cast was poured, and custom trays fabricated. Final impressions were taken after border molding was accomplished with zinc oxide eugenol impression material. The secondary cast was poured, and record bases were fabricated with occlusal rims. A jaw relation was established and transferred to the articulator. A trial denture was fabricated using a set of semi-anatomical teeth. Denture was fabricated and delivered to the patient. The patient was recalled after a week for occlusal and masticatory analysis.
Occlusal and Masticatory Recordings
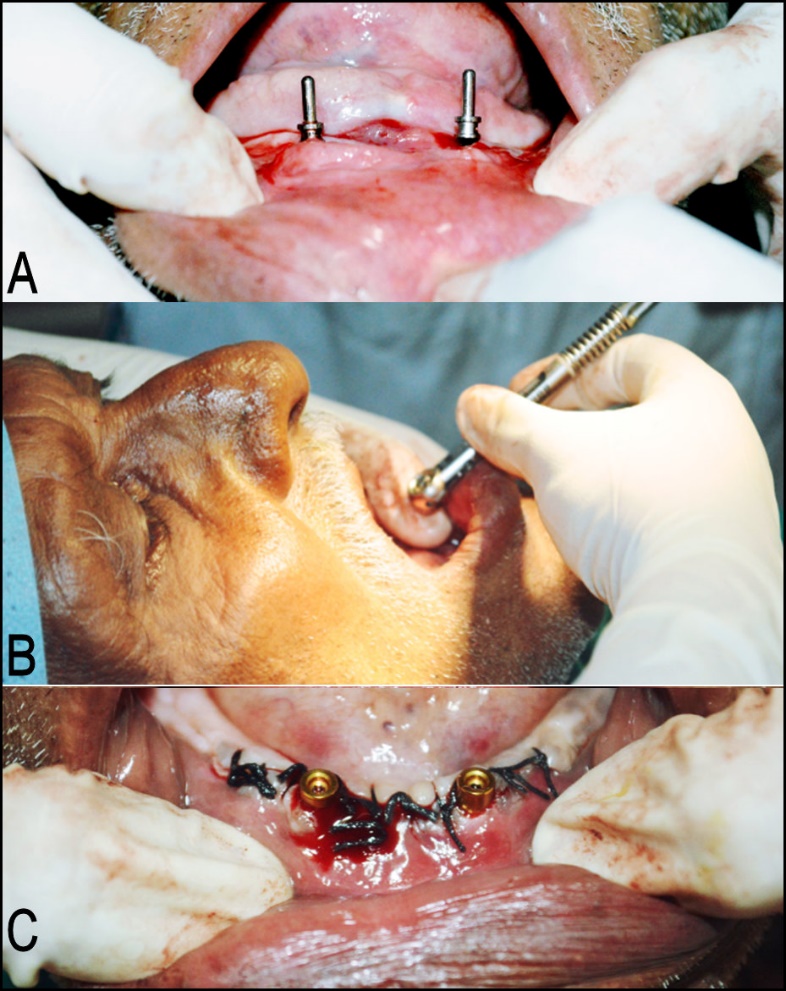
After the skin was cleansed EMG surface electrodes were placed over the regions of the superficial masseter and anterior temporalis muscles bilaterally. See Figure 1A. The electrodes were connected to the BioEMG III amplifier (BioResearch, Inc. Milwaukee, WI USA). See Figure 2A. Muscular activity and incisor-point masticatory movements were recorded simultaneously through the included BioPAK software.
Occlusal analysis was done with the software of the T-Scan III (Tekscan, Inc. South Boston, MA USA). Relative bite force was recorded and an occlusal equilibration was done to achieve bilateral force balance on the complete denture.
After the T-Scan occlusal analysis and adjustments, the jaw tracker was added for masticatory recordings. See Figures 1B & 2AB. The patient was asked to chew for 5 minutes on ‘Peanut Chikki’ (peanut and jaggery sweet) on the left and right sides, first edentulously and then with the conventional dentures in place. The patient was then recalled after one week to place the implants and then repeat the recordings with the implant denture in place.
Implant placement
Presurgical medical work-up was done followed by analysis of bone with the help of cone beam computed tomography (CBCT). It was decided to place two implants in the canine regions, which was localized with the help of lead foil markers placed on the denture. An implant size with a diameter of 3.7 mm and length of 11 mm (MIS system, India) was decided upon. Locator size was selected with a 5 mm collar height. See Figures 3ABC.
.jpeg)
Two implants were placed at canine regions, using the denture with lead markers as surgical guide, locator attachments were immediately attached. Suturing was done, denture loading was immediately done on the same day of implant placement. Post-surgical instructions were given and medications prescribed. Patient was recalled after a week for suture removal, occlusal and masticatory analysis.
Implant Supported Overdenture Analysis
Masticatory recordings were repeated using the same procedure and devices mentioned before with the help of the JT-3D jaw tracker, the BioEMG III and the T-Scan III. Since this was a single case study, all the recorded data in the three conditions were separated into 34 parameters to be analyzed. See Table 1. The incisor-point motions and separately the associated muscle activities, were analyzed with Student’s paired t test between the three conditions. Alpha was chosen as 0.05.
RESULTS & DISCUSSION
The thirty-four motion related parameters of the left-sided and right-sided mastication are shown in Table 1. With the single exception of the left-side comparison between the edentulous state and the conventional complete denture, the five other aggregate comparisons were significant (p < 0.05).
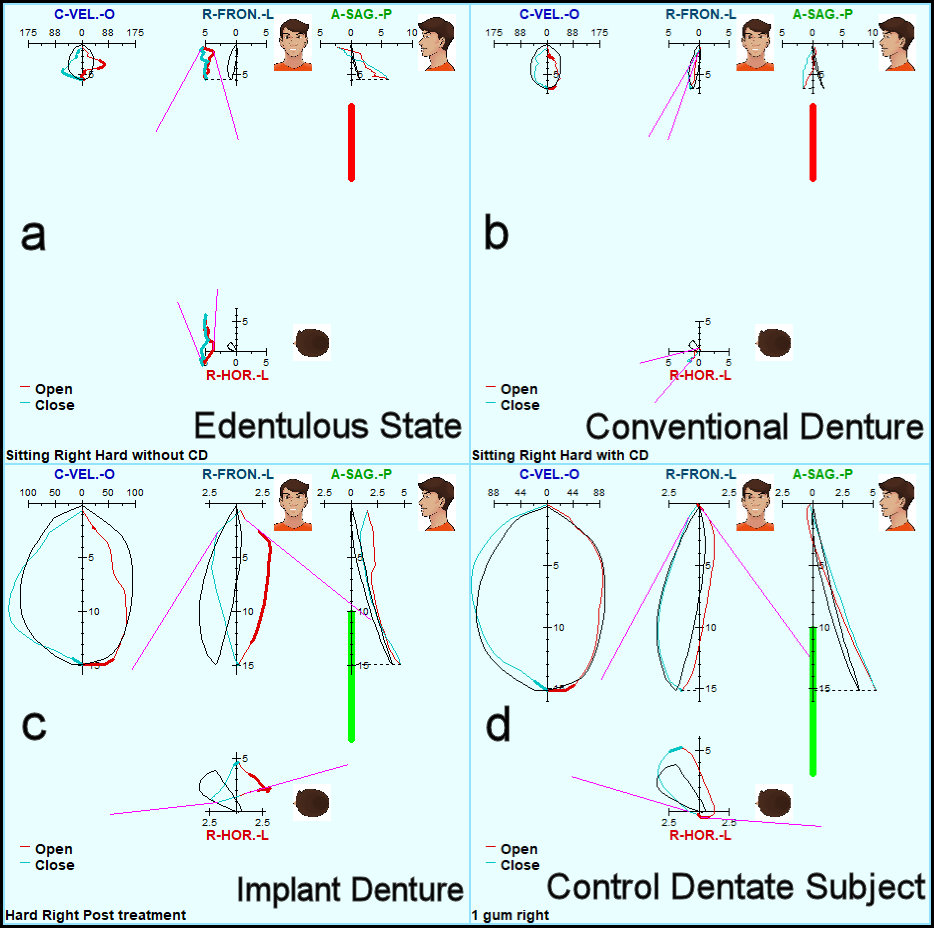
The mean cycle time for all edentulous mastication was 1.160 seconds, for all complete dentures 1.259 seconds and reduced to 0.696 seconds with the implant supported overdenture. The complete denture functioned with significantly less variability than the edentulous state (p < 0.05) and the implant-supported denture functioned much faster than both (p < 0.05). The mean vertical dimension of the Average Chewing Pattern (ACP) increased from 6.9 mm with the edentulous condition to 7.3 mm with the complete denture and to 13.6 mm with the implant supported overdenture. However, the amount of horizontal motion was greater with both the edentulous and the complete denture conditions. The mean total motion was not significantly different between the three conditions, the direction of the motion was different. See Figure 4ABCD. The more vertical ACP of the implant condition was similar to the ACP of a previously recorded control group with natural dentition. See Figure 5ABCD.

__are_even_more_dramatic_in_illustrating.jpg)
The average of the 4 Timings, (Opening time, closing time, occlusal time and cycle time) were compared using Student’s Paired t-test between the three conditions. See Table 2. The edentulous times were slower than the complete denture times (p = 0.0044), which were slower than the implant supported times (p = 0.00012).
The terminal chewing position (TCP) is the distance between the teeth (gums, dentures) at full bolus crush. The mean TCP for the edentulous condition was significantly larger than for the complete denture (p = 0.0357) and the implant denture (p = 0.0097), but the difference between the two dentures was not significant.
The maximum and average chewing velocities were not significantly different between the edentulous condition and with the conventional denture (p > 0.1610), but they were slower with the conventional dentures than with the implant denture (p = 0.0140) and when comparing the edentulous state with the implant denture (p = 0.0405).
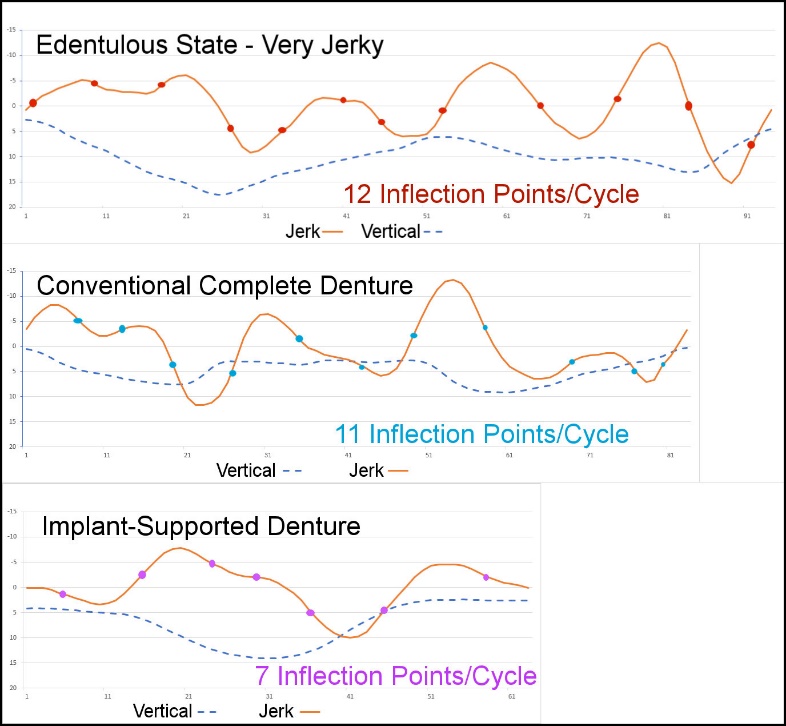
The jerkiness, as indicated by the mean number of inflection points in each cycle of mastication within the jerk function (d3s/dt3), is inversely related to smoothness of function. That is, the greater the number of inflection points, those transitions between the acceleration and the deceleration, the more jerkiness was present. The jerkiness decreased significantly from the edentulous state to the complete denture (p = 0.026) and significantly more from the complete denture to the implant denture (p = 0.0179). See Table 1 and a typical example in Figure 6.

Muscle activity during mastication
Table 3 presents nine EMG and timing parameters associated with muscle function during mastication. The Mean Area, (under the average distribution of muscle activity/cycle), multiplies the time with the microvolts of activity creating one parameter. Since it includes the duration and relative force level of a cycle, it is the best representation of the relative amount of effort involved per cycle. The effort decreased from edentulous to complete denture (p > 0.05) and decreased again with the implant denture (p < 0.05). The reason the effort is less with better function is not due to lower forces, but due to shorter cycle time. The amount of force needed is determined by the requirements of masticating the food, not the quality of the function.
The timing of the muscle activity adds another dimension to the analysis besides the opening time, closing time and occlusion time. The location of the peak in each muscle’s activity in relation to the end of closure is an indicator of the subject’s confidence. In dentate control subjects with good occlusions the peaks of all elevator muscles occur before the end of closure. In the edentulous state this patient’s muscle peaks averaged 151 milliseconds after maximum bolus crush, significantly later than those of the complete denture and the implant denture (p < 0.05).
Many crucial factors are responsible and directly involved with the proper functioning and maintenance of mastication: teeth, the bite force, muscle volume, jaw muscle activity, good TMJ function and the neuromuscular control of chewing all play important roles in fragmentation. The proper maintenance of these functions in turn helps in retaining a high quality of life and good health. In elderly people in particular, the quality of life, their nutrition and even some cognitive deficits can benefit from healthy mastication and good nutrition.8,14–18 For many patients, conventional complete dentures have allowed them to eat, to speak and to function in society more easily than they could without any prostheses. On the other hand, several studies have been conducted using traditional methods, which show implant-supported overdentures providing better masticatory efficiency and oral health-related quality of life than conventional dentures.19,20
More recently, the use of devices for quantitatively measuring mandibular motion has become more common in scientific and clinical use. Often, the goal has been to provide an objective basis for diagnosing musculoskeletal disorders, to monitor the progress of active treatment methods or to evaluate the functional results of prosthodontic treatment.21–23 The use of jaw tracker in this case report demonstrated the changes in masticatory motion from the edentulous state to a conventional complete denture and finally to the use of the implant-supported overdenture. The amount of improve-ment seen in this transition was measured and
observed in the data collected from the jaw tracker using previously recorded control subject data as the arbiter.
The reasons for calculating the average chewing pattern (ACP) are: 1) to cancel the random variations within the chewing pattern sequence that in normal subjects mostly represent bolus manipulation, 2) to reveal the average size, shape and speed of the underlying average pattern of function and 3) to provide a measure of the variability cycle to cycle of each pattern (the standard deviations). Masticatory dysfunction changes the overall shape of the ACP. It is usually distorted, and the most common changes seen are: 1) the size of the ACP decreases, 2) the velocity is reduced, and 3) the variability of the chewing motion pattern is increased. Thus, the duration of the chewing cycle time is extended as the patient chews more slowly and more tentatively.7,14 The recordings obtained from chewing of the Chikki with an edentulous mouth showed significant differences in the parameters making up the ACP when compared with the conventional complete denture and the implant supported overdenture. See Table 1.
Simultaneously, the EMG recordings obtained for calculating an Average Chewing Cycle (ACC) of the Temporalis and Masseter muscles are a characterization of the average muscle effort/cycle. If a malocclusion is present in a dentate patient, the mean area per cycle (summed muscle activity) usually increases, due to longer chewing cycles, while the Peak Amplitude may be decreased.14
The value of the ACP
The unaveraged Chikki chewing patterns of Figure 4 show visibly the transitions from the edentulous state to the conventional denture and to the implant denture as a continuous reduction in variability, increase in velocity and an increase in the vertical size of the pattern. Figure 5 shows the same data as ACP graphs, which cancel out most of the random left-right and antero-posterior motions, leaving just the vertical pattern of about 6 mm for the conventional denture, 7.3 mm for the conventional denture but a much larger 15 mm and more normal looking pattern for the implant denture. The black lines in the ACP graphs are the scaled mean normal patterns for reference. The red vertical lines in the edentulous and conventional denture patterns indicate the sizes of those two patterns are more than 2 standard deviations below the mean normal. The green vertical line in the implant denture graph indicates a normal range of vertical dimension.
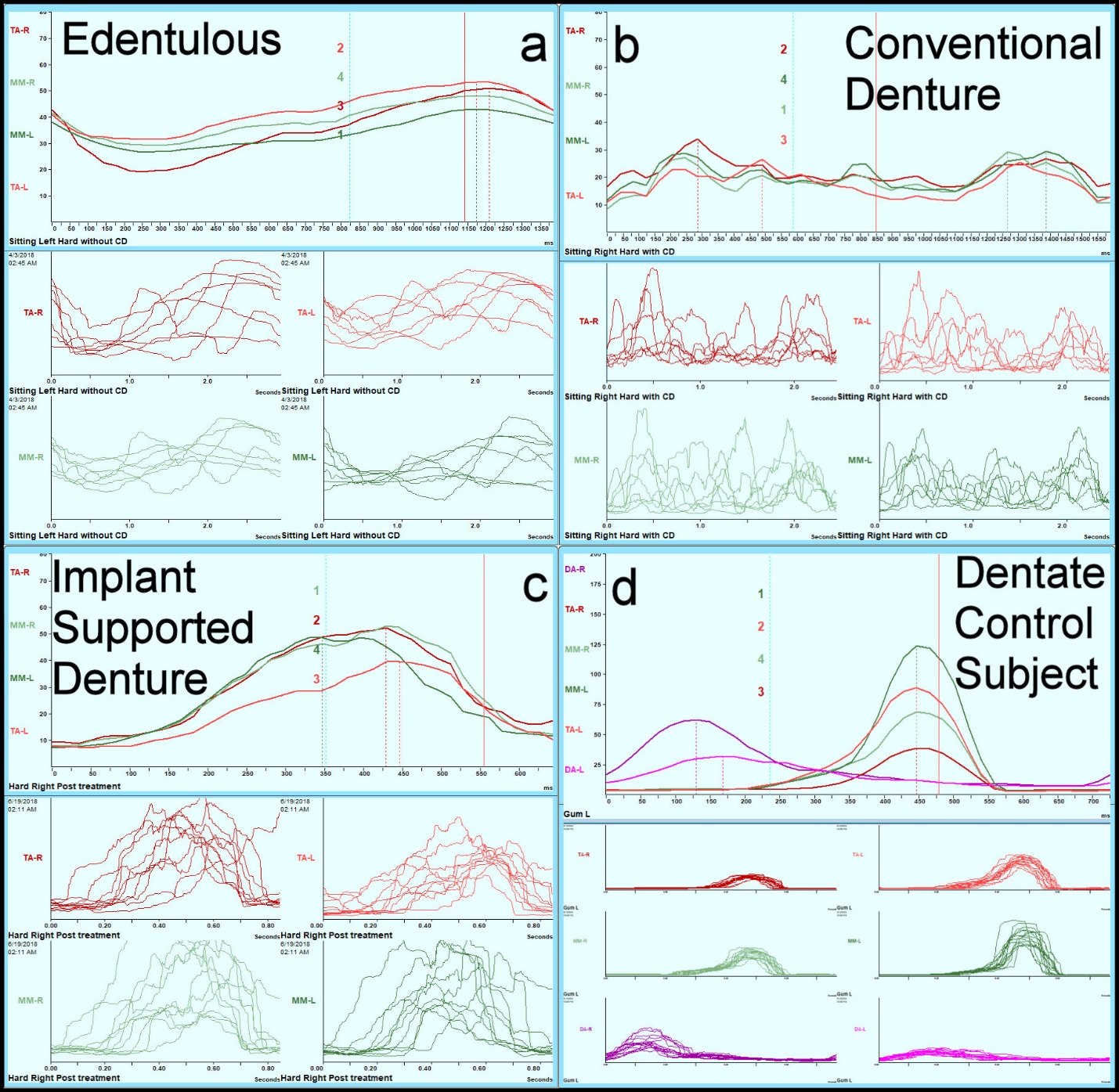
Average Chewing Pattern (ACC): The ACC is a characterization of the muscular effort/cycle for each muscle. Figure 7 shows the muscular effort for the masseter and temporalis muscles; a) for the edentulous state, b) for conventional denture, c) for implant denture and d) for a dentate control subject for reference. The upper half of each quadrant shows an average distribution of activity/cycle starting from the beginning of opening. The lower half of each quadrant shows all the individual cycles, giving a good visual indication of the variability, which for the edentulous case is nearly random.
__for_the_conventional_denture_(b)__for_the_implant_den.jpeg)
Conventional Complete Denture: Comparing the same patient’s ACP recordings with a conventional complete denture to the recordings in the edentulous state there was a small reduction in the cycle time and a small increase in the vertical size to the turning point. The chewing pattern of Figure 4 appears a bit more organized than for the edentulous state. The muscle function in Figure 7 is not substantially different between the edentulous state and the conventional denture. For two of the elevator-muscles the peaks of the contractions occur (on average) during opening rather than closing. This can be attributed to the need and the difficulty of attempting to stabilize the conventional denture during opening.24
Conventional complete denture ACC: The mean area for the conventional denture was less than for the edentulous state, but not significantly so. However, the peak amplitude was significantly less, the time to peak activity was significantly less, but the variability was significantly more. See Table 3. Subjectively, the mastication activity does not appear to be much improved compared to the edentulous state. It is possible that this patient needed more than three months to adapt to the new complete denture.25
Implant Supported Overdenture ACP: Precisely the same data were collected from the patient after the conventional complete denture was replaced with an immediately loaded implant supported overdenture. A dramatic change in the shape of the ACP was seen and the overall value for chewing cycle time reduced to an average of 0.749 seconds. The shape of the implant ACP appears to be much closer to the normal shape by the dentate control subject. The increase in the chewing rate has been seen in other studies.25 It is not likely that faster chewing by itself was responsible for the improvements, since forcing a higher than intrinsic rate tends to reduce the level of mastication performance.26
Implant supported Overdenture ACC: The mean area of the muscle activity with the implant denture was significantly less than for both the edentulous state and the conventional denture. This suggests less effort was needed in chewing with the implant denture. The peak amplitude was not different probably because it is related more to the force needed just to crush the bolus. However, the variability was significantly less with the implant denture in place (p < 0.05). See Table 3. In the graphs of Figure 7 it is visually apparent that the muscle activity patterns of the implant supported denture appear closer to that of the control dentate subject than the other two. It is likely that there will be more improvements in this patient’s mastication as he adapts to the new situation for some months.
Limitations
This case study of one subject does not begin to represent every possible outcome. As a clinical study the skill of the clinician is also a factor in the outcome. The T-Scan measurements were recorded with the same T-Scan wafer each time as some variation between wafers occurs. However, the wafer very gradually degrades, which might have occurred. EMG electrodes were carefully applied on the superficial masseter and anterior temporalis each recording session, but some small difference in the placement could have occurred affecting the measurements. That would not have affected the consistency or lack thereof. The alignment of the jaw tracker is an important requirement that requires due diligence for good data. The magnet positioner reduces the probability of error but does not eliminate it. The characteristics of the bolus affect how chewing progresses and a soft bolus may have shown less difference because a tougher bolus tends to reveal any dysfunction more dramatically.
CONCLUSIONS
From the EMG and motion data analyzed, there were significant improvements in several aspects of this patient’s masticatory function. As the patient transitioned from masticating in an edentulous state, to the conventional denture and ultimately to the implant-supported overdenture, significant improvements were revealed. The size, shape and velocity of the movement patterns and the function of the muscles improved. The improvements between the conventional denture and the implant-supported one are most likely due to the greater stability of the implant denture.
Statement of Conflict Potential
J Radke is the Chairman of the board of directors for BioResearch Associates, inc. No other potential conflict was declared by any of the authors.
Funding Statement
No funding was received.