




Background
The presence of a TMJ disc “stuck” to the eminence has been documented in the dental literature, either with the disc in a normal position or a displaced position.1–3 Arthrocentesis has been applied to break adhesions and release disks.4–6 It has been suggested that sliding of the disc in the TMJ is enabled due to the presence of phospholipids protected by hyaluronic acid (HA) that constitute an efficient lubrication system.7 “Joint overloading may be associated with uncontrolled production of reactive oxygen species (ROS) that causes degradation of the HA, followed by the exposure of the phospholipids to lysis by phospholipase A2 (PLA2).”7 If the lubrication has been defeated, the apparent adhesion of the disc may not be the case. Rather a suction with respect to the eminence may be responsible for the immobility of the disk.7 This has been supported by the ease with which some disks are reportedly released by arthrocentesis.7
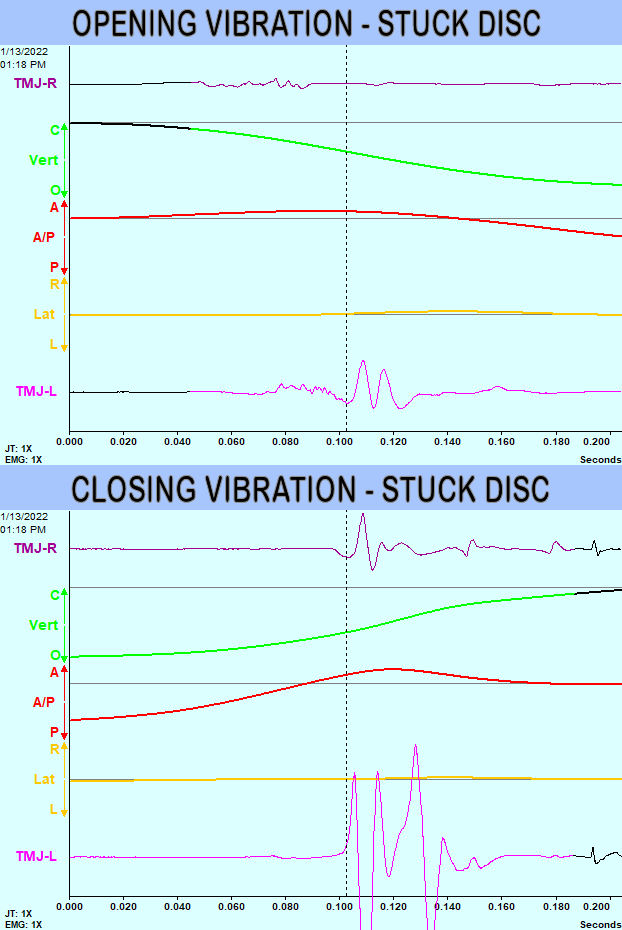
Although much of the literature describes stuck discs associated with a limited opening closed lock, occasionally a stuck disc may occur with a normal range of opening. If the disc is stuck in the normal closed position, the condyle must pass in front of the disk to allow it to translate fully. This situation produces a louder click on closing than on opening, which is an indication of a probable stuck disc.8 Because Joint Vibration Analysis (JVA) can quantify the intensity of TMJ vibrations, JVA combined with incisor-point tracking (IPT) can reveal when the closing vibration is substantially louder than the opening vibration for an internal derangement that includes a normal range of motion (at least 40 mm).9–14 See Figure 1. Note that the cyan color indicates closing and the red indicates opening.

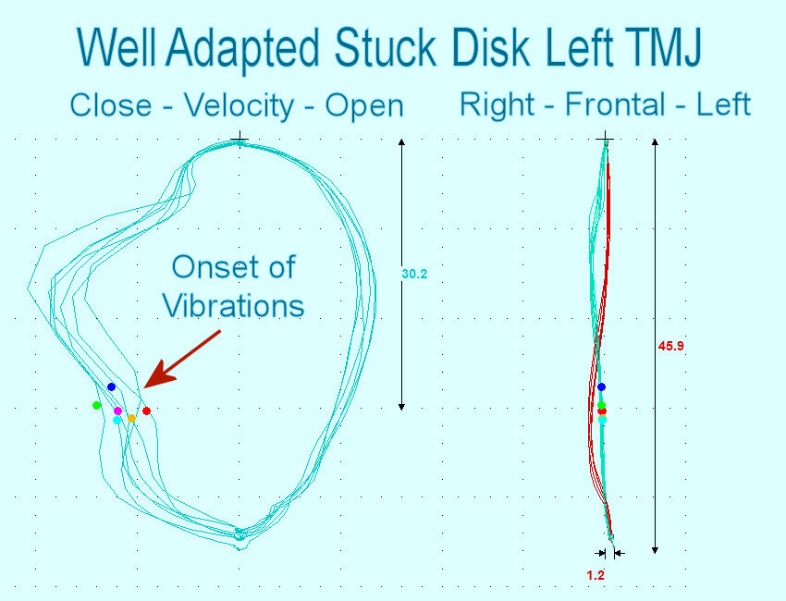
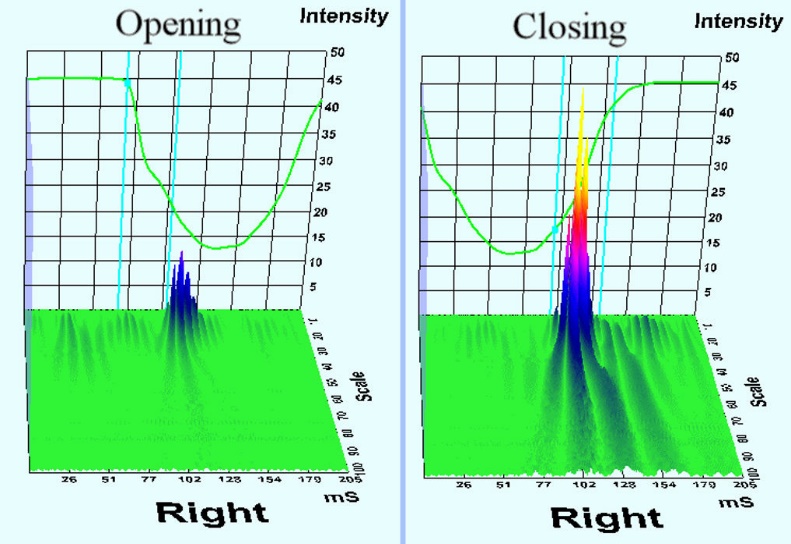
In Figure 2 the closing velocity is clearly more disturbed than the opening velocity. While the opening velocity is smooth, a sudden acceleration is visible immediately after the disc reduction that occurred during closure, as indicated by the onset of each vibration. The normal range of motion (45.9 mm) and relatively straight frontal pattern eliminates a diagnosis of unilateral permanent disc displacement without reduction. The Wavelet Transform View - Figure 3 - reveals a 3-dimensoinal view of the vibrations that includes the timing, frequency content and amplitude.


Case study
MRC, a 53-year-old female examined in September 2020, suffered from twice weekly headaches, tinnitus, hearing loss and described a loud noise in her left TMJ consistently during closure from a wide opening. She had previously received a tympanoplasty in 1985 and had non-extraction orthodontic treatment in 2005.
The patient retained 28 teeth, some included prosthodontic restorations and a Class I occlusal relationship. Figure 4.

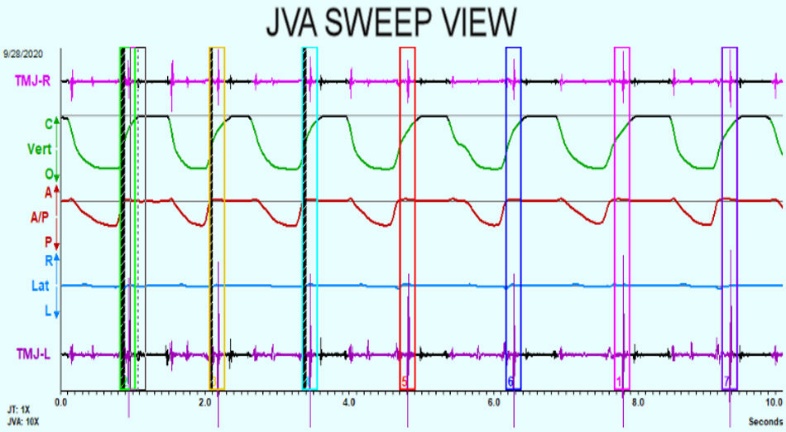
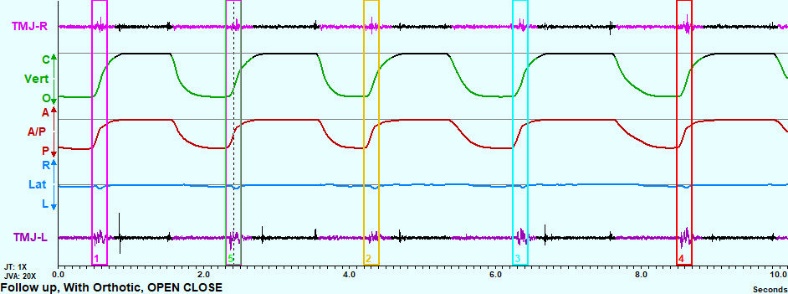
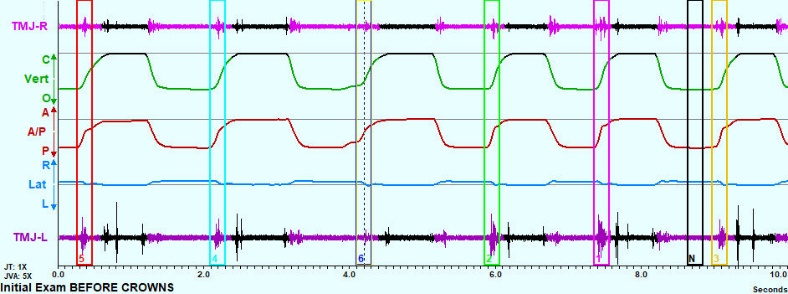
The JVA Sweep view indicated a larger closing vibration than opening vibration emanating from the left TMJ during the initial examination on 28 September 2020. See Figure 5.

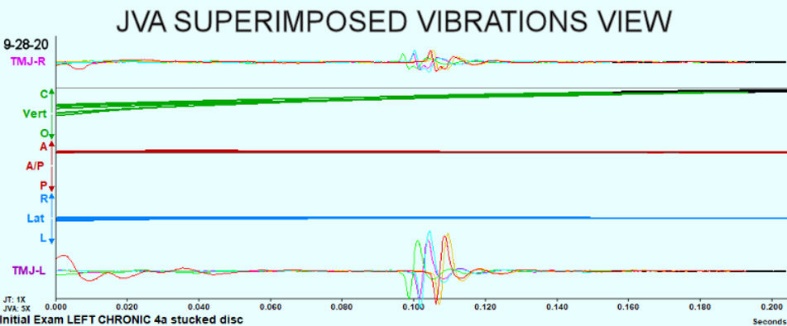
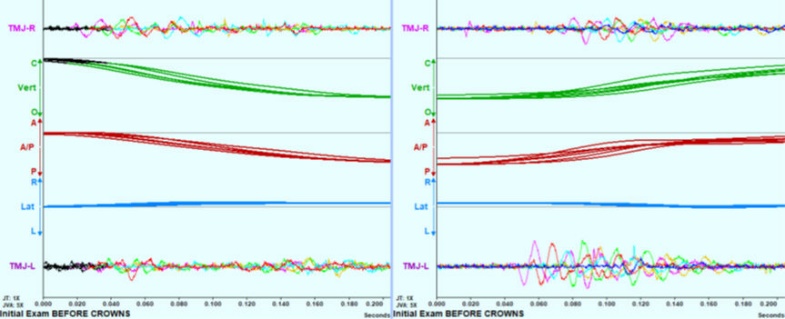
The view of the Superimposed Vibrations revealed that the waveform exhibited a consistent one-cycle high intensity with a short-duration. This type of waveform is associated with a disc reduction event. A disc that reduces during closure suggests that the disc is stuck to the eminence. See Figure 6.

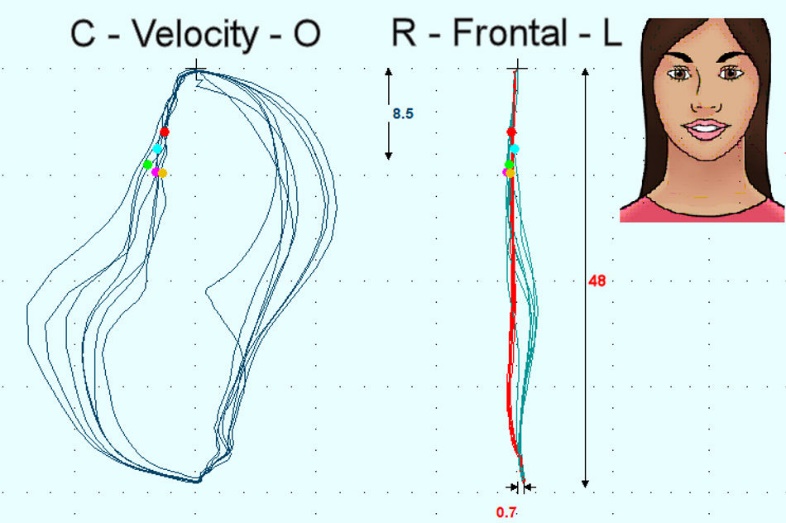
The Frontal Plane and Velocity view reveals a consistent late closing vibration location. See Figure 7.

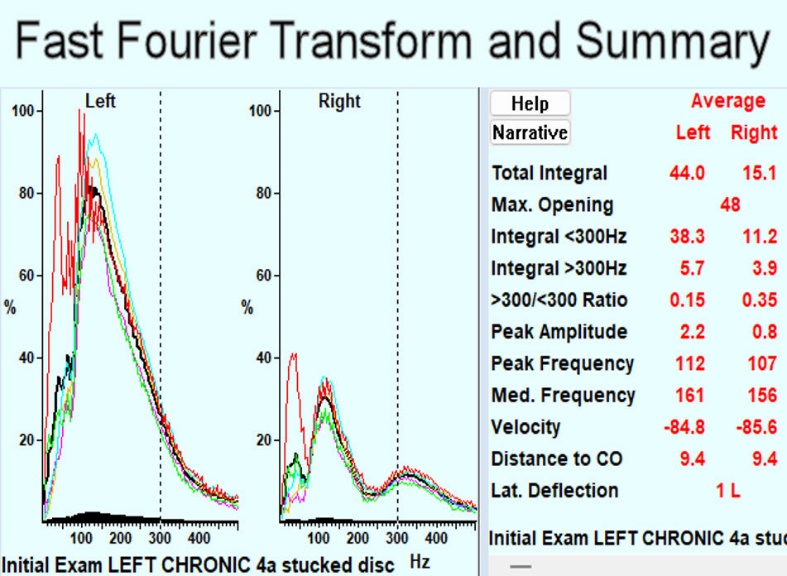
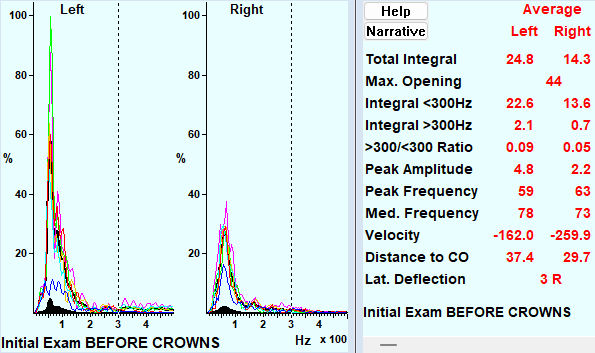
To evaluate the intensity of the vibration the Fast Fourier Transform is used to convert the data from the time domain into the frequency domain and plotted such that the X-axis represents frequency and Y-axis represents intensity. Then the intensity at each frequency is added together to create a Total Integral. The Total Integral represents the area under the averaged FFT frequency Distribution curve. See Figure 8. NOTE: The averaged Total Integral of 44 in the left TMJ is not considered high intensity as far the the population of internal derangement patients is concerned. It is only a medium intensity level, which indicates a chronic condition rather than an acute one.

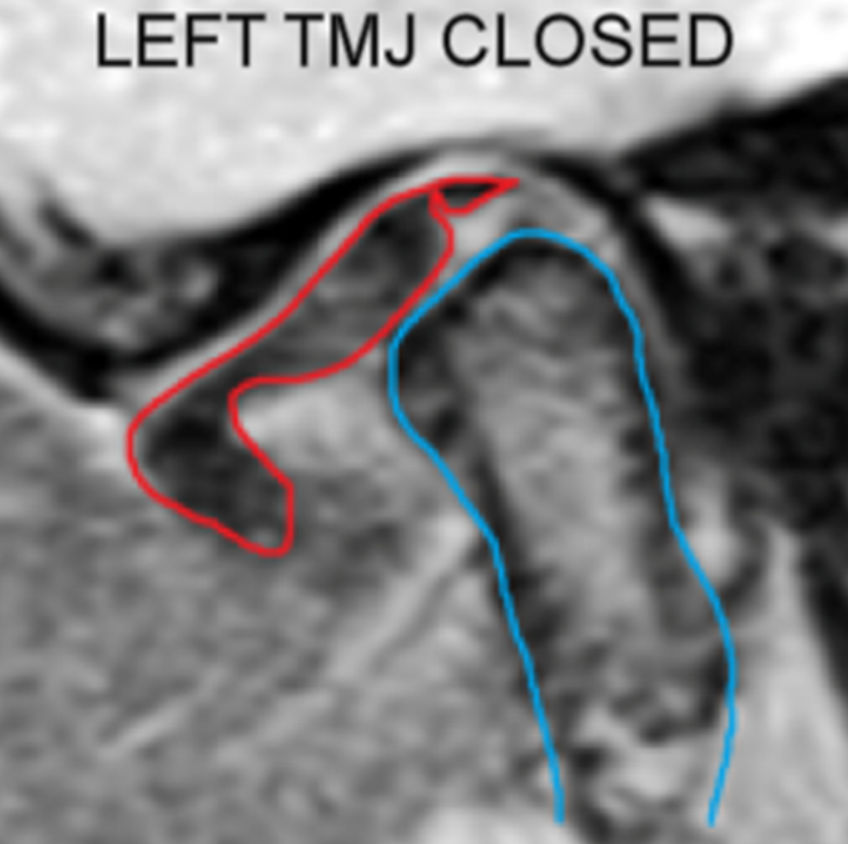
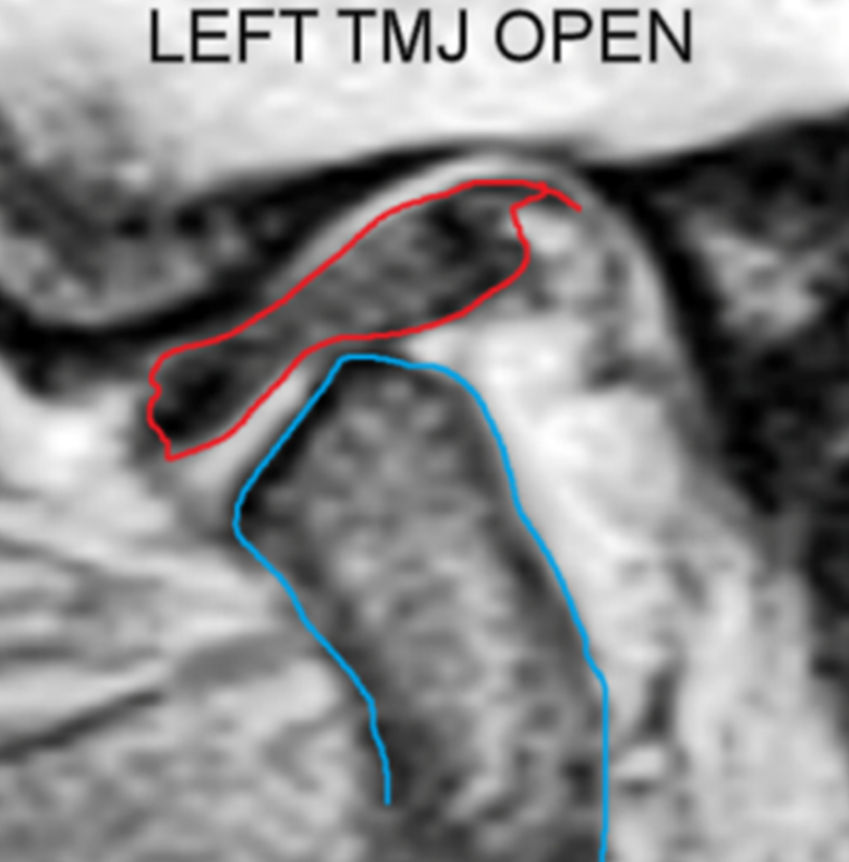
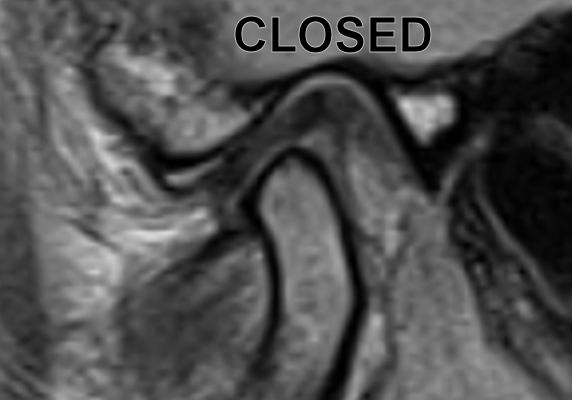
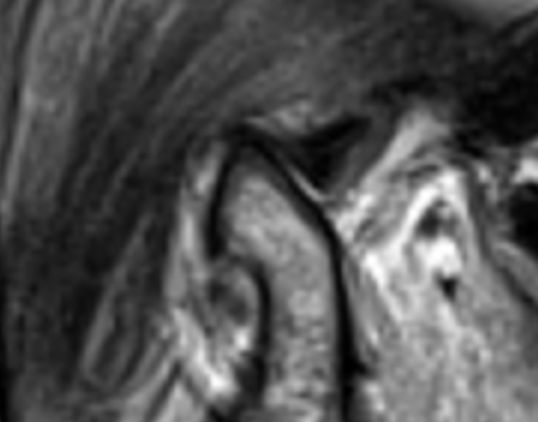
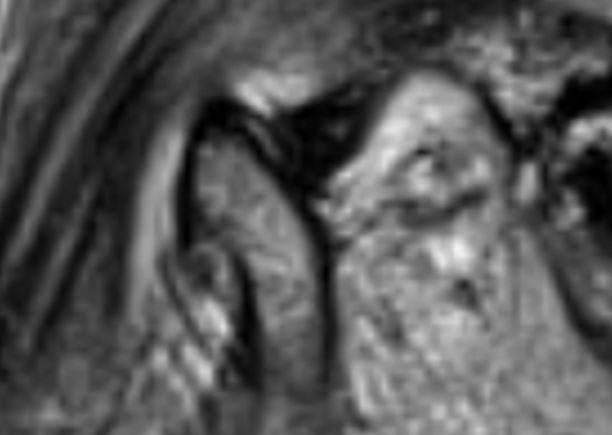
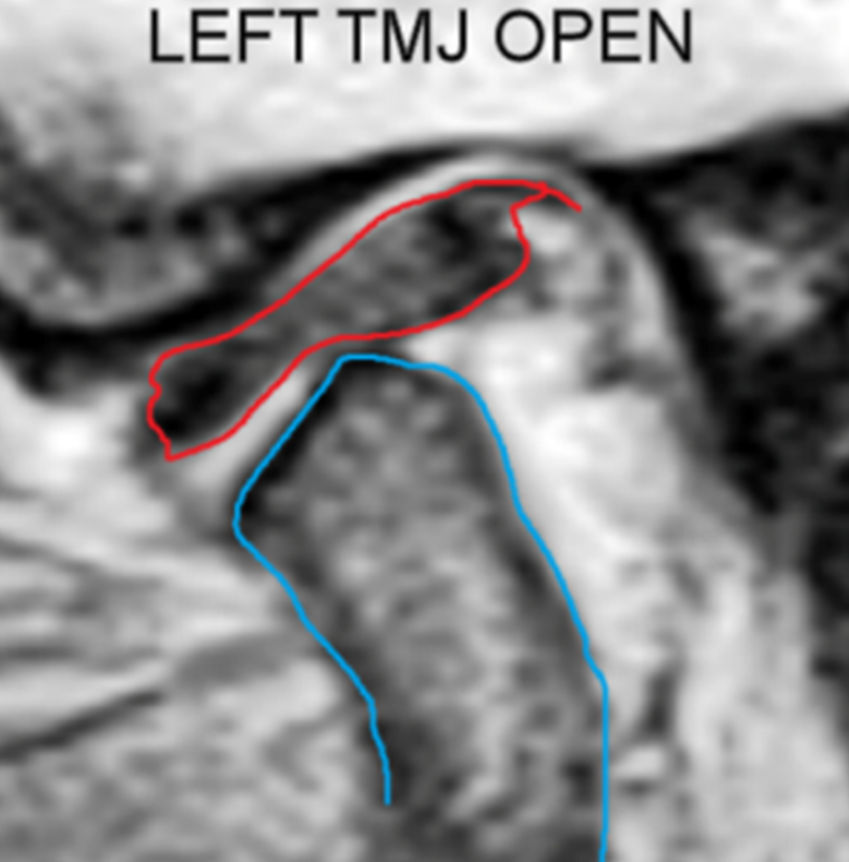
To confirm the diagnosis of a stuck disc in the left TMJ, proton-density MRIs were obtained with the patient in the maximum intercuspation position and with the mandible at the wide-open position. Disc appears partially displaced in the closed position, (Figure 9.) and it does not move with the condyle during a wide opening movement (Figure 10.)

Note that both condyles are very distalized in their closed positions. This suggests that a very substantial maxillo-mandibular mal-relationship may be present. Correction of such a condition may require repositioning of the bite.
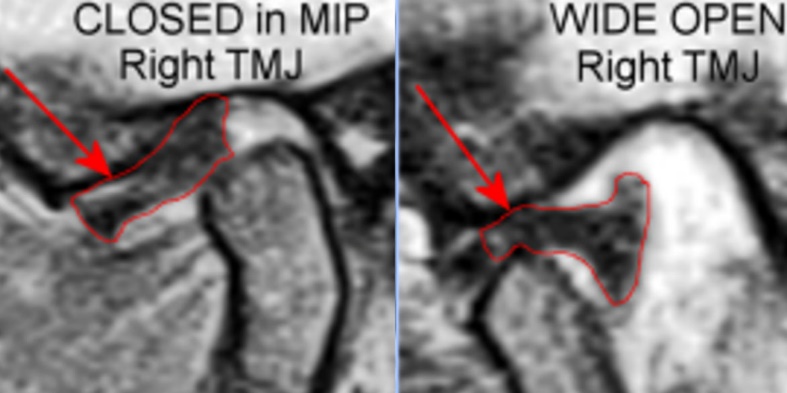
In contrast to the left TMJ disc and although also partially displaced in maximum intercuspation, the right TMJ disc moved with the condyle during opening. Note that the right TMJ was not making any large vibrations either. Figure 11.

In addition to the JVA and MRI documentation, the Range of Motion and velocity were recorded, as were the resting, clenching and swallowing EMG. Mastication capacity was qualitatively tested using the incisor-point tracking together with EMG.
Treatment Goals
a. Improve disc – condyle – fossa relationships
b. Reduce the intensity of TMJ vibrations
c. Decompress the retro-discal tissues
d. Balance the muscular components to relieve headaches
e. Avoid any progression of tympanic blood supply deficit
f. Reduce the level of tinnitus
Treatment Sequence
-
BioTENS was used to relax the musculature prior to taking a bite registration for twin night appliances. See Figure 12.
-
A twin (upper and lower) night appliance was initially delivered in early November to avoid overloading the lower anterior teeth as can happen with an anterior stop-bite single piece night appliance. The twin appliance creates an anterior-only contact point that maintains the posterior teeth out of contact. By the mere fact of opening the bite a few millimeters the condyles are translated forward to relieve pressure on the posterior attachment tissues. See Figures 9 through 13.
-
In late November a full coverage lower appliance with metal clasps that, fabricated from the previous BioTENS bite registration, was delivered. See Figure 14. The full coverage appliance includes occlusal morphology that allows the patient to function while wearing it.



After only two months of appliance wear the symptoms were substantially reduced, all the TMJ vibrations were minimized, the ROM had increased to 55 mm and the headaches were absent. The MRIs revealed improved disc condyle relationships in the maximum intercuspal position. Figures 15 & 16.


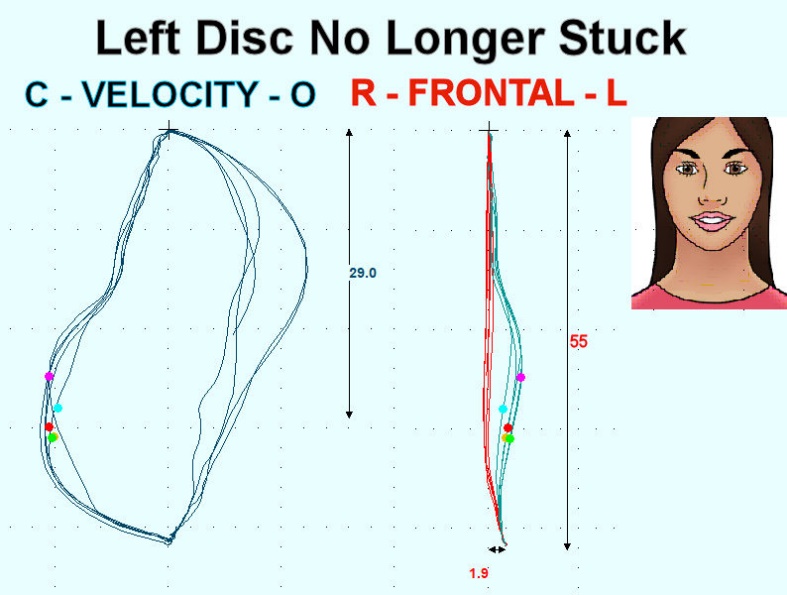
Based upon the post treatment MRIs it appears that the disc in the left TMJ was freed up from the eminence, was moving with the condyle and was re-captured. Figures 17 and 18.


The JVA record after 2 months of appliance treatment indicates smooth TMJ function bilaterally without any significant vibrations and an increase in the range of motion from 48 to 55 mm. Figures 19.

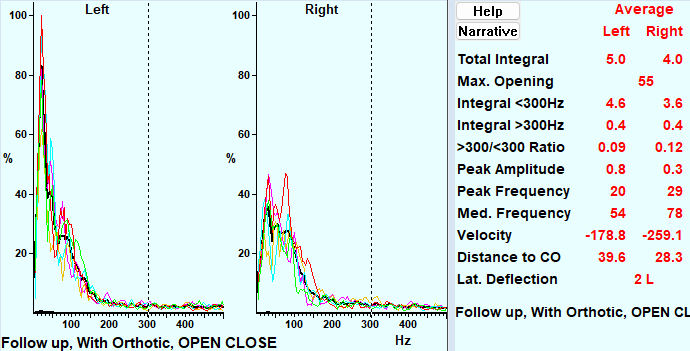
The Fast Fourier Transform into the frequency domain and the JVA Summary confirm the normalcy of the TMJ function bilaterally. Left and right Total Integrals that are less than 20 are routine observations in most asymptomatic control subjects. Figure 20.

The slight leftward deviation during closing visible in Figure 21 would be an indication of a slight resistance to translation, but that would be the right TMJ, not the left TMJ. (The cyan line in the frontal plane view is the closing path.)

Discussion
When the disk is stuck to the eminence in the intercuspal position the anterior border is negatively affected by the forward translation of the condyle, but the posterior border is not. That means freeing up the disk can allow recapture of a normal disc – condyle relationship as the posterior border should still be intact. Improved stability in a more forward intercuspal position in this case was also achieved using appliances. Of course, a permanent establishment of the altered maxillo-mandibular relationship can require an orthodontic or prosthodontic solution.
Historically, there has been a theory that the opening of the mouth begins with a purely sagittal rotation of both condyles for some distance before the condyle begins to translate. This concept is still embraced by some groups.15 However, more precise technology has demonstrated that the motion is a combination of rotation and translation starting from the intercuspal position.16
The conventional description of an internal derangement with a reducing displaced disc includes 1) a normal range of motion and 2) a more intense opening vibration and 3) a less intense or absent closing vibration.17 There may also be a deviation towards the affected side during opening and/or away from the affected side during closing. A portion of the vibration produced during reduction is usually transmitted to the non-affected side. The relative amount of transfer is dependent on the direction of the displacement because a disc reducing from a medial position causes more transfer than one reducing from an anterior displacement.18
The combination of a normal ROM and a larger closing vibration than opening vibration emanating from the TMJ indicates a stuck disc that is not moving from a normal closed position during wide opening.8 The disc may have an adhesion or just lack normal lubrication, but in either case, the condyle is required to pass in front of the disc to allow the mandible to open wide. In contrast to the situation where the disc is displaced anteriorly and reduces on opening, this condition includes the disc reduction on closing, which causes the closing vibration to be larger than the opening vibration.
There is one other joint condition that produces a larger intensity vibration during closure than during opening, which is the loose capsule. However, the waveform appears very different with much lower frequency content and less intensity (Total Integral). It is considered as a precursor to a full internal derangement that is due to minor stretching of discal ligaments. The looseness appears during closing because there is less tension between the disc and the condyle during closing than during opening, at least until the resistance of a bolus is met. With an empty mouth open-close, the tension between the disc and condyle during closing only increases when the intercuspal position is reached. Figure 22.

The reduced tension during closure allows a loose capsule in the left TMJ to wobble producing a low frequency, long duration waveform. See figure 23. In contrast, the higher tension on the disc from the condyle pushing it forward during opening is enough to suppress the wobble. Note that the waveform in Figure 23 is visibly less distinct than and less consistent than the one seen in Figure 6.

The FFT and JVA summary reveal that the loose capsule vibration contains both lower frequencies and lower intensities than other forms of displacing discs. Figure 24.

Limitations
Every case study is limited by the fact that every individual includes differences that make generalization difficult. The purpose of this case study was to suggest a novel approach to a situation that is likely to occur in clinical practice. While the stuck disc is not a very common finding with TMJ internal derangements, its presence has been well established within the dental literature.19
Conclusions
A TMJ disc that is stuck to the eminence in the intercuspal position without adhesion can sometimes be un-stuck using appliance therapy, which can be a non-invasive alternative to arthrocentesis with lavage. The JVA indication of a stuck disc is a consistent, short duration, larger intensity vibration during closing instead of during opening when the Range of Motion is also within normal limits. After the detection of a stuck disc by JVA the confirmation of it with a proton density MRI can be more easily cost-justified.
Potential Conflicts
J Radke is the chairman of the board of Bioresearch Associates, Inc.