INTRODUCTION
The Diagnosis and treatment of Temporo-mandibular Disorders is often a challenge due to patients presenting with varying symptoms. Consequently, many different therapies, some conservative and reversible, others irreversible, have been advocated for patients with Temporomandibular Disorders. A number of successful treatment outcomes have been reported, with occlusal splints, physiotherapy, muscle-relaxing appliances, and pharmacological interventions.1
Many dentists advocate that Occlusion is the structural foundation within the Stomatognathic system and is of integral significance in the multifactorial concept of the Temporomandibular Disorder (TMD) etiopathogenesis. When the occlusion is pathogenic and playing a role in the appearance of chronic symptoms, occlusal splint therapy is a considered a viable option due to its reversibility, and the reported beneficial effects a splint may have on the Craniomandibular complex.2
Bledsoe defines a splint as a removable oral device fitted between the maxillary and the mandibular teeth that stabilizes and unloads Temporomandibular Joint, reduces the muscle activity of the Craniomandibular complex, provides for occlusal disengagement, restores the vertical dimension of occlusion (VDO) when overclosed, and reduces the attrition of the teeth from traumatic parafunctional occlusal forces.2,3 Many recommended treatment protocols that include the use of splints, to not only to relieve symptoms, but also to establish (in theory) an “ideal” or “correct” jaw relationship.
The efficacy of conservative occlusal therapy through splints remains a controversial topic. A number of relevant studies have highlighted the therapeutic efficacy of these occlusal appliances,4–8 while different authors have reported contradictory results.9,10 and others have denied the usefulness of splints in resolving Craniomandibular disorder symptoms.11
A few clinical studies have demonstrated that Occlusal Stabilization Splint therapy can provide clinical relief from myofascial pain.12,13 When properly adjusted with stable occlusal tooth contacts throughout the dental arch, the Stabilization Splint is a good method of obtaining Centric Relation occlusion, while eliminating posterior interferences, and providing anterior guidance on anterior teeth, all of which helps reduce neuromuscular activity.1,12 A splint reduces neuromuscular activity by providing a barrier effect between opposing teeth, which bocks (to a degree), the neurologic response that teeth emit when opposing teeth compress each other within the Periodontal Ligament fibers, or when nerve endings within the pulp respond to when opposing teeth load and flex.14
All disciplines of dentistry (including adjustment of occlusal splints) require that the clinicians assess the articulation of the teeth/prosthesis with respect to simultaneous contacts, bite force and timing. However, assessing dental occlusal forces often requires complex, yet inaccurate interpretations frequently based on subjective, non-quantifiable occlusal indicators (articulation paper, shim-stock foils, or impression waxes, used with patient “feel” feedback).15–17 These methods lack objective accuracy and measurement during occlusal adjustment procedures, which can lead to poor outcomes with respect to occlusal force imbalance and non-uniform distribution.17–20
Studies show articulating paper marks cannot measure occlusal loads, and that no scientific correlation exists between the depth of a mark’s ink color, or the mark’s surface area (size), with the amount of applied force. Nor do articulating paper marks illustrate the contact timing sequence that results from transitory occlusal contacts that precede complete intercuspation.15–17 Alternatively, multiple studies repeatedly show the T-Scan Computerized Occlusal Analysis System (Tekscan, Inc., S. Boston, MA, USA) demonstrated the ability to record in real-time, quantifiable occlusal contact force and time variances from the initial tooth contact into Maximum Intercuspation (MIP), that provide objective insight into the degree of right side-to-left side occlusal force imbalance.17,18,21
OBJECTIVE
This pilot study evaluated if a maxillary full arch Stabilization Splint was successfully measurably bilaterally balanced using articulation paper with an operator’s best judgment. After the conventional adjustments were completed, T-Scan data (T-Scan Version 9.2, Tekscan Inc., S. Boston, MA, USA) further guided the occlusal adjustments to the splints, to achieve an improvement in the measured bilateral occlusal force balance.
MATERIAL & METHOD
Eleven Thai patients ages 21 - 45 years, (mean age = 30 years), who had been wearing a hard-acrylic maxillary full arch Stabilization Appliance for a minimum period of six months while under the care one clinician for Temporomandibular Disorders, at Thammasat University Faculty of Dentistry clinic, were selected from the Thammasat University patient database who were undergoing splint therapy for TMD symptoms (including bruxism, occlusal discrepancies, sleep disorders, tenderness in or around the masticatory muscles). Stabilization Appliances were fabricated to treat the specific signs and symptoms of occlusal dysfunction that the patients presented with, by customizing the occlusal force components therapeutically, without altering natural teeth, or changing existing restorations. All of the splints were made in Centric Relation, and adjustments were done in CR for majority of patients, but for some of patients, the CO (MIP) position was selected depending on the individual patient requirements. The goals were to alter the maxillo-mandibular relationship and disengage the occluding natural teeth.
The Inclusion criteria were that subjects had used a hard-acrylic maxillary full arch Stabilization Appliance for a minimum of six months and presented with no more than four missing teeth excluding third molars, had no edentulous spaces within the arches, and each presented normal skeletal relations.
Subjects with anterior or posterior cross bite or open bite, removable dentures, were wearing orthodontic appliances at the time participation, or had more than four missing teeth (excluding 3rd molars), were excluded from the study. The prospective subjects were randomly selected from patient follow-up records.
Institutional research ethics committee approval was obtained from the Thammasat University Research Board. Prior to participation, the study protocol was explained to each subject, and they had the opportunity to ask questions about it, in order to obtain informed consent.
Each included subject filled out a TMD questionnaire that documented the subject’s clinical presentation; popping and clicking of the TMJ, restricted mouth opening, temporalis or masseter muscle tenderness, complaints of neck, shoulder, or facial pain, difficulty chewing, disrupted sleep patterns, and sleep bruxism. The questionnaire qualified the subjects for their need for Splint therapy, but the questionnaire content was not utilized in this study itself. This study’s focus was to determine the difference in the mean right side-to-left side occlusal force distribution discrepancy for each splint, when measured at the four stages of splint adjustment (described below).
The digital diagnostic and occlusal adjustment procedures performed on the splint were carried out on the same day, where the recording and adjustment steps categorized the splints into 4 different groups (Figures 1-5).
-
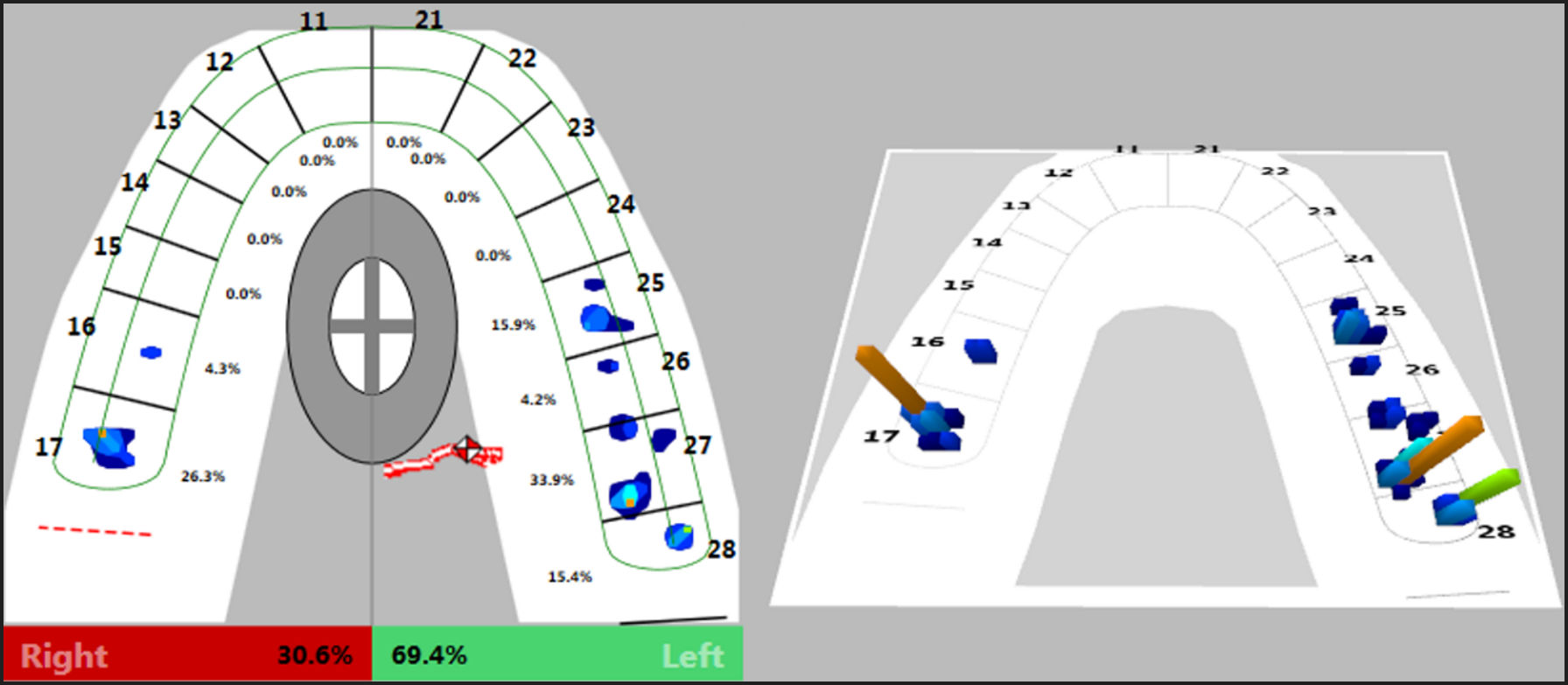
(WS) - Without Splint after being worn for more than 6 months’ time. The initial T-Scan evaluation determined the subjects’ bilateral force distribution and their right side-to-left side force imbalance within their arch (Figure 1).
-
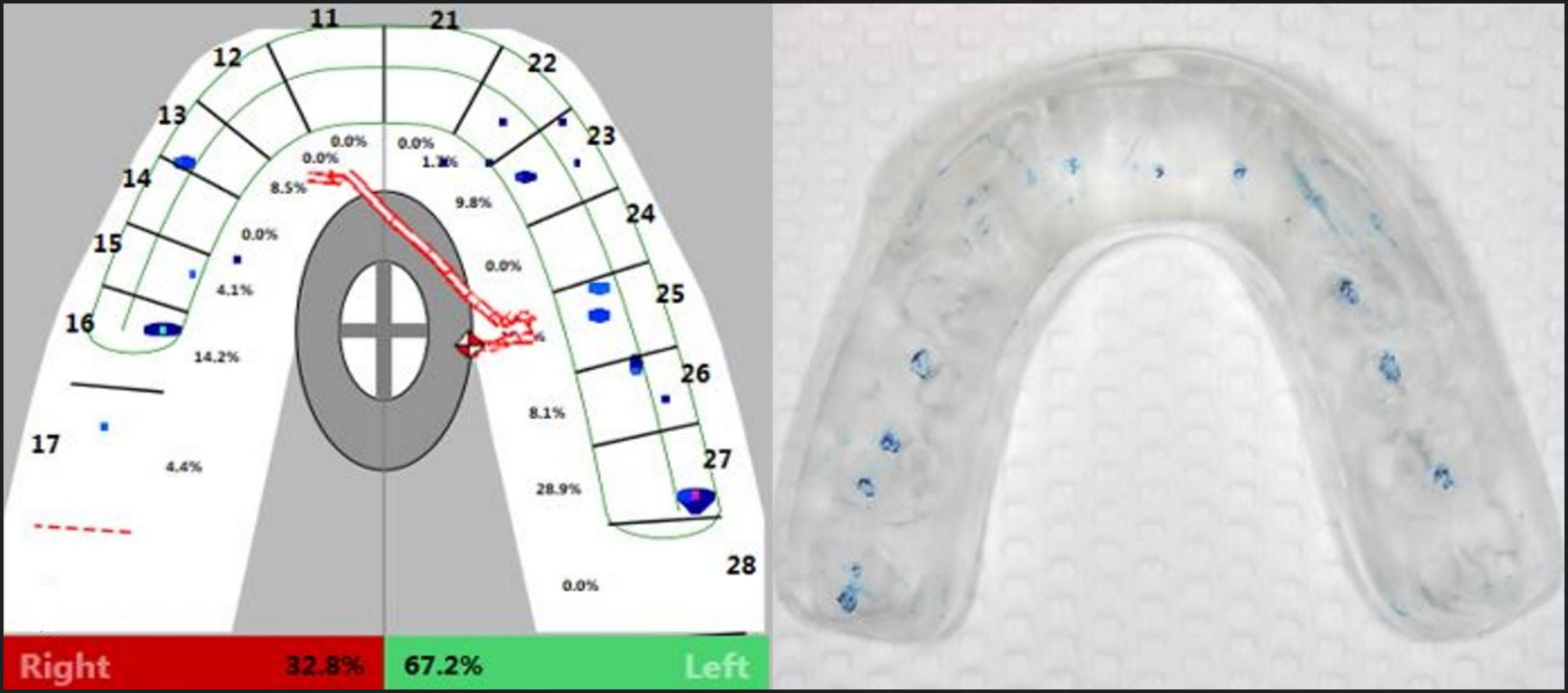
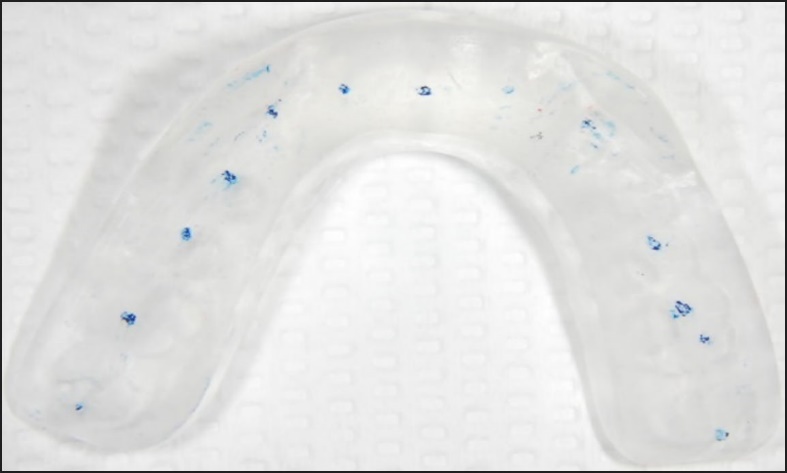
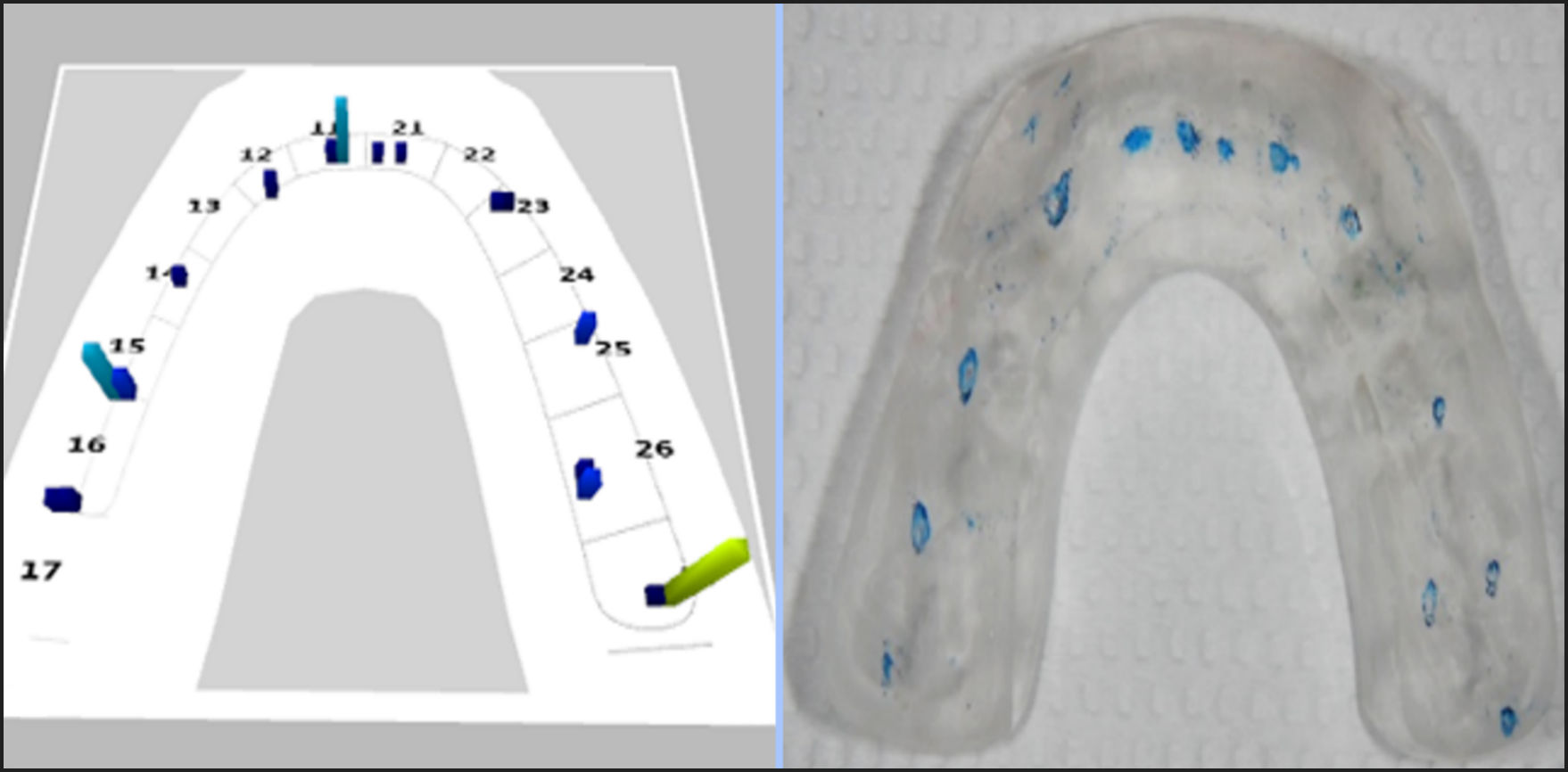
(Pre) – With existing maxillary splint in place - The 1st T-Scan recording was made of the maxillary splint before any adjustments were made. This recording was followed by photographs of the splint’s paper mark distribution made from the patient occluding on articulation paper (Blue Red Radar Articulating Paper, 65 micrometers from Nordin, Harald Nordin S.A., Chailly, Switzerland.) (Figure 2).
-
(Post 1) – The 2nd T-Scan recording made of the maxillary splint after occlusal adjustments were performed by the same operator, using the paper marks as the guideline for adjustment until similar sized, evenly distributed occlusal point contacts were achieved on the splint (Figures 3 & 4).
_baseline_occlusal_analysis_showing_right_side_30.6__-_left_side_69.4__.jpg)
_next_to_the_same.jpg)


Then further occlusal adjustments were performed with T-Scan data guiding the corrections to objectively reduce the specific area on the splint that presented with excessive force. A final T-Scan record was made that assessed the left side-to-right side occlusal force balance achieved by the T-Scan guided adjustments (Figures 5 & 6).
- (Post 2) – Final recording of the T-Scan guided left side-to-right side occlusal force balance.


Prior to the T-Scan recording, each subject had his or her dental arch dimensions and tooth distribution entered into the T-Scan’s tooth chart. This customized the graphical dental arch in T-Scan software, which contributed toward good occlusal arch mapping during recordings. Then, calibration of the T-Scan HD sensor was done to match the sensor’s recording Sensitivity level to the occlusal force strength range of the subject. Proper sensitivity limits the number of red/pink high-force columns/contacts to only three during pre-recording test conditions, and once set properly, the Sensitivity per patient was maintained throughout the 4 dates of measurement.
Subjects were instructed to “bite firmly” into the T-Scan HD sensor, into their Maximum Intercuspal Position (MIP) for 3 consecutive firm intercuspations (Multi-bite recordings), while sitting upright in the dental chair. The single closure that contained the maximum-recorded occlusal force (100% Total Force) was the selected data point of the right side-to-left side force percentage imbalance (Table I), that was used in the statistical analysis with SPSS software (SPSS Inc., Chicago, IL, USA). The Wilcoxon Signed-Rank for Matched Pairs test compared the geometric mean difference of the left and right-ide occlusal force distribution and imbalance, in each of the four splint groups. (Table 1)
Results
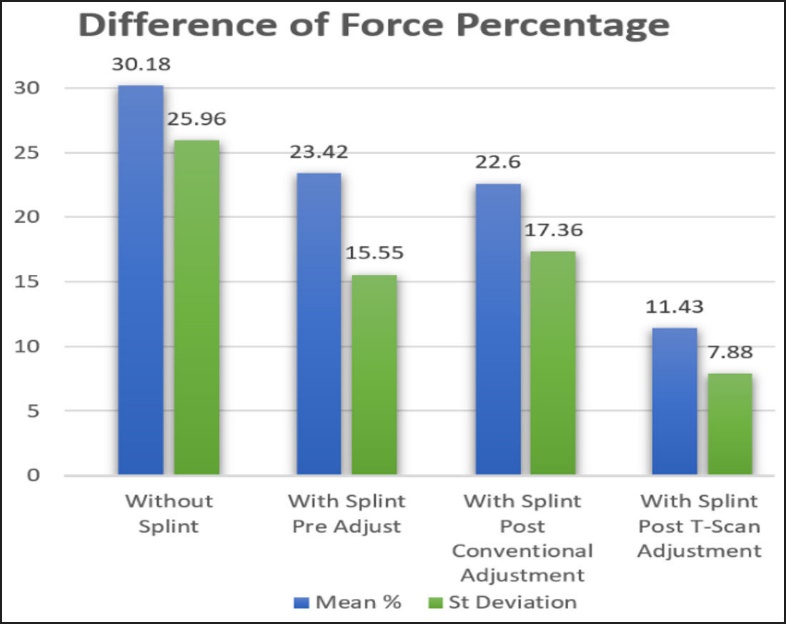
The means and standard deviations of the percentage force differences between the left and right sides were calculated for each of the four groups; a) WS without splint, b) Pre with splint unadjusted, c) Post 1 paper adjustment and d) Post 2 T-Scan adjustment. (Table 2 and Figure 7) However, because the imbalance differences were percentages, it is customary when testing statistical percentages to calculate the geometric means, instead of the arithmetic means. Based upon the geometric means, the unadjusted splint Pre group initially had a greater, but not significant mean imbalance difference compared to the baseline without the splint. The Wilcoxon Signed-Rank test revealed that 1) the paper-only adjustments did reduce the splint imbalance difference somewhat (Post 1 group), but not significantly, 2) the Post 2 T-Scan adjusted group imbalance differences were significantly lower than all three other conditions (p < 0.05). No other comparison was significant.

Discussion
This is the first pilot study involving splints where the splints were actually measured for their adjusted occlusal force imbalance. The results confirm other measured occlusal adjustment studies that show using T-Scan data during occlusal adjustment, provides for improved occlusal balance outcomes while optimizing the occlusal force distribution.22–26 The digital occlusal force data used in this clinical research, provided objective insight into the differences an operator can attain in occlusal force balance, when subjectively adjusting a splint just with paper conventionally, compared to using data to objectively adjust a splint. The Pre to Post 1 changes were negligible using articulation alone to create balance, where only a 1% improvement was obtained over the splint baseline (Pre - 23.42% ± 15.55%; Post 1 - 22.60% ± 17.37%).
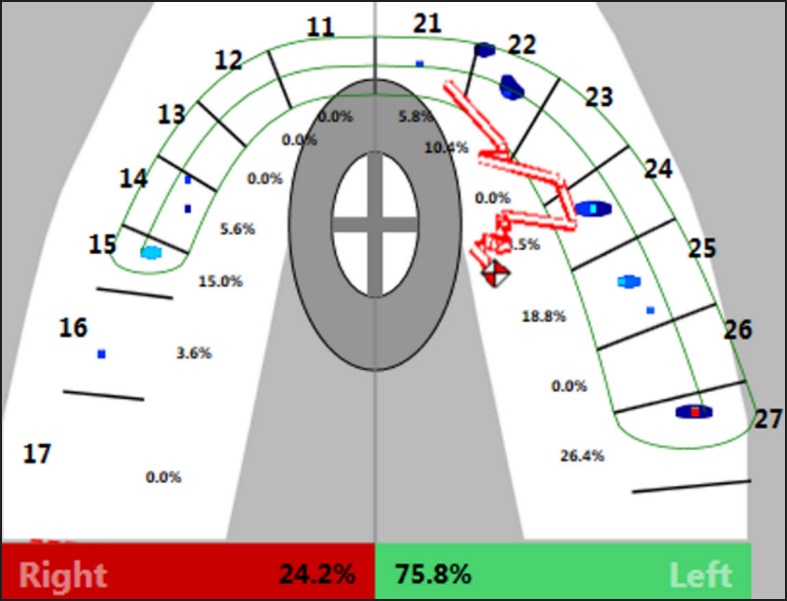
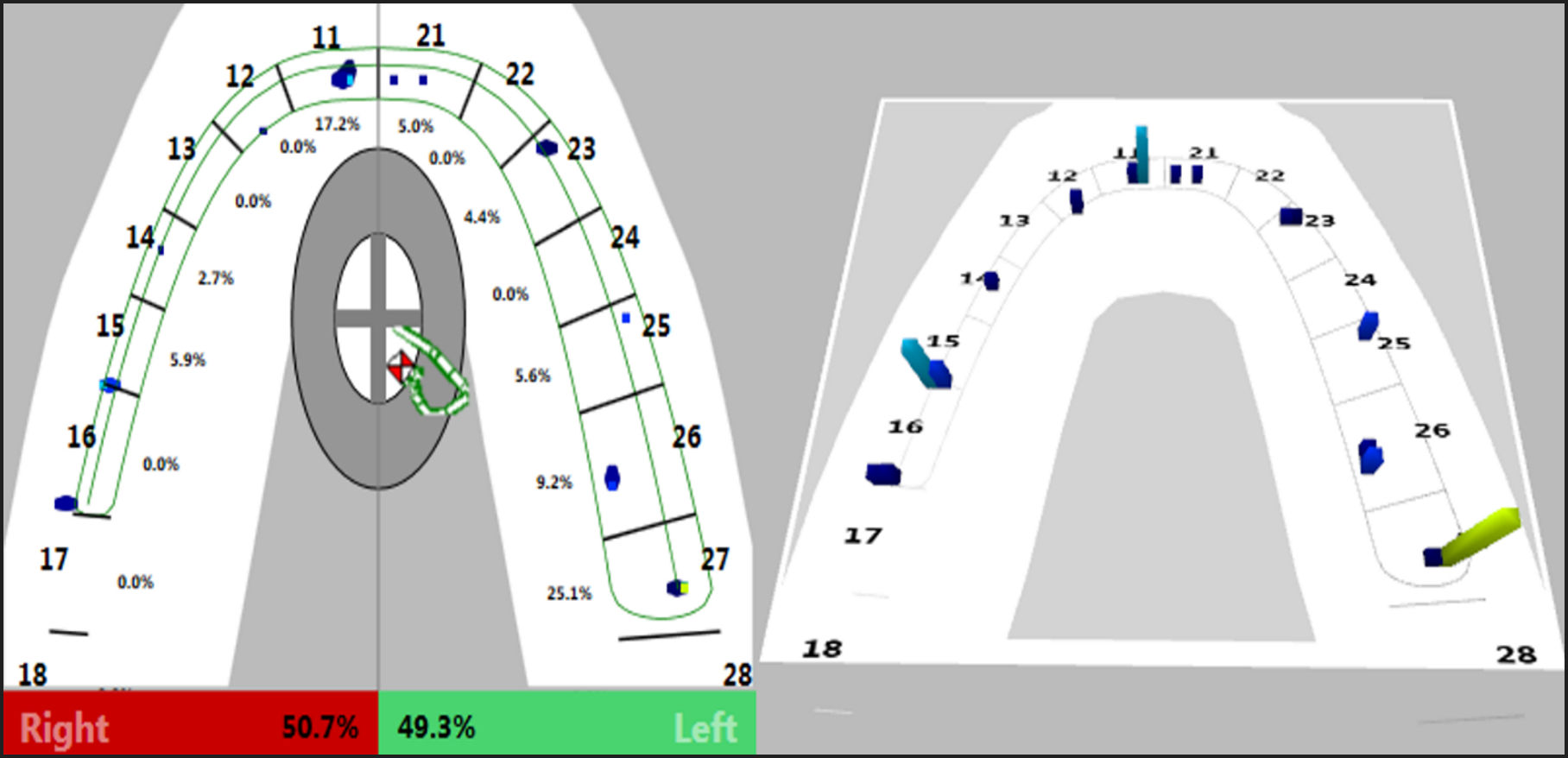
However, The Post 2 T-Scan guided result showed a near 12% improvement over the Pre baseline and the Post 1 results (Post 2 = 11.44% ± 7.88%), with a much smaller standard deviation. This means the Post 2 individual splint force balance results were more similar to each other than were the individual splint Pre and Post 1 results, with doubly large standard deviations. In this study, the conventionally adjusted stabilization splints presented with surprisingly uneven occlusal forces when measured with the T-Scan (Figure 3), where left = 24.2 % and right = 75.8 %). This lack of balance would be detrimental to the treatment goals and outcomes. However, with the T-Scan guided corrections the occlusal force distribution on the same splint closely approached balanced occlusal forces (Figure 4), where right = 50.7 % and left = 49.3%.
The findings also documented that when the conventionally adjusted splints relied on the operator’s “best judgement” and patient “feel” feedback (Post 1 group), these subjective assessments resulted in unbalanced splints (mean force imbalance 22.6% +/-17.4%), compared to computer-guided adjustments using T-Scan data, which resulted in a 50% reduced force imbalance (11.4% +/- 7.8 %). The T-Scan occlusal analysis assisted the operator with obtaining better quality adjusted balance, and in determining the poor occlusal force profile of the paper-only adjusted occlusal contact patterns.
The literature defines a therapeutic occlusion as exhibiting multiple, bilateral posterior tooth contacts with the mandibular condyles physiologically seated, and immediate separation of the posterior teeth by the anterior teeth in all excursive movements.27–29 These “supposed ideal” occlusal contacts are usually identified by articulating paper markings, but research has repeatedly shown that conventional identification of occlusal contacts with articulation paper, inked silk, or plastic ribbon is not accurate.16,18,19 Whereas, the T-Scan actually makes it possible for a dentist to adjust with force data, that helps the operator to measurably obtain these theoretical ideal contact endpoints. This is something that articulating paper is incapable of doing for a dentist.
Full arch maxillary splints are strong barriers to opposing tooth-to-tooth contacts.30 They limit neurologic influences of contacting teeth. But the pulpal and Periodontal ligament nerve fibers of the opposing teeth to the splint, are still fully activated when teeth make excursive or closure contact against the splint. It would seem logical that the better balanced any Splint’s occlusal design is, the better should be the opposing dentition’s neurologic response to the splint, e. g. when trying to obtain a healing effect in a symptomatic patient. Adjusting and delivering any Splint with quantifiable measurement from the T-Scan technology will make a difference in the splint’s occlusal contact force quality at the time the splint is installed. This improved occlusal force profile could have an improved physiologic response of the patient to the splint. In contrast, occlusally imbalanced splints could cause adverse effects or slow down healing, from uneven overloading of one or both Temporomandibular Joints, as the imbalanced splint is worn by the patient.
Despite the small sample size of this pilot study, the findings do illustrate that conventional occlusal adjustment methods are not adequate for delivering an optimal, well balanced splint. This can be clearly seen by comparing Figure 3 and Figure 4 to Figure 5 and Figure 6, where there is no way to tell which splint was more balanced from observing the distribution paper marks on each splint. This is a problem every clinician faces when working solely with articulating paper and one’s “best judgement” (Subjective Interpretation), in that nothing about the ink mark distribution or their relative sizes, adequately describes the occlusal force imbalance.
The T-Scan digital occlusal analysis technology eliminates the Subjective Interpretation of occlusal contact markings, and lessens the need for patient feel feedback, by objectively and precisely quantifying both the occlusal forces on individual teeth, and the distribution of force on either side of the arch. Occlusal adjustments guided by the T-Scan accurately correct which paper marks on the splint are high, medium, and low force contacts, so an operator can make intelligent decisions about what contacts on the splint actually require treatment, and which ones should be left unadjusted. (Figure 6)
LIMITATIONS
This pilot study was conducted on only 11 splints, that limited the reach of the statistical findings. Another Limitation was the skill variance of the operator who carried out the adjustments on the splint, both with and without T-Scan guidance. A clinician’s skill in making corrective adjustments subjectively is always a Limitation, because there is no measure of one’s “best paper mark judgement”. But to counter this limitation, T-Scan data sets graded the capability of the single operator, by quantifying the imbalance that remained after Subjective Interpretation adjusting (Post 1 group), and after the T-Scan guided adjusting (Post 2 group).
A 3rd Limitation was no therapeutic effects of the conventionally adjusted and T-Scan adjusted splints were studied, despite that a TMD questionnaire was filled out by each included subject before study participation. Further studies with larger sample sizes, that include therapeutic responses to the differing splint adjustment methods, are warranted. This type of study would better elucidate the effectiveness that a well-balanced Stabilization Splint has on symptom resolution.
A 4th possible limitation was that no splint Occlusion Time or Disclusion Time data was reported upon, which are also measures of the quality of a splint’s occlusal design. As this study focused solely on the quality of the right-to-left force % balance created first by an operator subjectively followed by using T-Scan data, there was no attempt to gather or report on other Measured Occlusion parameters. Balance is considered a very important parameter of splint design, as it is thought that a well-balanced splint will establish better occlusal harmony for the patient than they were experiencing from their own occlusion.
CONCUSIONS
Conventionally adjusted maxillary full arch Stabilization Splints, using articulation paper marks and an operator’s clinical judgement to guide the performed adjustments, demonstrated markedly worse bilateral occlusal force imbalances than did splints that were adjusted using the T-Scan technology. The majority of the conventionally adjusted (and supposedly well-balanced) splints did not provide the ideal occlusal contacts they were intended to provide, until they were further corrected by using measured occlusal force data. Computer-guided occlusal adjusting provided the splints with a more precise occlusal force balance, than did unmeasured, articulation paper-based, subjective occlusal adjusting.
Funding Statement
No Funding was received for this activity.
Potential conflicts
The RB Kerstein is a clinical consultant to Tekscan Inc., South Boston, MA USA and has received an annual stipend. However, he receives no compensation from the sales of any Tekscan products. The three additional authors claim no potential conflicts of interest.