


Introduction
Dental implants are a predictable modality to restore a biomimetic dentition but can incur complications of crestal bone loss and mechanical breakdown, ranging from abutment screw loosening to fracture of the abutment screw, abutment or implant. It is intuitive that mechanical problems are directly related to the level of occlusal force but the effect of occlusal overload versus bacterial challenge on peri-implant bone loss has been less clear.
Preclinical experiments have the advantage of visualizing results on the histologic level. Kozlovsky et al used a dog model to compare the effect of occlusal trauma from implant abutments in premature occlusion with non-contacting abutments, both with and without ligature-induced gingival inflammation. Only the inflamed tissue sites demonstrated bone loss, which was amplified by occlusal trauma, however the magnitude of the effect of inflammation was predominant compared to the occlusion.1 Miyata et al placed implants in monkeys with a superstructure of 100u, 180u or 250u excess height and controlled inflammation by weekly hygiene. There was a direct relationship between the extent of excess height and the amount of peri-implant bone loss indicating the adverse effect of occlusal trauma.2 Heitz-Mayfield et al placed bilateral implants in dogs with one side in supra-occlusion and maintained daily hygiene. They found no bone level or density changes between sides in the absence of inflammation.3 Several systematic reviews reiterate these conflicting conclusions.4,5
Ethical concerns prevent exposing test subjects to traumatic forces in the human model, so top hierarchical randomized controlled trials are not possible and observational studies are used. van Steenberghe et al showed in a narrative review examples of bone loss from excess occlusal force.6 Bone loss was evident on the abutment adjacent to a long prosthetic cantilever but not on one adjacent to a short cantilever. Bone loss was demonstrated from bruxing directly on overdenture abutments but not on the adjacent abutment without wear facets. Merin documented complete radiographic osseous repair of a tissue level molar implant with significant infra-bony defects, but no peri-sulcular inflammation, after only an occlusal adjustment (OA).7 Tawil radiographically documented the development of infra-bony defects on previously stable multiple implants after placement of an unstable overdenture.8 Complete resolution of the defects to the original bone levels was shown after a new prosthesis was fabricated. Wiskott et al radiographically documented the formation of infrabony defects with clinical mobility on previous stable implants after 4 months of interim restoration placement.9 After occlusal correction of the interim restoration mobility resolved and the bone reformed close to the original levels. Passanezi et al documented radiographically bone crest stability at a 2-year examination and bone loss to the 6th implant thread at 6-year examination when the patient reported bruxism. Complete radiographic reformation of the bone crest was seen 4 years after treatment with an occlusal device.10
Misch et al stated that occlusal overload is related to the implant design, bone density and the magnitude of force and is an etiologic factor in peri-implant bone loss.11 Fu et al concluded in their systematic review, “It is obvious that a positive correlation between occlusal overloading and peri-implant marginal bone loss exists.”12 They endorsed occlusal evaluation as part of maintenance visits. Dario documented the occlusion in 100 implant restoration patients with digital occlusal analysis to create an optimal occlusion.13 He found that nearly half the patients required continual OA over 18 months to correct hyper-occluded crowns.
The clinical implication of this research is that the dentist needs to diagnose occlusal problems and create a treatment plan that minimizes force on restorations to avoid peri-implant bone loss. The occlusal design of the implant restoration is one of the few factors that the dentist can completely control. The clinical case presented shows precise occlusal analysis that explained the patient’s problem set and verification of a therapeutic occlusion that created an optimal environment for a future implant-supported restoration.
Case presentation
Diagnosis
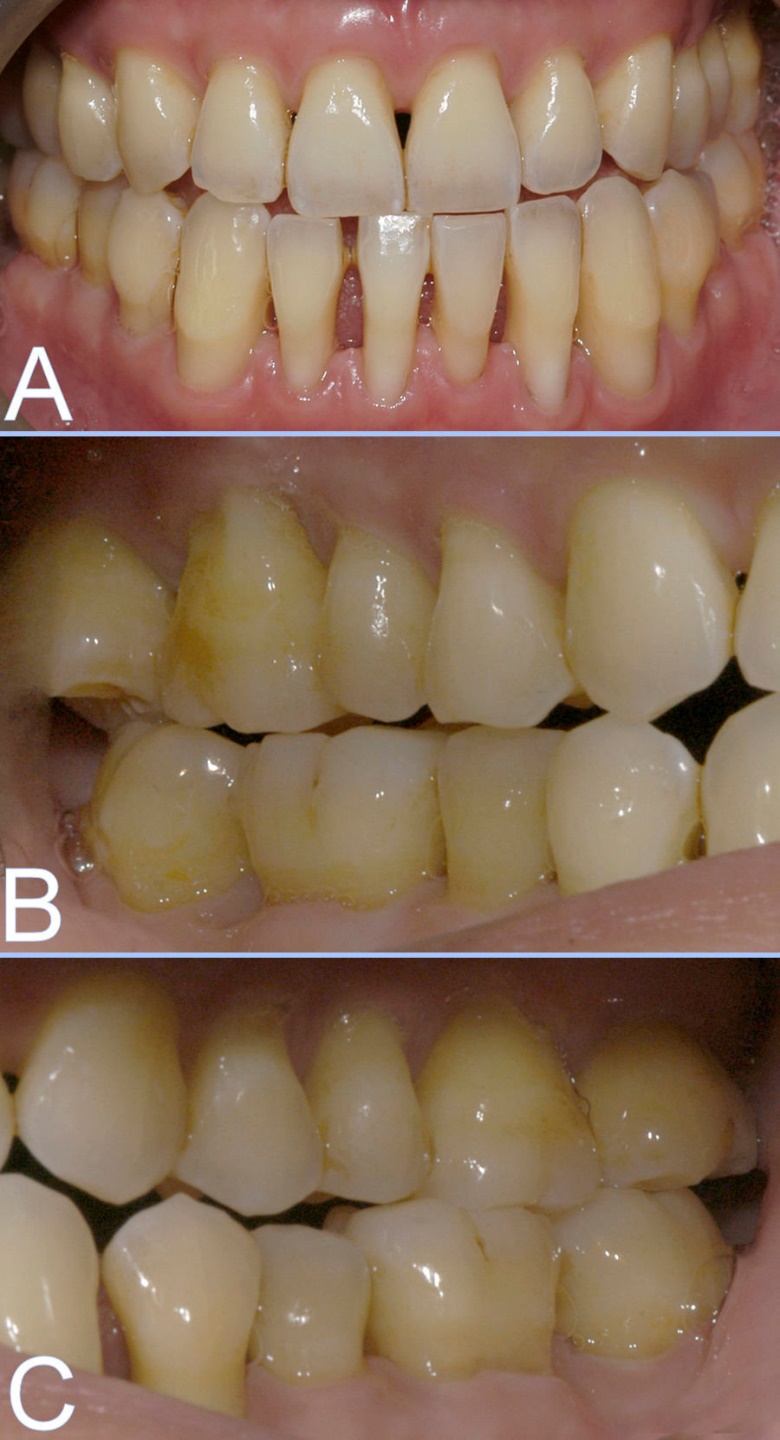
A 35-year-old male was referred by his periodontist with the chief concern of the mandibular anterior sextant with advanced bone loss, fractured lingual retainer, displaced left central incisor, an uncomfortable bite and enlarged gingival embrasures. Figures 1A, 1B, 1C, 1D and 1E.
_preoperative_clinical_presentation._reduced_periodontium_was_uninflamed_wit.jpeg)
_lost_palatal_wire_of_the_orthodontic_retainer_and_generalized_lack_of_enamel_we.jpg)
The patient’s medical history was not significant and his dental history included orthognathic surgery with bilateral sagittal split osteotomy at age 22, 4 rounds of orthodontics and full mouth root coverage grafts. There was no soft tissue pathology, caries or tooth fracture, periodontal inflammation or probes > 3 mm, temporomandibular pain or limited mandibular motion. Gingival recessions remained after root coverage procedures.
His post-surgical, post-orthodontic Class III relationship prevented proper anterior teeth guidance in lateral excursions and premolar and molar lateral and protrusive excursion interferences were evident. The bonded lingual retainer was fractured at the mandibular left central incisor which was displaced facially 1mm with Class I+ mobility.
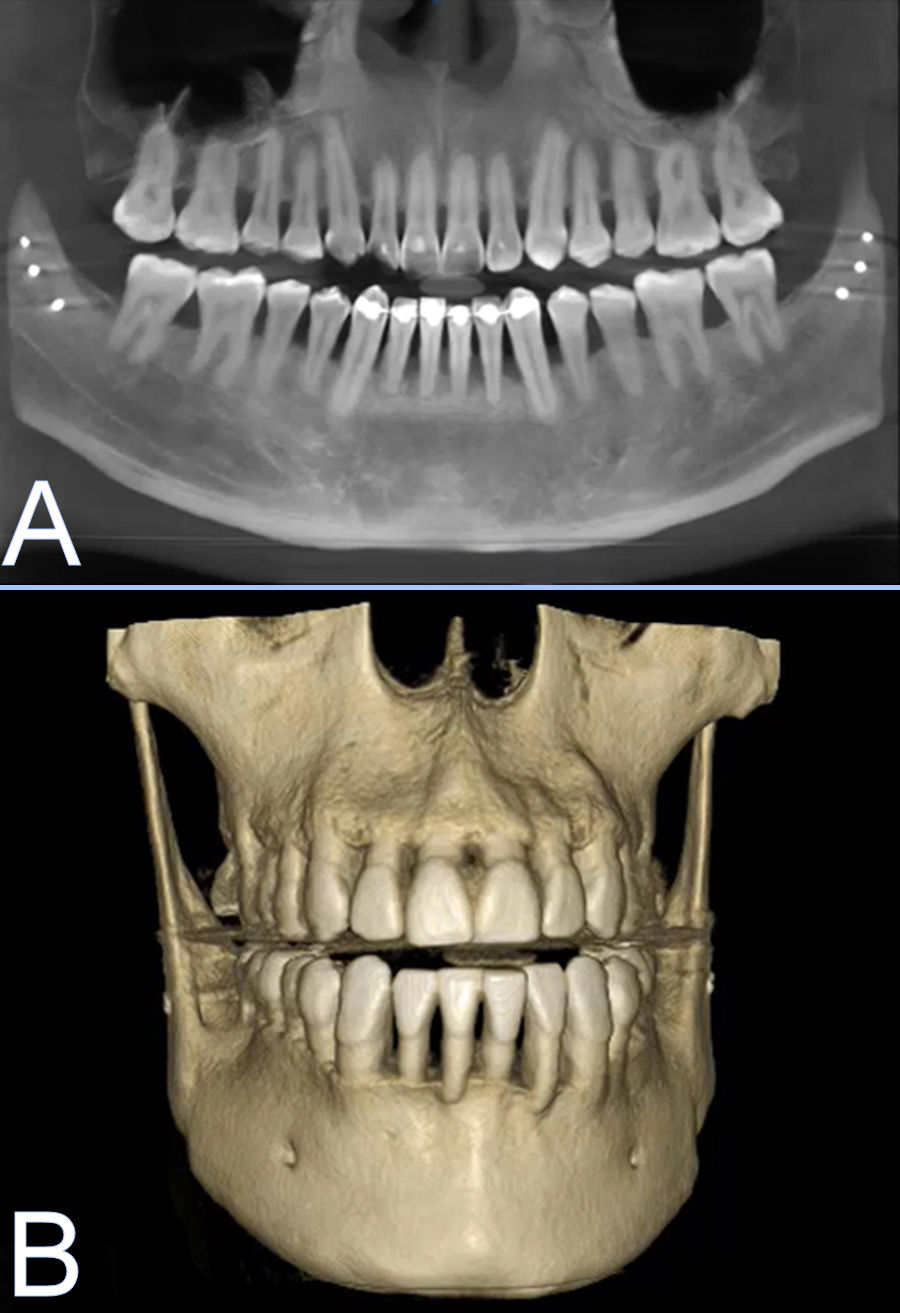
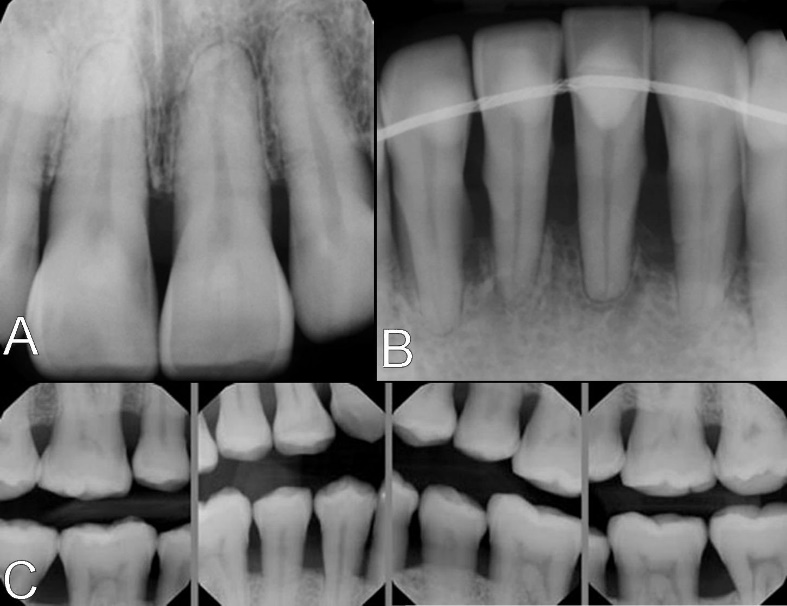
The cone beam computed tomogram showed advanced bone loss on the mandibular incisors with 20% of the root remaining in bone (Figures 2A & B). Plain digital radiographs showed this bone loss in detail along with moderate bone loss on the maxillary incisors, contrasting to the mild moderate posterior teeth interproximal bone loss. Figures 3A, 3B and 3C.
_2d_and_(b)_3d_images_showing_advanced_bone_loss_in_.jpg)
_moderate_maxillary_anterior_bone_loss__(b)_.jpeg)
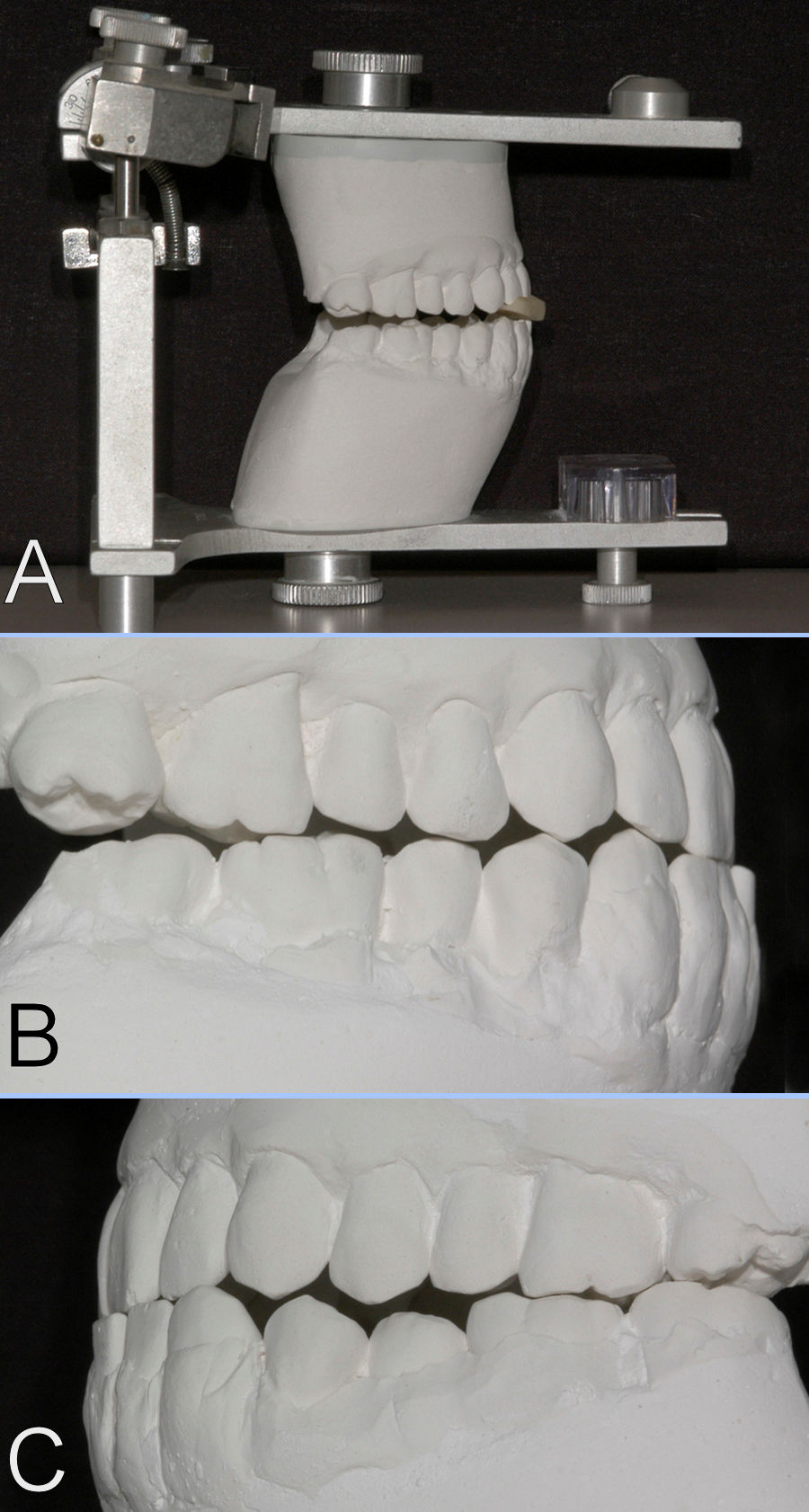
Mounted diagnostic casts on a semi-adjustable articulator were verified in centric relation (CR) with a marked anterior deprogrammer, showing consistent lower incisor contact when the patient closed in the arc of closure on his own and with bimanual guidance.14,15 Figures 4A, 4B and 4C. Stone models are not compressible, unlike the natural dentition, and showed the posterior teeth separation by this interference for accurate treatment planning. The mounted casts demonstrated an arc of closure interference on the lower right central incisor. The right maxillary 2nd molar and 2nd premolar were above the occlusal plant and the mandibular left premolars were below the occlusal plane without contact of the antagonist teeth by about 1.0 mm. Occlusal force from the arc of closure interference corresponded to the mandibular fractured retainer and the most extensive sites of periodontal bone loss.
_mounted_diagnostic_casts_verified_in_centric_relation._anterior_deprogramme.jpg)
Additionally, the patient’s maxillary nightguard showed pronounced wear facets from shear forces from the lower anterior teeth instead of providing nocturnal bruxism protection. The maxillary and mandibular fractured ortho-dontic retainers were consistent with occlusal overload risk factor for bone loss. The <1 mm slide CR to maximum intercuspation (MI) discrepancy indicated that subtractive OA to create multiple arc-of-closure contacts would be conservative without perforating enamel.
The posterior open occlusal contacts could be closed with additive OA using enamel-bonded composite resin and the normalized contours of the maxillary 1st premolars could provide guidance in lateral excursions.16
Consult with the orthodontist and periodontist discussed vertical extrusion of the mandibular incisors for implant site development. The consultation with the patient recommended correcting the occlusal problem as the first priority to avoid the existing occlusal overload problem on the planned implant restorations.
Treatment
The mandibular anterior malalignment was addressed first to establish a normal incisal plane. The orthodontist did not recommend orthodontics for alignment because severe tooth mobility was expected after retainer removal and manual repositioning was suggested instead.
The composite resin and wire fragments were removed with diamond burs but there was no mobility on the incisors except the displaced left central incisor which was Class I+.
The teeth were etched with 35% phosphoric acid (UltraEtch; Ultradent) and coated with unfilled resin (Clearfil SE Bond; Kuraray). The left central incisor was manually repositioned, with firm pressure, in line with the adjacent teeth and secured with a new bonded retainer. 3 mm sections of woven polyethylene (Ribbond Original; Ribbond) were embedded in microhybrid composite resin (Renamel; Cosmedent,), placed interproximally extending to the line angles of the teeth and light-polymerized. The 4-5 mm long composite resin reduced the gingival embrasures and did not cover the lingual surface for tongue comfort. Figure 5.

Composite resin was bonded on the posterior teeth with absent occlusal contact, using the same protocol, with interproximal stainless-steel bands placed to avoid bonding adjacent teeth together. Full mouth OA then established point occlusal contact marks in the arc of closure with no excursive contact on the posterior teeth, except the maxillary 1st premolars which provided anterior guidance line marks.17 Figures 6A, 6B & 6C.
_20-micron_accufilm_marking_showing_arc_of_closure_contacts_in_centric_relat.jpg)
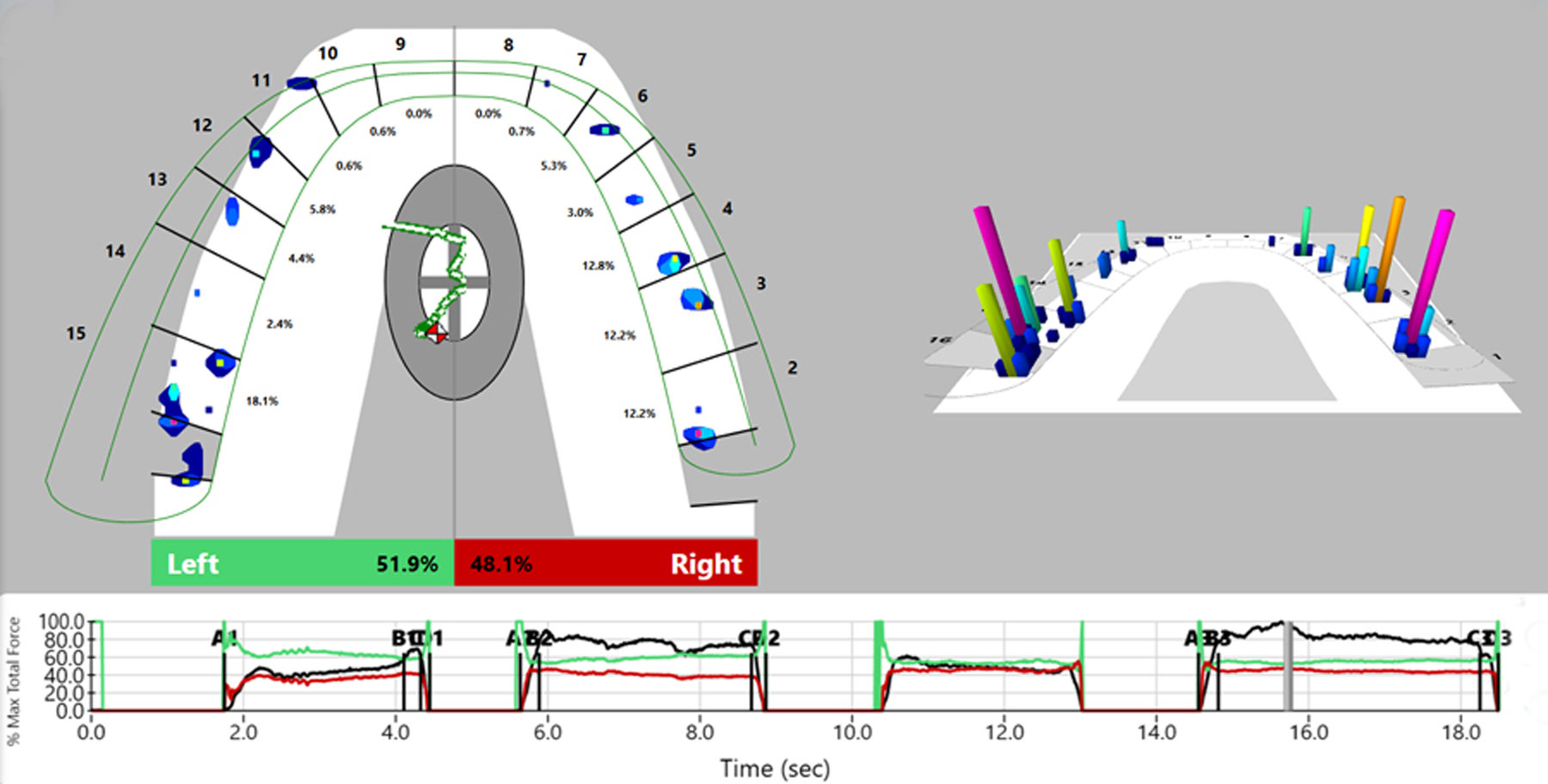
The mandibular anterior incisal edges were adjusted for an even incisal plane and lighter contact than the posterior teeth. Digital occlusal analysis (T-Scan, Tekscan) confirmed the optimized occlusal contacts shown by 20-micron ink ribbon (Accufilm, Parkell). The patient reported complete comfort with his bite and the new retainer design. Figure 7A.
_2d_and_3d_displays_shows_bilateral_even_contacts_wi.jpg)
The absence of significant mobility on the mandibular incisors changed their prognosis and countered the urgency to restore this site with definitive implant-supported restorations. The patient’s excellent hygiene and optimized occlusion allowed maintenance of the splinted mandibular incisors as an interim alternative.

Discussion
Orthodontics and orthognathic surgery give the clinician direct control over the occlusion and the forces that affect teeth during function and parafunction. A treatment goal for both these modalities is an occlusal relationship that provides long-term stability and comfort for the patient. However, these specialists do not follow patients over the long term and when this goal is not achieved it is critical for the general or restorative dentist to diagnosis the problem.
Accurate occlusal analysis with mounted diagnostic casts allows the dentist and patient to visualize the arc of mandibular closure and excursive contacts in three dimensions. These contacts explain the occlusal component of the patient’s problem set but are not accurately assessed by intraoral inspection.14 Stone casts clearly show arc of closure interferences since they are solid and not compressible like teeth in their sockets. Intraoral inspection does not accurately assess these interferences because a tooth can have a significant premature contact but intrudes on closure, allowing adjacent teeth to mark with inked ribbon and obscuring the occlusal problem. The patient receives objective information and a visual understanding of their problem. When restorations are done without this analysis, the dentist preserves the error of the discrepancy from centric relation to maximum intercuspation, which can be significant.
When there is a small CR-MI difference, there is little practical value to duplicating casts and doing trial additive or subtractive OA. A 1 mm discrepancy would indicate a 0.5 mm adjustment to each arch which may not incur significant loss of enamel or restorative material.
A large CR-MI difference indicates the need to measure the difference between the casts before and after trial procedures, so treatment planning is quantified. Adjusted duplicate diagnostic casts verified in CR produce a precise preview since the anatomical arc of closure is preserved. Subtractive OA of the posterior teeth can predict whether the anterior teeth will have proper anterior guidance contacts or an open occlusal relationship. When all trial adjustment is done on one arch, the occlusal matrix technique can show the reduction volume of each adjusted tooth.18 An acrylic resin matrix is fabricated on a duplicate diagnostic cast to record tooth contours, relined with bite registration material and seated on the trial-adjusted cast. When set, the registration material is removed and measured with calipers to predict the volume of reduction at each site.
Additive OA conservatively bonds composite resin to enamel to augment the shape of teeth for proper closure and excursion contacts. Alternatively, cast gold or ceramic can be bonded. The duplicate diagnostic cast can be waxed to preview the occlusal result and a clear silicone index fabricated to facilitate direct intraoral or indirect laboratory adhesive onlay placement.19 Additive OA on anterior teeth also decreases the amount of tooth reduction needed on posterior teeth to develop a programmed occlusion.
Lateral guidance was placed on the most anterior tooth possible since force is greater in a Class III lever system on the more posterior teeth, amplifying adverse torque. The longest track possible was developed on the composite resin augmentation without distorting the shape of the tooth. The inclination of this track was minimized to slightly separate the posterior teeth and decrease stress on the premolar root. The maxillary 1st premolars had good periodontal support with no mobility after augmentation. Group function contacts were avoided as lateral contact in any direction increases muscle activity, total force on teeth and occlusal wear.20
Physical casts and direct digital occlusal analysis on the patient are complementary techniques and were combined to take advantage of each. Physical casts show the clinician and patient the location of the arc of closure interference and the mandibular shift from this interference to MI. Physical casts show the overlap and overjet of all teeth and occlusal plane problems. They allow duplication and trial OA and occlusal waxing to preview and accurately predict the final results.
Digital occlusal analysis shows the timing and relative force of occlusal contacts with great sensitivity, providing additional preoperative diagnostic data and postoperative evaluation of OA and restorative procedures. This is a critical clinical advantage compared to interpreting ink markings which do not accurately assess the occlusal problem due to the intrusion of teeth as described above. Additionally, ink marks only show whether teeth do or do not contact, they do not show the force or duration of contact. Clinical research consistently demonstrates that dentists cannot correctly interpret which ink mark is premature by its size or color, misleading the clinician during occlusal procedures.
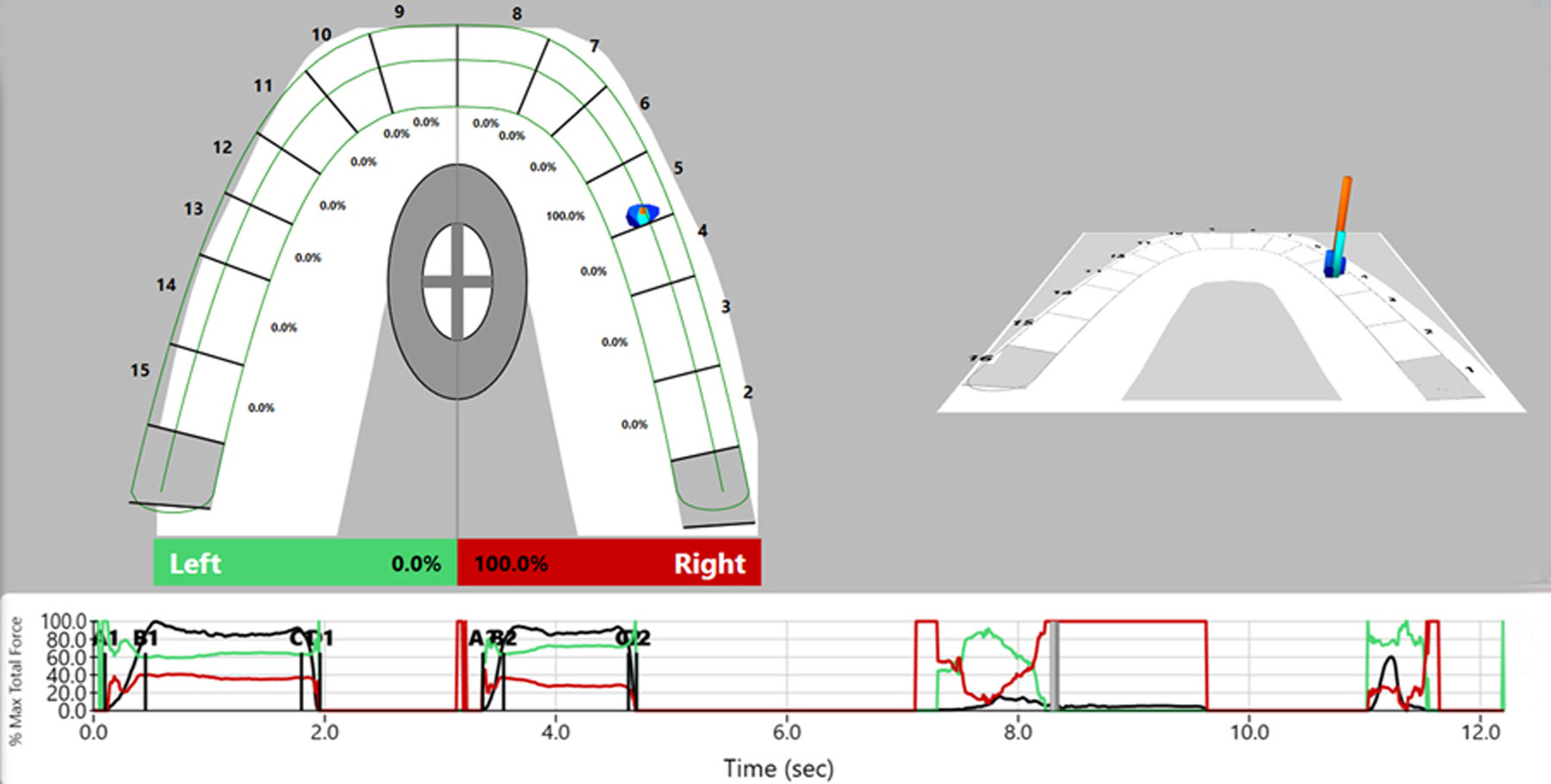
When patients have an arc of closure interference, they avoid repetitively traumatizing the tooth and are programmed to close differently to distribute force over more teeth. Arc-of-closure interferences of the posterior teeth typically show an anterior and lateral shift from the initial arc-of-closure incline contact into maximum intercuspation. This often results in wear and mobility on the teeth at the endpoint of the CR to MI shift instead of the interfering tooth. Anterior teeth arc of closure interferences, as in this post-orthognathic surgery patient, result in a similar anterior and lateral shift. In this patient, the arc-of-closure interference contact and the lateral shift contacts on the anterior teeth as well as the inappropriate anterior splint contacts resulted in a force overload on the anterior sextant periodontium. The patient could not escape the traumatic contact during the day or with nocturnal use of the splint, resulting in fracture of the orthodontic retainer, bone loss and the displacement of the incisor.
Most implant restoration literature focuses on definitive treatment. However, an essential decision for the patient and clinician is when to treat. Each patient has different concerns and preferences, but with all patients the clinician has a responsibility to discuss the longevity of maintaining the existing dentition. If there is no progressive loss of bone, placing implants later, so they have less years of maintenance and waiting for further technological advances, could be a better decision.
The referenced studies accept that occlusal overload amplifies peri-implant bone loss and show this overload can be an independent risk factor in non-inflamed sites. In reality, all the patients have some level of bacterial inflammation on implant restorations, so these risk factors act in concert. Although the dental literature gives general guidelines on prosthetic contours to align forces along the implant axis and avoid destructive lateral torque in an effort to keep bone stress between 2.0 and 4.0 MPa, the patient’s bone properties may not be average in the implant site.21,22 The clinician doesn’t have complete knowledge of the patient’s bacterial and occlusal overload risk factors, so optimizing the occlusion to minimize adverse force and ensure patient comfort represents best treatment. Prior to implant placement and definitive restoration, both the periodontal and occlusal environment should be prepared to support long-term success.
Conclusion
Preclinical randomized controlled studies and clinical observational reports support the importance of occlusal analysis in diagnosing and treatment planning implant-supported restorations. Recognizing the effects of force imparted to the supporting bone at the diagnosis, restoration and maintenance stages of patient care is as important as understanding bacterial challenge. Mounted diagnostic casts verified in centric relation and digital occlusal analysis provide accurate, objective information facilitating precision in diagnosis and treatment. Treatment of occlusal overload by conservative additive and subtractive OA can stabilize the dentition prior to definitive implant restoration or serve as an interim treatment.