
INTRODUCTION
The dental occlusion develops under the guidance of genetic and functional influences through the differing stages of dental arch development and adaptations to temporomandibular joint (TMJ) and masticatory muscles. It is understood that at the completion of the orthodontic treatment, there should be simultaneous contact of all teeth with good timing and equal intensity of masticatory force distribution around the arches.1
When dealing with complex malocclusions, orthodontists modify all dental contacts to achieve a new position of occlusal equilibration, take responsibility for its functional integration, and devote special attention to the quality and aesthetics of the outcome of their treated cases, irrespective of the therapeutic philosophy to which they adhere. Upon completion of their orthodontic treatment, the occlusal contacts of all teeth should demonstrate simultaneous contact timing and exhibit equalized forces, thus creating a uniform and symmetrical distribution of their masticatory forces.2
Angle described normal occlusion as an evenly placed row of teeth arranged in a graceful curve with harmony between the upper and lower arches. Besides good aesthetics, form and function, achieving a balanced occlusion is an important goal after restorative, prosthodontic or orthodontic treatment. Hence, occlusal balancing procedures are of significant importance after dental treatment and many methods are used in clinical practice to attempt to achieve this occlusal harmony.3
Clinicians use occlusal contact detection products to identify high restorations, when equilibrating occlusion, and to perform any post-orthodontic adjustments. However, these static indicators only mark the surface area of tooth contact, and demonstrate no ability to display the degree of occlusal force within the contact or quantify its time variance.3
Orthodontists have traditionally evaluated the quality of dental contacts by direct visual inspection supplemented by articulating paper marks. Most do not even routinely employ the time-consuming technique of mounting models on articulators, except for some complex cases or for the construction of customized positioner type retainers.4
Post-orthodontic occlusal changes may lead to occlusal force and timing discrepancies that can potentially be a contributing factor to the onset of temporomandibular disorders (TMD). Temporomandibular disorders are a collective term that describes a large number of clinical factors encompassing the entire stomatognathic system, namely the teeth, muscles and the temporomandibular joints (TMJ), but its etiology and the pathophysiology remains less than well defined. Occlusion is frequently cited as one of the major etiological factors precipitating TMD.2
The T-Scan III (Tekscan, Inc., S. Boston, MA USA) is an occlusal analysis system that records occlusal contact force distribution in real-time progressively from the first tooth contact until maximum intercuspal position (MIP) during closure.1 It provides quantifiable time and relative force measurements and displays accurately the occlusal contact sequence in closure and excursive movements, thereby improving the precision and treatment outcome of an occlusal adjustment procedure.2
Electromyography (EMG) is the most objective and reliable technique for evaluating muscles’ functions and their efficiency by detecting their electrical potentials. It makes it possible to assess the extent and duration of muscle activity. The main aim of surface electromyography is to detect signals from many muscle fibres.5
Disclusion time reduction (DTR) is an objective treatment protocol using T-Scan III (digital analysis of occlusion) and electromyography for treating occlusally activated orofacial pains. Chronic occluso-muscle disorder is a myogenous subset of temporomandibular disorder symptoms. These muscular symptoms are induced within the hyperactive masticatory muscles due to their excessively prolonged disclusion time, occlusal interferences, and occlusal surface friction that occur during mandi-mandibular excursive movements.6
Time recorded from the initial tooth contact into the maximum intercuspation is represented as occlusion time (OT) and should ideally be under 0.2 seconds; a longer OT indicates more interference and premature contacts during closure. Posterior Disclusion time (DT) was first described by Kerstein and Wright as the elapsed time required for all molar and premolar posterior teeth bilaterally, to separate from each other during a single excursive movement made in one direction (right, left, protrusive).2 Studies have shown that reducing the Disclusion time to less than 0.5 s per excursion with the Immediate Complete Anterior Guidance Development Coronoplasty (ICAGD), many chronic muscular TMD symptoms can be greatly reduced or eliminated.2
AIMS & OBJECTIVES
With these considerations in mind, the aim of this pilot study was to investigate the difference in occlusal force parameters in post-orthodontic subjects using T-Scan occlusal analysis data and BioEMG.
The objectives of this study were to evaluate:
-
The difference in the right and left lateral Disclusion Times in post orthodontic subjects, associated with pre and post DTR (Disclusion Time Reduction) using the T-Scan.
-
Difference in the muscular activities associated with pre and post DTR using BioEMG III.
MATERIALS
The following linked instruments were used:
-
T-Scan III® (Tekscan, Inc., S. Boston, MA, USA)
-
BioEMG III TM (BioResearch Associates, Inc. Milwaukee, WI USA)
Method of Collection of Data
The collection of T-Scan data provides objective insight into the differences in the excursive movement force and timing parameters between naturally developing occlusions and post-orthodontic occlusions, while verifying any association of TMD symptoms to frictional contacts and longer Disclusion time that previous studies have identified. Institutional research ethics committee approval was obtained for this study from the Rajarajeswari Dental College and Hospital Research Board. Five post-orthodontic treatment subjects were selected from dental students present in the Rajarajeswari Dental College and Hospital. Prior to an individual subject’s participation, the study protocol was explained to each subject, who had the opportunity to ask questions about the protocol, so as to accept or reject study participation. Informed consent was obtained from each subject prior to inclusion in the study.
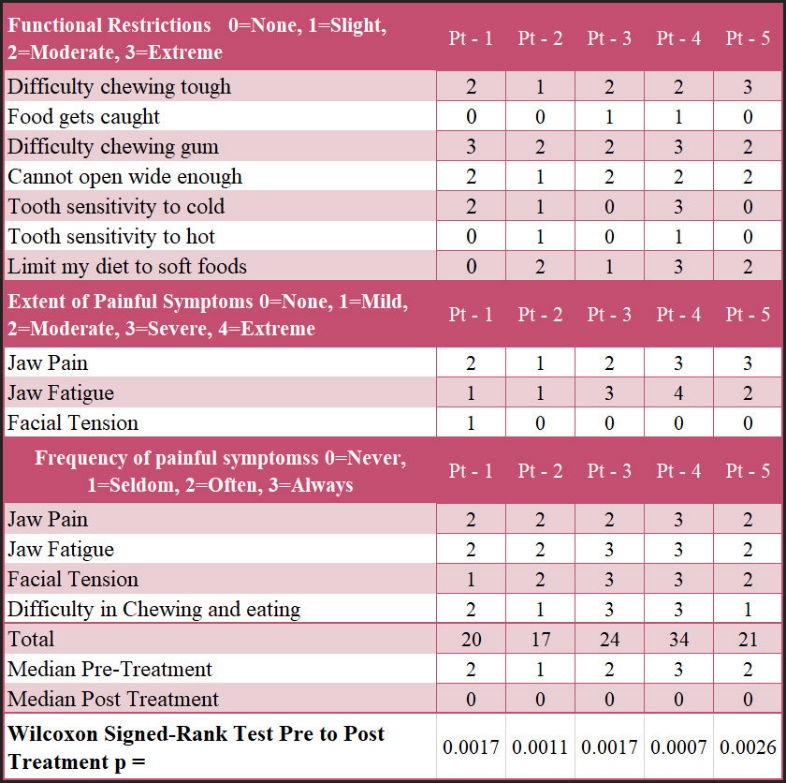
Inclusion criteria: Subjects presented were post orthodontic treated cases with no more than four missing teeth, excluding third molars, and with no edentulous spaces within the arches. Subjects with anterior or posterior crossbite, open bite, removable dentures, or more than four missing teeth (excluding the third molars), were excluded from the study. An intra-oral examination was performed on each subject to determine any missing teeth, whether crowns and/or bridges were present, and if third molars were present or absent. Following this examination, each subject filled out a TMD questionnaire documenting functional restrictions, painful symptoms and the frequency thereof such as; popping and clicking of the TMJ, restricted mouth opening, temporalis or masseter muscle tenderness on palpation, neck, shoulder, or facial pain, difficulty chewing, disrupted sleep patterns or sleep bruxism.
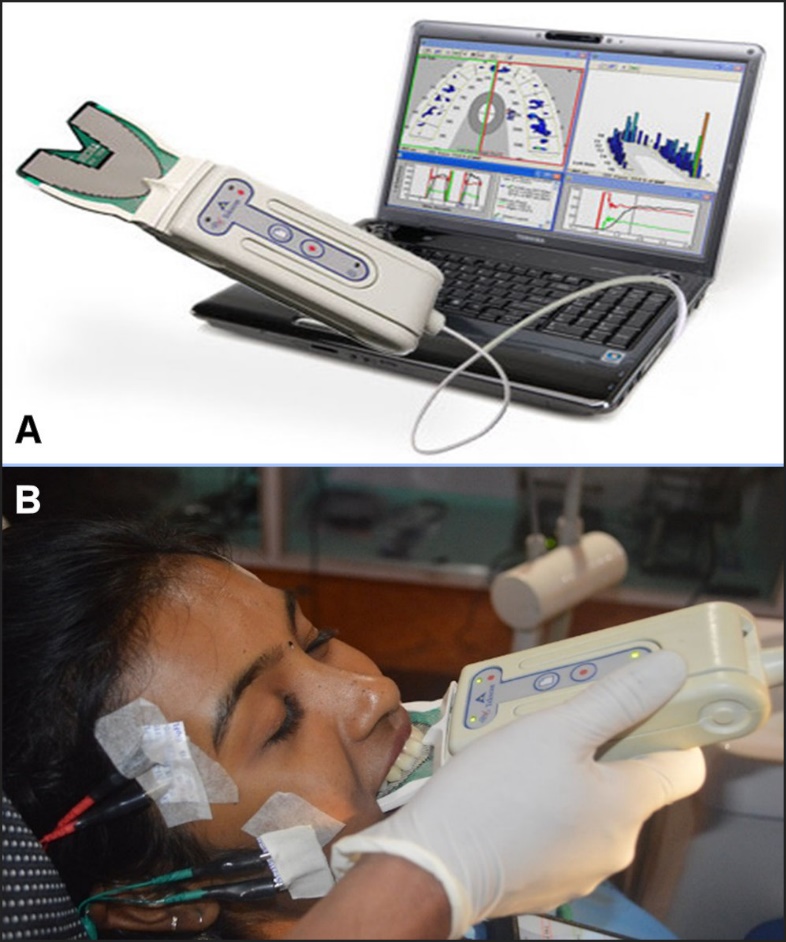
Multi-bite closure, and left and right excursive T-Scan recordings were obtained from each subject to measure the occlusal parameters to be analyzed during the study. All T-Scan recordings were made with the subject seated upright in the dental chair. For multi-bite recordings, each subject was instructed to occlude onto the recording sensor three times in succession using their maximum bite force. For the excursive recordings, the subject was instructed to occlude onto the sensor in their MIP, hold that position for 1–3 seconds, and then slide as far as possible to the left or right while maintaining tooth contact and open. This completed one excursive recording. Similar instructions were given for the opposite side’s working excursive recording. (Figure 1AB).
_the_t-scan_system_and_(b)_the_recording_of_relative_bite_forces_simultaneously_with.jpeg)
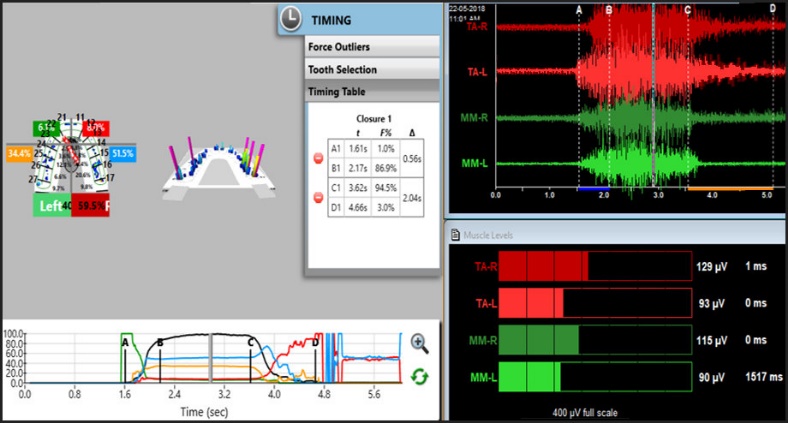
With the reliability of HD recording sensors, the occlusal timing and relative force analysis feature in the T-Scan software and computer hardware electronics, the clinician can see unparalleled occlusal force and timing information. Patients will be informed about their disclusion times if they are excessively long, causing excursive muscle hyperactivity detected in the EMG data (Figure 2).

After obtaining each patient’s consent Disclusion Time Reduction (ICAGD) was then performed to reduce occlusal interferences to function present and reduce prolonged Disclusion time. See Figure 3.
_disclusion_time_reduction_procedure.jpeg)
RESULTS
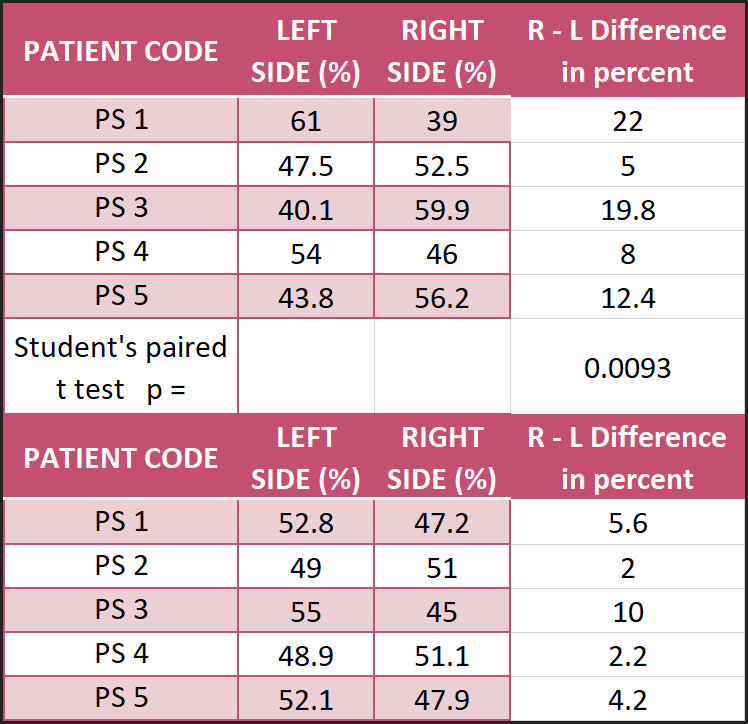
The occlusal force, timing data and EMG records were obtained by the following occlusal function recording types for five post orthodontically treated subjects. Multi-Bite data were recorded by three repeated patient self-closures onto the sensor to capture the first tooth contact closing into their static maximum intercuspation (MIP). These records also revealed the occlusal force balance between the right side and left sides, both pre and post ICAGD. See Figure 4
_and_post_(bottom)_with_the_percentage_differences_and_the_sig.jpg)
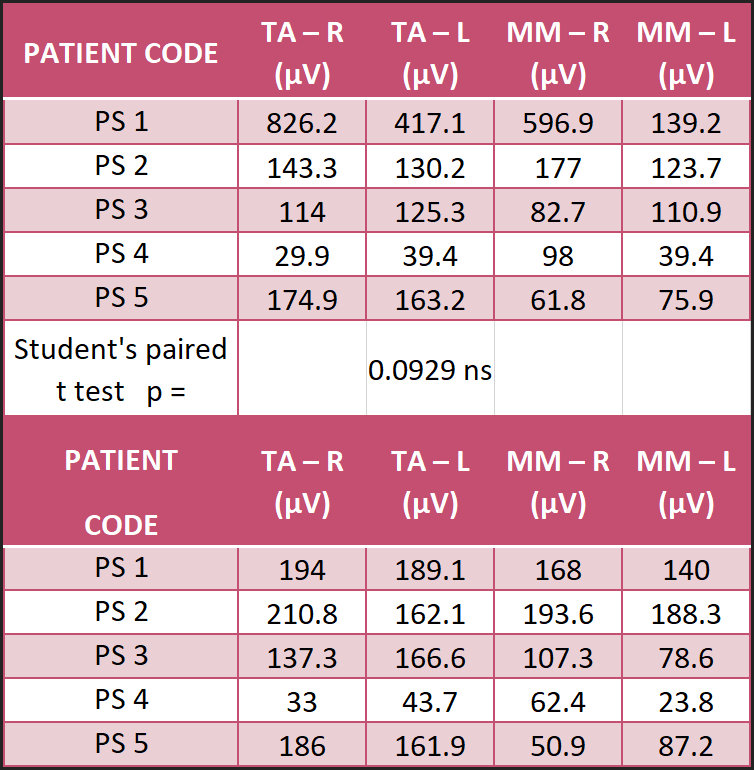
The Multi-Bite records, including the associated muscle activity (EMG) pre and post ICAGD, are listed in Figure 5. A trend was revealed towards lower EMG values, but the differences were not significant.
_and_post_(bottom)_icagd._although_a_.jpg)
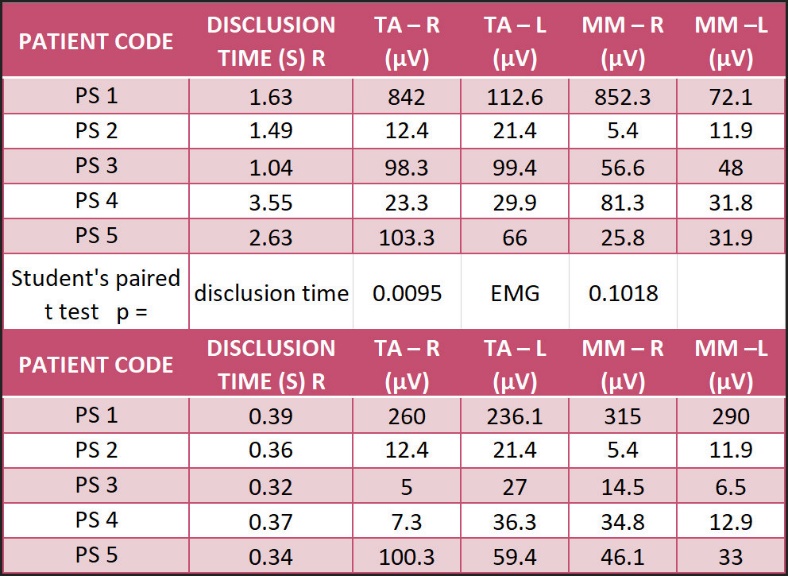
This assessment determined that the patients presented with prolonged disclusion times and friction excursing from MIP. The mean right lateral Disclusion time was 2.07 seconds. The values were outside of the known physiologic ranges of normal Disclusion Time (DT) < 0.5 s).1
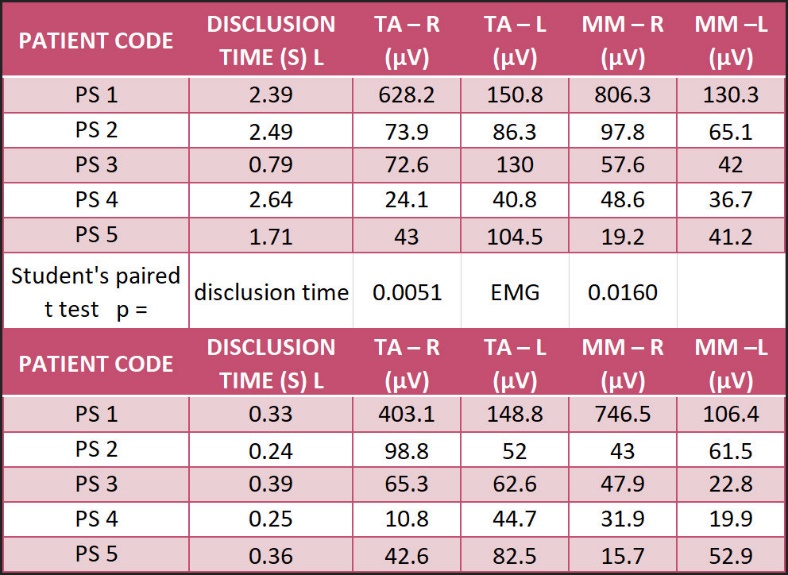
The mean pre-treatment left lateral Disclusion time was 2.0 seconds. All values were outside of the expected normal physiologic ranges of Disclusion Times. (Figures 6 & 7) The muscle activities are also shown in Figures 6 & 7.
_in_pre-treatme.jpeg)
_in_pre-treatmen.jpeg)
The reductions in the right and left disclusion times and their associated muscle activities are shown in Figures 6 & 7. The right mean post treatment disclusion time was 0.35 seconds and was significantly reduced from the pre-treatment mean time of 2.07 seconds (p = 0.0095). The left mean post treatment disclusion time was 0.31 seconds and was significantly reduced from the pre-treatment mean time of 2.00 seconds (p = 0.0051). A significant reduction was found in the reported symptom intensities for each of the five patients as shown in Figure 8.

DISCUSSION
The role of occlusal factors in the etiology of craniomandibular dysfunction has long been debated. Studies have documented the presence of heavy posterior force in post-orthodontic subjects and its association of TMD to occlusion. The results of this pilot investigation corroborate those prior studies and indicate that orthodontic treatment can increase the frictional contacts, prolong Disclusion time, and create more working side group function.2 The present study illustrates that; a.) the force finishing of post orthodontic treatment cases with occlusal equilibration utilizing T-Scan III and EMG III and b.) having “force quantified against time” data for precise treatment protocol constitute the best scientific method for dental medicine practice.1 A significant difference in the mean combined disclusion time was found between the pre and post right and left lateral DTR records. In the pre right and left lateral DTR times the Disclusion times were nearly six times those of the post right and left lateral DTR values. These values were outside of the known physiologic ranges (physiologic Occluding Time (OT) ≤ 0.2 second; Disclusion Time (DT) < 0.5 second).7–9
The post DTR right lateral mean disclusion time was 0.35 of a second and the left mean lateral disclusion time was 0.31 of a second. Such lengthy disclusion times have been shown in previous EMG studies to elevate excursive muscle activity levels. Reduction of the Disclusion time to < 0.5 seconds can reduce the muscle hyperactivity and related myofascial pain symptoms.10,11 The prolonged posterior tooth contacts of the occlusal surfaces of opposing maxillary and mandibular premolars and molars during lateral excursions results in prolonged forces on the periodontal ligaments of these posterior teeth. The prolonged forces stimulate the muscle fibers to contract for as long as the teeth remain in contact as long as the occlusal surfaces are engaged. Shortening of the disclusion time to < 0.5 seconds results in an occlusal scheme where the posterior teeth minimally contact each other during excursions and their respective periodontal ligaments are far less stimulated than during the pre-treatment condition. The shortened PDL stimulation time shortens the contraction time of the muscles of mastication.12 Permanent occlusal changes to reduce disclusion time appear to have reduced the muscle activity, although not significantly, for this pilot study. This suggests that one major etiologic factor for occluso-muscle disorder patients may be excessive posterior tooth contacts during lateral excursive movements that result in lengthy disclusion times.7 When the treatment protocol includes modification and management of occlusal forces, especially in cases such as prosthetic rehabilitation and various orthodontic treatments, T-Scan guided occlusal adjustment procedures should be considered as a finishing step to minimize occlusal imbalances, remove excursive friction, and shorten disclusion times. This technology aids the operator in obtaining an occlusion that is precisely finished to numerical endpoints that enhance the probability of healthy long-term results.2,3
CONCLUSIONS
Significant differences were found between the pre and post ICAGD treatment symptom levels in this pilot study. This was concurrent with right and left lateral disclusion times being reduced significantly and a trend towards lower muscle activities. Posterior occlusal surface frictional contacts and unbalanced occlusions following orthodontic treatment appeared to contribute to the symptomatology. Computerized occlusal analysis provides objective digital data for determining the status of the orthodontic result, as well as for observing the occlusal force distributions in occlusions that develop naturally, helping to improve the occlusal harmony of orthodontic treatment outcomes.
Conflict statement
The authors declare no conflict of interest within this unfunded study.