

BACKGROUND
Rather than establishing the etiology for the presence of CDH in the dentition, this common malady has been traditionally empirically treated without determining its causation.1–13 Citations in the prior sentence represent only some of the medicaments, approaches, and publications purporting to reduce or eliminate this type of common oral pain. None promote the discovery of etiologic conditions for this sharp and rapidly induced type of oral pain. Regarding CDH, Addy et al. appear to be the first authors to embrace the term of cervical dentin hypersensitivity in 1985 which was then followed by Pashley in 1993.10,14 A finding of CDH can result from: air, temperature variations (especially cold), osmotic change, tactile stimulation, electrical stimulation, or combinations of these stimuli.15 CDH is rapidly absolved once the stimulus is removed.
Let us now look at differences between CDH and dentin hypersensitivity (DH). The term of DH has been used for decades to describe both pulp pains, but they are each distinctly different. Slow, dull, and lingering DH pain arises under recently placed restorations or crowns. Of a clinical nature noted by the authors, it is self-limiting under liners or bases if deep dentin interfaces do not contain irritating materials to pulp tissues. Also, poor bonding exists with open dentin tubules present, as reported by other authors to create this type of tooth pain. DH is likely to result from a transient pulpitis produced by sympathetic activation to heal the pulp from bacterial insult, operative temperature elevations, and/or regional partial dentin tubule occlusion. A pulpitis is associated to pulp edema as a part of the healing process. Dental pulp increased pressure has been shown to be stimulated both independent of and dependent upon neuronal transmissions. Endothelium-derived vasoactive neuro-peptide Y has been shown as a stimulus for independent increased pulp pressure whereas sympathetic nerve fibers provide dependent vascular pressure elevations. Parasympathetic fibers do not exist in pulp tissues.16
Regarding neuronal mechanisms, there are four types of neurosensory transmission routes in the dental pulp: small non-myelinated c-fibers which are slow, more rapid myelinated A-delta fibers that connect to mechanoreceptors at the pulp-dentin interface, extremely rapid myelinated A-beta, and less speedy non-myelinated A-gamma fibers.15 A- gamma fibers regulate smooth muscle contractility. Separation of these neurosensory functions in the pulp and their influences on sensations of DH & CDH are still not completely defined in relation to either the Trigeminal Ganglion or Central connections for dental pain reactions. Neurogenic inflammation in the pulp and neurotransmitters from systemic sources via circulation can produce a pain perception quite dissimilar to traditional pain reactions reported as DH or CDH.
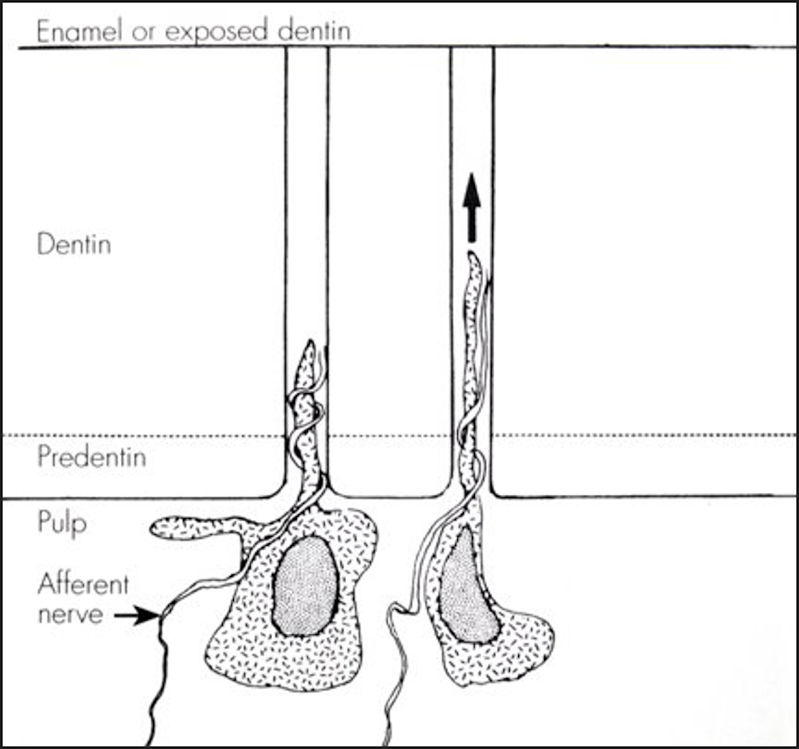
CDH (fast and rapid) has been theorized by Brännström’s “hydrodynamic theory” to rise as a result of dentin tubule fluid flow. The terms of DH and CDH were not clearly separated in that early 1960s time period.17 His primary research tool at that time was the scanning electron microscope. Brännström’s concept of hydraulic effects to odontoblasts and afferent nerves in the pulp from oral stimuli appears as Figure 1.

Terry indicated in 2011 that most authors and researchers accept the hydrodynamic theory with dentin fluid flow as a reasonable explanation for events of CDH.18
Subsequent development of a Frictional Dental Hypersensitivity (FDH) theory was proposed by Yiannios in 2014 to explain the biphasic presence of cold hypersensitivity to teeth. The FDH theory proposed that occlusal surface friction produced pain reactions due to his clinical interpretation of content found within research published by both Linsuwanont and Kubo.19–21 Recent reporting of molecular transducer influences by Chung from odontoblasts and adjacent pulp tissue in response to pulp temperature change give credence for CDH induction from his FDH theory.22 Chung also proffered that low-threshold mechano-receptors within and around the sensory organs that are the teeth are likely responsible for not only the transduction of proprioception, but may also help to mediate nociceptive inputs such as those related to DH or CDH. The robust concentration of A-beta myelinated fibers within the intra-pulpal and periodontal tissues are likely germane to the explanation as to why excessive (in force/time) posterior occlusal interferences relate to the presence of CDH. The authors also suspect that excessive autonomic sympathetic inputs resultant of excessive force/time interactions may also relate to pulpal edema22 and subsequent CDH symptoms. Therefore, a combination of mechanoreceptor, sympathetic and molecular transducer inputs are likely responsible for the nociceptive inputs relating to the perception of CDH resultant of occlusal origins.
A condition of occlusal disease (OD) was defined by Lytle in 1990 and advanced further in 2001.23,24 The term of OD was developed to explain conditions of chronic occlusal physiology or pathologies that arise during the contact(s) of teeth. Ruiz & Coleman later modified OD in 2008 to include CDH and TMJ effects from long-term occlusal contact, which can include function, parafunction, or from the deflective/aberrant intercuspation of teeth.25
Of note from a respected investigation by Gibbs et al. is that on average, teeth occlude for greater time and force during deglutition compared to during mastication.26 An exception to that scenario would be the presence of unavoidable occlusal interferences as indicated by repetitive triggering of EMG silent periods during every chewing cycle.27 Also, there are proposed exceptions to the Gibbs et al. findings or those of Kerstein in that the character of a food bolus for reducing particle size may be anticipated to impact timing and force values. More resistant foods require greater effort to reduce particle size than those that are not. Deglutition force and timing values are more of an average once particle size is sufficiently reduced to allow for this oral action of swallowing.
Additionally, while introducing the concept of adapted centric posture as a descriptor for a damaged but stable and adapted orthopedic temporomandibular joint, Dawson stated in 1995 that there is a direct correlation between the TMJ status and the occlusion. He suggested that dental medicine begin recognizing the correlation of deranged and imperfect temporomandibular joints as potentially a contributor to the clinical presentation of an altered occlusion.28 The current authors suggest that forms of occlusal disease, including CDH, seldom occur in a single category of this physiology or pathology.
Coleman developed a protocol in 1979 using an attenuated air stream to detect and quantify CDH.29 See Figure 2. It was defined as an “air indexing method” using a minor puff of air for ½ to one second beginning on the most distal tooth in a quadrant. Then, rapidly progressing anterior directed to cemento-enamel junction (CEJ) regions at a 45° angle to the long axis of respective teeth with room temperature air at a distance approximating 5 mm. See Figure 2. Both vestibular and lingual regions were evaluated in this same manner to gain a “threshold patient response” to an air stimulus while minimizing desiccation from air. If a tooth was found with a “positive air index”, then all air indexed teeth were exposed to the same air pressure.29 A “diagnosis” of CDH was not rendered until a second appointment verified an initial “detection” to rule out conditions of “incidental tooth trauma” or a recent occasion of exogenous/endogenous biocorrosion.30,31 The definition of biocorrosion includes chemical, biochemical, electrochemical, and/or protease action upon teeth, but was not included in the purpose of this article.

During the '80s a device known as a Fluid Control Block (FCB), see Figure 3, was developed and then patented by Coleman to share air indexing information with distant office personnel and remote clinicians.29 It was never brought to the dental marketplace, but attenuated volumes of air used in the determination of CDH were now standardized for clinicians.
_with_5_choices_of_air_volumes._reprinted_by_.jpg)
Yiannios developed a “cold water swish” protocol following an empirical clinical observation that patients frequently reported cold hypersensitivity of their dentitions resultant of the air water ports of a hi-speed handpiece cooling the surfaces of the teeth targeted for computer-directed occlusal treatment procedures.19 This hypersensitivity would consistently abate by the end of Disclusion Time Reduction (DTR) ICAGD computer-directed occlusal treatment.32 He implemented the protocol of using a cold water swish for 5 seconds both prior to and after the ICAGD occlusal therapy for Occluso-Muscular Disorder (OMD) patients. He also used this protocol for patients returning following operative filling or crown procedures with confounding hypersensitivities to determine a means of tracking patient responses. This protocol involves recording the patient’s cold hypersensitivity response using a combined numerical/visual analog scale (0-10) both before and after digitized and objectively measured occlusal therapy.
The cold-water swish used by Yiannios involved using a cupful of ice cubes which was submerged in water. After a minimum of 3 minutes, the ice-cooled water was then used by the patient to swish throughout the mouth to determine the /visual analog/numerical scale pain response. The cold water was measured repeatedly by Yiannios to report a consistent temperature of 35° F.
Comparison Between Cold-water and Air Indexing Stimulations Among Yiannios’ TMD Patients
After publishing the novel FDH theory based upon the cold-water swish stimulus for CDH, the authors felt that it would be of value to test the patient response to an attenuated air stimulus as well as the cold-water swish. The cold-water swish and air indexing protocols were used to generate data on thirty symptomatic and consenting TMD patients over several months to determine if the ICAGD occlusal therapy protocols would decrease CDH cold water and/or air episodes.
Both air and cold have been supported in the literature as stimuli for CDH.10,14,18,29 The current authors proffer that conditions of OD which can include CDH frequently evolve from more than just occlusal imbalances to include internal TMJ circumstances as well. An investigation was undertaken with these concepts in mind.
METHODS & MATERIALS
A population of 30 subjects was evaluated by the cold-water swish (Yiannios) and air-indexing with a “Fluid Control Block” (Coleman) as presented in the background section of this article and the FCB as shown in Figure 3. Of a clinical and etiological basis, the least amount in the volumes of air which produced a hypersensitivity response was then used in the detection and qualification of air responses for all teeth termed as a threshold patient response. These patients had all sought diagnosis and potential treatment from Yiannios due to symptoms of CDH as well as other traditional OMD maladies relating to headaches, tension in the muscles of mastication, and/or suspected TMJ pathologies.
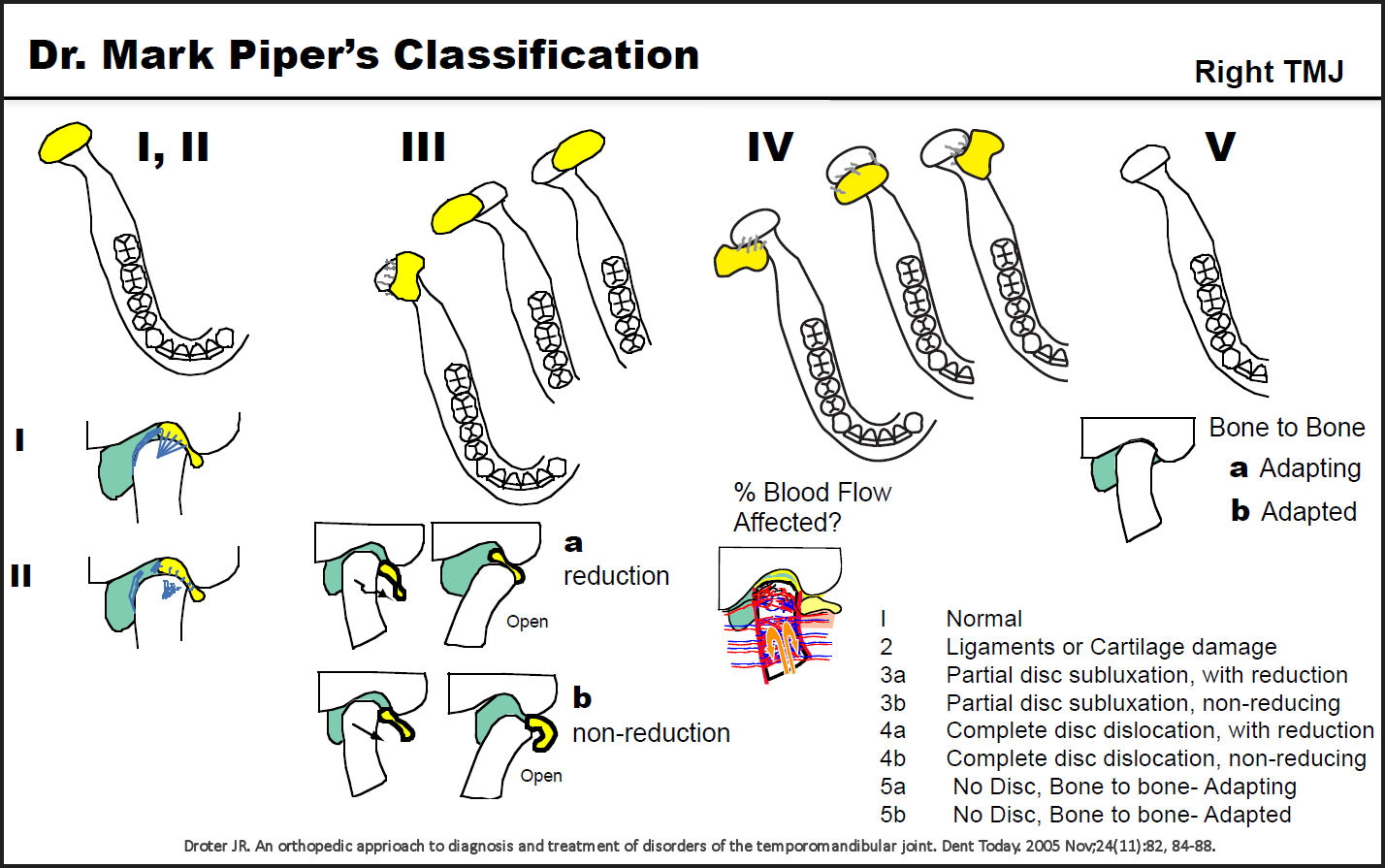
Each subject underwent a thorough medical and dental history analysis to rule out systemic disease, biocorrosion, or dental conditions that could have contributed to their orofacial pain symptoms. All patients underwent CBCT and Magnetic Resonance Imaging (MRI) screening to determine their Piper Classification of TMJ health bi-laterally since the condition of the hard and soft tissue components can readily influence the occlusion. The condition, position, and degree of herniation or lack thereof of the articular meniscus (disc) is extremely important in vetting occlusal stability for a patient as disclosed by Shellhas and associates as well as Wang et al.33–35 The Piper Classification system is based upon joint & disc location and health determined by MRI and CBCT with its clinical meaning shown in Figure 4. An MRI objectively and reproducibly discloses soft tissue abnormalities whereas a CBCT performs the same for hard tissues. Adapted and non-adapted joints for the 60 TMJs (30 patients) in this investigation are shown in Table 1. This Table also shows additional characteristics for the study population.

Patients’ bilateral TMJs were all screened with Joint Vibration Analysis (BioJVA - BioResearch Associates, Inc. Milwaukee, WI USA) and then imaged using CBCT and MRI prior to Yiannios’ implementation of occlusal therapy. Range-of-motion (ROM) maximums were obtained and observations of aberrant mandibular movements recorded. Palpation for muscles of mastication (MOM) sensitivity levels also took place in the screening protocol.
Note that in determining the status of adapted vs. non-adapted TMJs, Yiannios considered Piper 1, 2, 3a, 4a and 5b joints as relatively stable and adapted. Piper 3b, 4b, and 5a joints were deemed as unstable and maladapted according to the Piper classification system. It should also be noted that if either of a given patients’ two TMJs were found to be unstable, then the patient was considered not an ideal candidate for occlusal therapy.
Inclusion criteria within this investigation were those individuals lacking a history of recent macro-trauma, patients willing to complete all pre-op evaluations, and those not in need of expanded systemic medical or dental workups.
Excluded in the investigation were patients without CDH, lack of adequate diagnostic criteria, patients who presented with anterior open bites, and those who for any reason could not continue pre- and post-op data collection.
All included patients underwent T-Scan III/T-Scan 9 (Tekscan, Inc. South Boston, MA, USA) evaluations to determine force and timing values both during closure into Maximal Intercuspation Position (MIP) as well as through left and right excursive movements. Occlusion Times (OT) and Disclusion Times (DT) respectively were obtained for all individuals in the study, both in the static OT closure and measured excursive contacts of teeth (DT) during mandibular movements.
OT represents the time from the first contact until total tooth intercuspation is achieved. A healthy OT has been shown to be less than or equal to 0.2 seconds. DT force and timing values are registered with the T-Scan system from the full closure in a MIP position until complete disclusion of posterior teeth is achieved over time upon canines, laterals, and/or central incisors (measured anterior guidance). A healthy DT has been shown to be less than or equal to 0.5 seconds according to Kerstein and other authors.27,32,36,37
In addition, electromyography (Bio/EMG III - BioResearch Associates, Inc. Milwaukee, WI USA) synchronization was used with the T-Scan III data to disclose muscular contractility during both MIP and excursive contacts of opposing teeth in both the initiation of the static OT and the dynamic DT timed occlusal events. The Bio/EMG III system has in recent years been developed to record muscular contractility synchronized with T-Scan III screen frames and is known as the T-Scan/EMG Link.
Appliance therapy was not begun or prior appliances worn at any time point during this investigation.
Included occluso-muscular patients found with positive CDH were then treated by subtractive or additive occlusal therapy according to the ICAGD protocols from the maximum intercuspation position as promoted by Kerstein and Yiannios19,32 and earlier subtractive methodology for occlusal therapy by Schuyler.38 The subjective Numerical Scale (NS) reporting of cold-water swish values (0- 10) were compared pre- and post-op ICAGD occlusal therapy for each patient.
Subjective threshold patient responses were recorded with an attenuated air stimulus severity range from 0 (no sensitivity) to 3 (severe) since each individual served as his or her own control. These minimal detection rankings were totaled for each patient and then divided by the number of teeth present before and after ICAGD on the same day as cold-water swish values were obtained. These post-op measurements always occurred the same day and within hours of the completion of occlusal therapy.
Care was taken to separate times in the evaluation of the two different CDH stimuli in a fashion to quiesce remaining hypersensitivity levels during post-op data acquisition. To be clear, a constant minimum of fifteen minutes was used as the separation time between cold water swish and air index testing. A Wilcoxon Signed-Rank test (difference pre- to post-DTR treatment) was used to determine probabilities that occlusal therapy influenced the reduction of CDH.
All 30 patients underwent ICAGD treatment in the effort to reduce the Disclusion Times obtained by digital occlusal analysis (T-Scan). It slaved in 3/1000 second increments to the Bio-EMG III to objectively study the influence that the altered DT’s had upon the bilateral superficial masseter and anterior temporalis muscles. The synchronized EMG data assisted the clinician in determining when to cease occlusal corrections, as shown in previous publications as published by Kerstein and Yiannios.19,32
All 30 subjects were evaluated pre-operatively with JVA, EMG, CBCT, T-Scan, and MRI to objectively and reproducibly establish current masticatory system conditions. Air indexing and cold water swish pre- and post-op occlusal therapy values were obtained and recorded.
RESULTS
Table 2 shows T-Scan pre- and post- op cold water swish & air index values for ICAGD occlusal therapy in this treatment group. Correlation coefficients between cold and air stimuli for CDH changes as a result of digitally guided occlusal therapy are shown in this Table. Probabilities of correlations in the analysis by the Wilcoxon Signed- Rank test are similar pre- and post- ICAGD therapy as disclosed by Table 2.
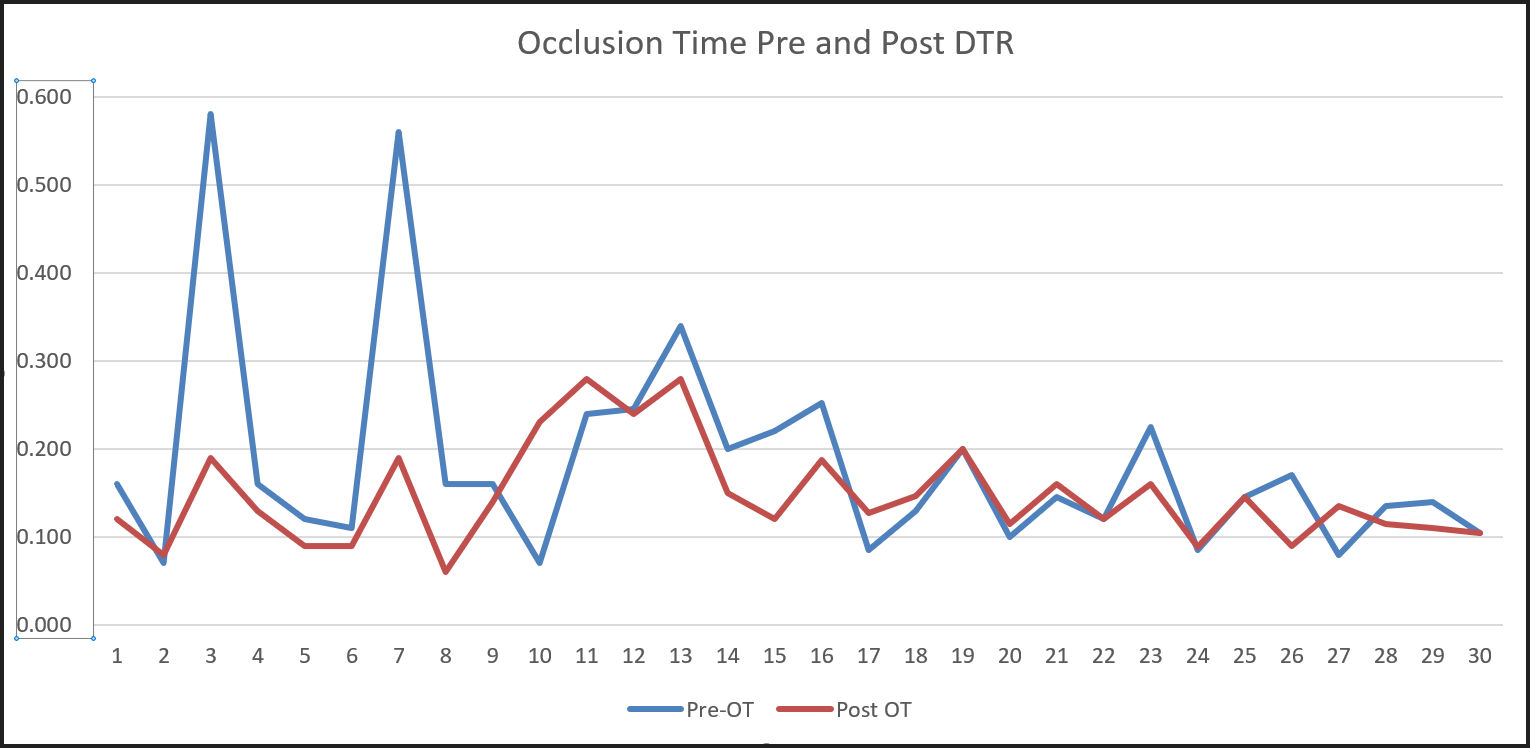
OT force and timing values relate to sagittal plane contacts of teeth. On most occasions, when DT was reduced to promoted levels by ICAGD to accomplish Disclusion Time Reduction (DTR), then OT recordings also fell to within normal limits (WNL). Figure 5 discloses pre- and post-op OT reduction times following DTR treatment. FO recordings not reported by a Figure in this Results section relate to timing values during the initial contacts of teeth.
_as_a_result_of_icagd_as_recorded_by_t-scan_sof.jpg)
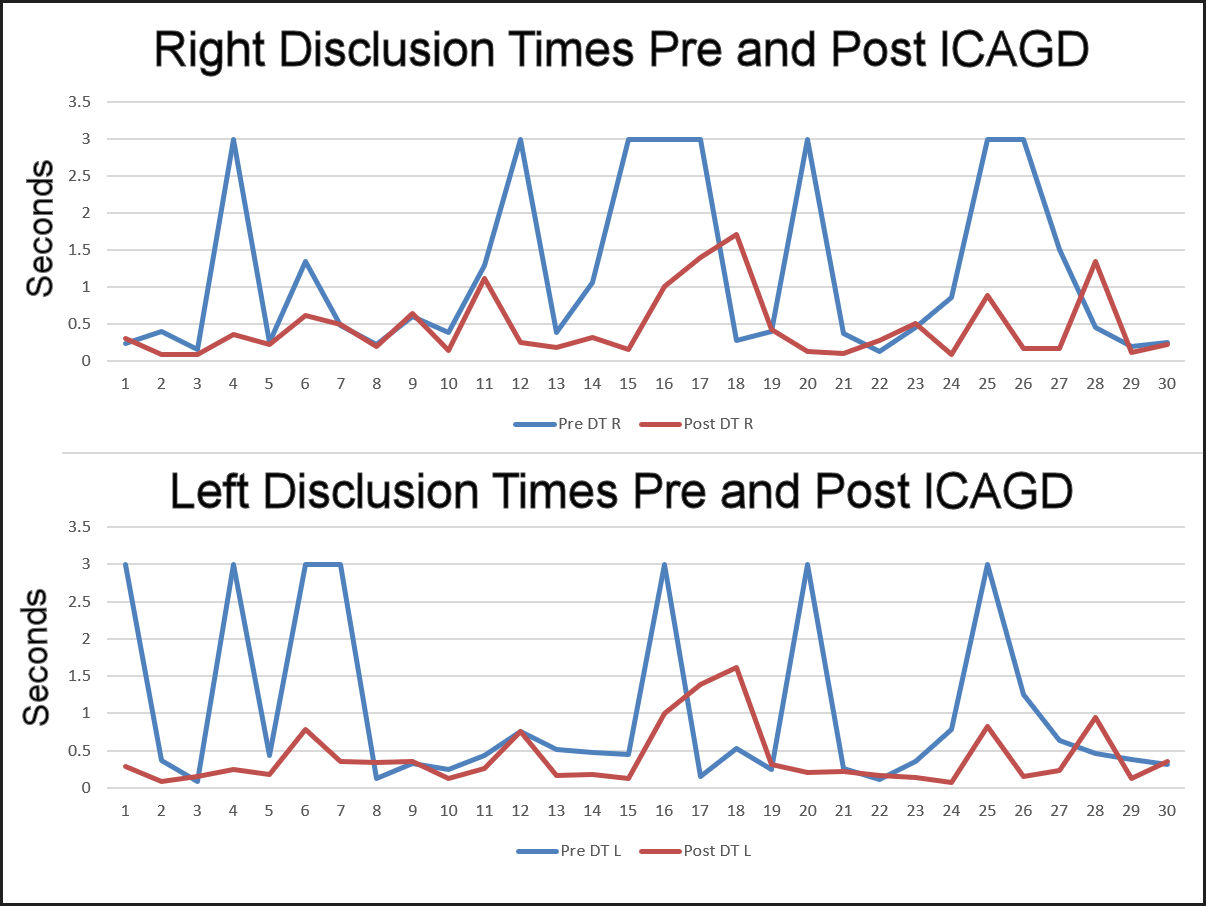
Figure 6 shows graphically the pre- and post- ICAGD disclusion times for right and left lateral excursions.
_following_icagd_for_respective_individuals_sho.jpg)
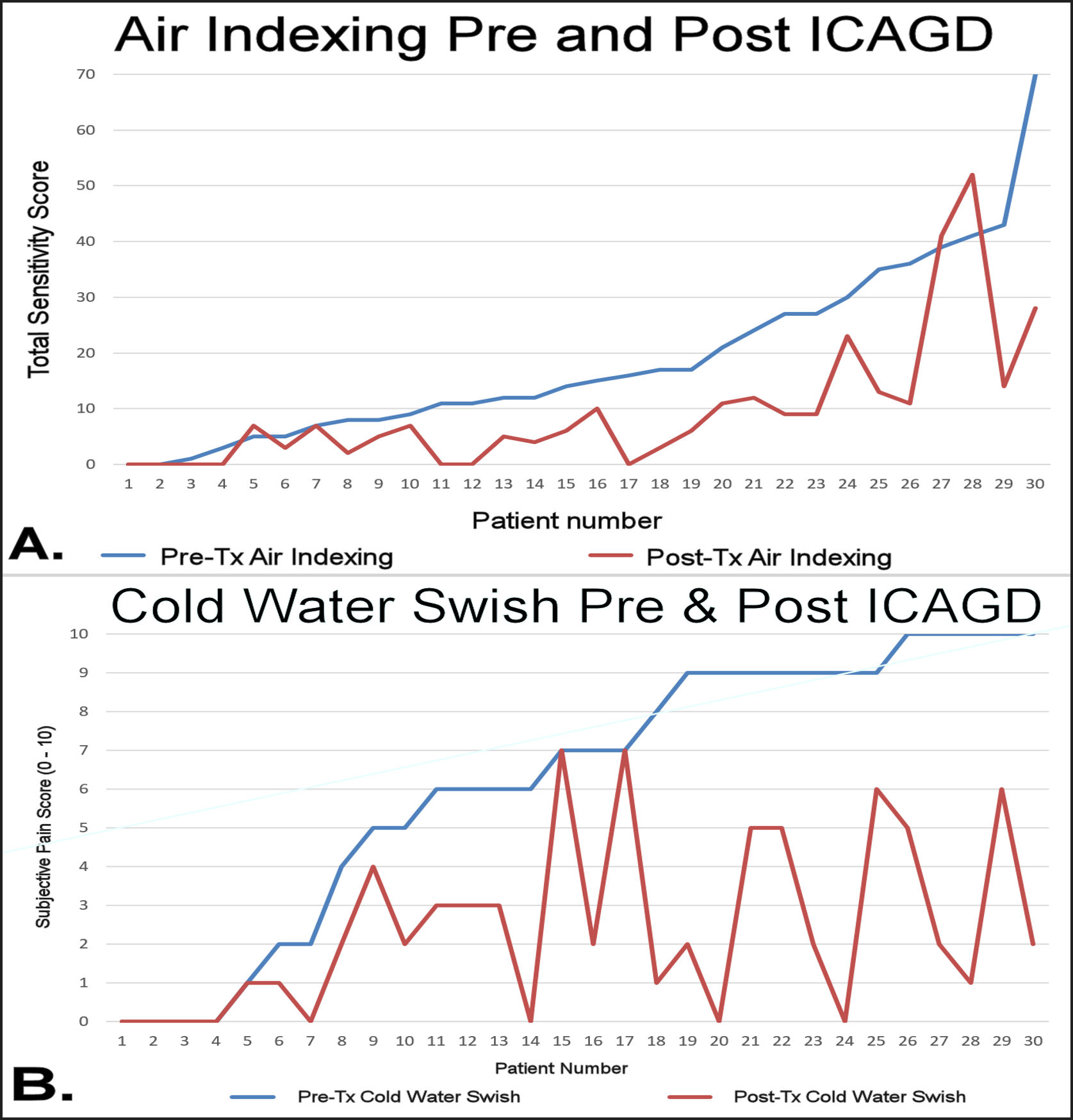
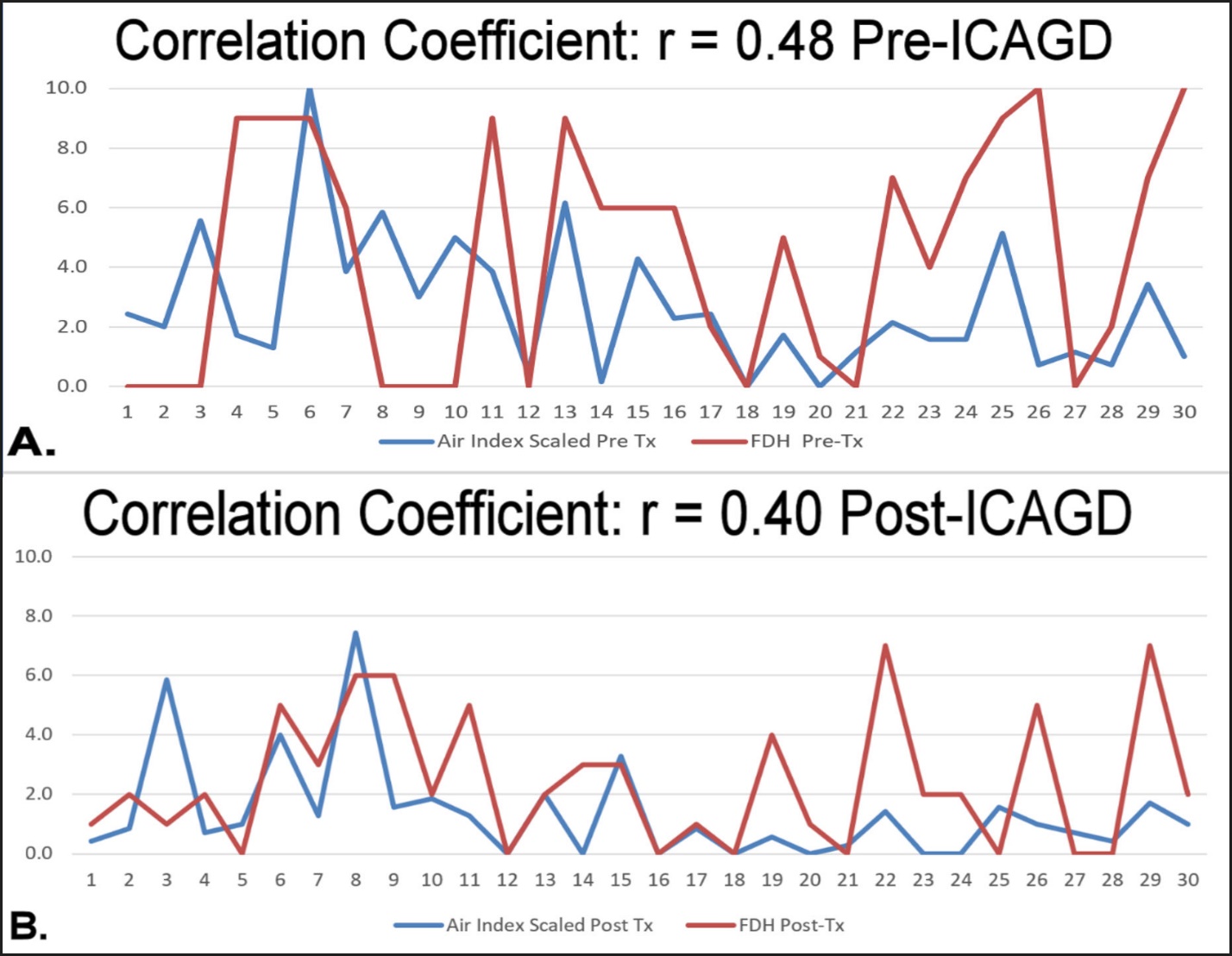
Line graphing for pre- and post- ICAGD sensitivity levels of CDH are shown in Figure 7A for air indexing and Figure 7B discloses values for cold water swish as found on the same patient treatment day. Figures 8A and 8B illustrate air indexing and cold-water swish line graph correlation coefficients pre- and post- ICAGD treatment for these CDH stimuli with reporting that both are related & improved by measured occlusal therapy.
_and_cold-water_swish_(b)_pre-_and_post-icagd_respectively_for_all_30_m.jpg)
_and_post.jpeg)
Nine patients of the 30-subject patient pool were treated, at least in part, by additive occlusal therapy on canines using composite bonding or ceramics to shorten DT recordings. In general, ICAGD occlusal treatment by DTR (anterior guidance) produced OT levels to WNL outcomes of less than 0.2 seconds, rarely requiring necessitating occlusal changes to accomplish this OT reduction separately.
Within the patient pool, the five relatively unstable and maladapted Piper Class 4b TMJs were reluctantly treated by Yiannios with occlusal therapy due to informed patient’s election to do so. Surprisingly, these individuals also found reductions in air indexing and cold-water swish values post-op.
DISCUSSION
Most of the prior literature does not address the differences between DH and CDH, but each is distinctly different. These types of dental pain are likely modulated to local and/or central neurosensory systems by different mechanisms or pathways. DH seems for the most part to be related to pulp edema, whereas CDH to the presence of internal neuropeptide controlling factors and/or open dentin tubules.
The various conditions of occlusal disease are not all related to CDH. In the same sense, both endogenous and exogenous biocorrosion play a role for creating CDH due to an increased number or size of open dentin tubules in the application of the hydrodynamic theory. The FDH theory can apply whenever rapid temperature variations occur in the pulp from frictional engagements. An FDH response of CDH may or may not be related to patent dentin tubules. Hence, a combined application of both theories seemed prudent for reporting changes of CDH.
Chronic occlusal microtrauma was investigated by measured means for timing and force values in the disclosed study. ICAGD occlusal therapy was found to reduce both attenuated air and cold-water stimuli for CDH.
The five relatively unstable Piper Class 4b TMD patients treated by ICAGD means were also found with CDH reductions. A conclusion could then be proposed that not all CDH positive teeth have an etiology of TMJ pathology. However, the elimination of CDH by occlusal therapy means has no basis for a reduction of internal TMJ pathology.
Further investigations are indicated to support or refute results of this investigation using objective and digitally measured means. The effects of chronic microtrauma which ultimately produce OD needs further study. The investigation described in this publication found moderate correlations between cold water swish and air indexing stimuli for CDH prior to the removal of occlusal etiologic factors. A bottom-line finding was that both cold and air sensitivity reductions were accomplished by the reduction of DT force and timing values.
Though long-term follow-up was not accomplished in this 30-patient study, it would have been interesting to track both the air indexing threshold patient response and cold water swish numerical scale recordings over an extended time period. Over the years in regards to the FDH cold water swish reduction following ICAGD occlusal adjustment therapy, Yiannios has found that as long as the patients’ TMJ orthopedic condition does not worsen nor does the patient undergo unmeasured iatrogenic restorative and/or orthodontic changes which can produce altered opposing dental interactions in space and time, then the patients’ decreased pain response to the cold water swish over passing time typically remains lasting and stable.
The effects from frictional abrasion compared to occlusal imbalances or biocorrosion upon CDH have been reported as minor contributing etiologic factors for its presence.31
The FDH theory proposed by Yiannios needs closer scrutiny to determine what role excitatory influences of molecular transducers, the TMJ health condition, and excessive excursive occlusal engagements play in the genesis of CDH.
LIMITATIONS
Macro-traumatic events which produce either temporary or permanent TMJ pathology were not evaluated or reported in this investigation. However, the use of MRI for soft tissue and CBCT for hard tissue imaging with the assignment of the Piper classification determinations assisted to clinically separate individuals not deemed appropriate in this investigation of CDH treatment by occlusal therapy. Not all patients with CDH are appropriate candidates for measured occlusal treatment. Occluso-muscular disorders (TMDs) which produce muscular tension by MOM and/or joint pain in accommodating TMJs can result from either macro-trauma or chronic micro-trauma.
EMG data for muscular contractility was not reported during this investigation, but Dr. Yiannios as the investigator, reports that ICAGD therapy reduced contractile muscle actions. An experienced clinician must determine what measured methods seem most appropriate prior to initiating occlusal therapy following a diagnosis of CDH for a patient.
CONCLUSIONS
The null hypothesis that cold water swish and air indexing stimuli for CDH are not related was rejected. Further, ICAGD occlusal therapy did reduce sensitivity values to both cold and air. The use of digital occlusal analysis with the objective and reproducible T-Scan technology was found to be of significant benefit for reducing these CDH conditions post- ICAGD. Future investigations are indicated to support or refute that cold-water swish and air indexing dental hypersensitivity is significantly reduced by digitally measured anterior guidance development. Both additive and subtractive occlusal means need additional study in the reduction of CDH for appropriate clinical situations.
The FDH theory was introduced as a novel approach to explain how measurable excursive occlusal aberrations can readily result in the development of CDH. Additional study is needed to determine how and when both the hydrodynamic and the FDH theories apply in the dental pain condition of CDH, particularly since the etiologic condition of occlusal imbalances are not routinely measured within the oral cavity.
Funding
No funding was provided for this study.
Potential Conflicts
No Conflicts were reported.