


INTRODUCTION
The Costantinides et al’s Systematic Review’s search found 144 references within the dental literature, summarily dismissed 117 as duplicates (117 duplicates?), added one reference manually, dismissed 18 because they did not have full text copies and removed seven more as “inadequate” for various reasons.1 Then, after reviewing the 3 remaining articles, they concluded: “The scientific evidence does not support the usefulness in clinical practice of the jaw-tracking devices to diagnose temporomandibular disorders because their diagnostic reliability is poor.” Although this conclusion regarding all TMDs is technically correct on its face, it cleverly switches its indictment from the evaluation of just TMJ internal derangements (as the title indicates) to the complete diagnosis of all temporomandibular disorders. Their true statement can also be made with respect to MRI, CBCT and all other TMD diagnostic approaches, since no single device or technique can accurately diagnose all TMD. Neither the RDC/TMD nor the DC/TMD can accurately diagnose all cases of TMD.4–6
To their credit, the authors did recognize that the three articles they chose to include in their review all projected a high risk of bias. Consequently, by their own admission, they obviously ignored 98 % of the literature upon which any conclusions could be based, but managed to find three highly biased articles to support their conclusion that jaw tracking has no value in TMD diagnosis. It is clear that these authors are not aware that Jaw Tracking has unique value beyond just detecting internal derangements of the TMJ.
Regarding the three references that were reviewed, two of the cited references were published auf Deutsch and neither of them condemns axiographic measurements as having no usefulness in the diagnosis of TMD. Most likely those two publications were written with an understanding that TMD cannot be diagnosed by any single device. With respect to the third article by Manfredini et al, they only compared the agreement between MRI and Kinesiography for detecting internal derangements, not for diagnosis of TMD. Manfredini et al were also accused by the manufacturer of using the K6 Jaw Tracker contrary to its published indications for use.7 This Systematic Review could be better described as a Systematic Attack against the use of all jaw tracking devices and provided no unbiased support from within the scientific literature for its conclusion. In point of fact, the majority of the disregarded scientific literature strongly disagrees with their conclusions and most often describes significant benefits from the application of Jaw Tracking to patients suffering from TMD.
Concluding that Kinesiography is unreliable compared to MRI in the above reference as competing devices to diagnose TMD reveals an inadequate comprehension of the nature of both devices. Jaw Trackers can reliably record jaw motion and MRIs reliably image the TMJ, but each one requires clinical interpretation of the significance of their records. It was the lack of reliability of the interpretations that was previously at stake and found wanting in that article. When authors have an inadequate understanding of the technology, as was probably the case in that article, reliable interpretation of the significance of either jaw motion recordings or MR images can be absent. However, incorrect clinical interpretation does not diminish a device because, although each instrument records data accurately, neither one interprets data significance.
MRI & JT ARE COMPLENTARY
Tracking jaw motion by means of Kinesiography, Electrognathography, Axiography, etc. and the taking of MR Imaging provide very different and highly useful information with respect to TMJ status and the quality of masticatory function, but neither one provides a stand-alone capability to diagnose all 40 + temporo-mandibular disorders.7 In fact, it is clearly absurd to compare MRI to Jaw Tracking as if they represented alternative stand-alone (one or the other) exclusive all-encompassing TMD diagnostic tests. The unsupportable opinion that MRI and JT must be stand-alone alternative TMD diagnostic tests and that one must be chosen over the other constitutes a disservice to all TMD treatment providers and their patients.
MRI and Jaw Tracking (JT) both unquestionably provide reliable, but very different data describing the conditions within the TMJ. However, they are not alternative, stand-alone diagnostic tests for “Temporomandibular Disorders.” Neither device is self-interpretive and both of them require a specific interpretation by a very knowledgeable clinician. It is most likely that the data interpretation within the Systematically Reviewed Manfredini article was unreliable because the JT never provides a “diagnosis.”
For those who understand technology, MR Imaging and Jaw Tracking have distinct capabilities with only limited overlap, recording substantially different information. While MRI provides static grey-scale images of the TMJ, revealing the morphology and important aspects of the physiology, jaw tracking records the dynamic function of the structures and allows an estimate of the degree of successful adaptation to a current disorder. In terms of their cost/benefit ratios, JT represents an inexpensive screening procedure easily accomplished within a private practice, while MRI is limited by its high cost to applications where the presence of a TMJ mal-condition has already been predicted. Consequently, JT is an ideal pre-cursor to MRI and that is how it is most often used in thousands of TMD practices world-wide.
EXAMPLES
Typical of jaw tracking records, the data in Figure 1 A and (B) is totally in agreement with the MR images (C) and (D) regarding this non-reducing TMJ disk displacement (DD). However, the records (A) and (B) also suggest a lack of successful functional adaptation (the erratic frontal and horizontal movements). In this example the jaw tracking interpretation justified the expense of obtaining the MR images. While the images of the TMJ revealed the present morphology, only the motion recordings revealed the aberrant dynamic function.
_recorded_by_egn_is_clearly_limited_(a)__at_negligible_cost.jpg)
Can the jaw motion records presented in Figure 1 possibly be seen just as alternatives to the MR Images or can either one can be considered sufficient by itself? In this example, as is often the case, the jaw motion recordings indicated that an internal derangement was present without the expense of an MRI, but also justified procuring an MRI series for this patient due to the lack of successful adaptation. In other cases, the adaptation has been recorded as very good, eliminating an unnecessary MRI expense. A complete diagnosis is only possible with a comprehensive approach. One diagnostic test can never be expected to provide every piece of information needed for a thorough TMD diagnosis. Just as one treatment cannot be expected to be successful for all TMDs, no single test can ever be expected to correctly diagnose all 40+ TMDs.
If one has a pre-conceived notion that a particular relationship is not statistically significant, the creation of a complex logistic regression model that includes factors that are not related can reduce the overall predictive capability of the model.8 For example, to conclude that occlusion has no relationship to internal derangement of the TMJ requires the assumption that one portion of the mandible (the condyle) can change position (disk displacement, condylar necrosis, etc.) without the alveolar portions of the same mandible (a single bone) changing its relationship to the maxilla, which of course is a physical impossibility. This has not prevented the preposterous claim that occlusion has no relationship to TMD. Considering the known sensitivity of the teeth in occlusion to a micron level of change, any change at either condyle will most certainly be detected at the occlusion. Whether the change in the occlusion is causative or the result of the TMJ internal derangement is immaterial because mitigation can be accomplished either at the TMJ surgically or at the occlusion (splint or occlusal adjustment) to resolve these TMD conditions. In contrast, Cognitive Behavioral Therapy has not been successful in reducing even the emotional symptoms associated with TMJs. This is not a failure of CBT as a technique, but simply an indication that the emotional factors in TMD are usually secondary to physical factors. In fact, correction of the physical factors has been shown to greatly alleviate the emotional ones,9 supporting the alternative hypothesis that TMD is nearly always a physical condition that provokes the secondary emotional symptoms of depression and anxiety. Any effort to detect or measure somatization in the presence of a physically painful condition is contraindicated in medicine, unless all of the symptoms are determined to be medically unexplained symptoms (MUS).10
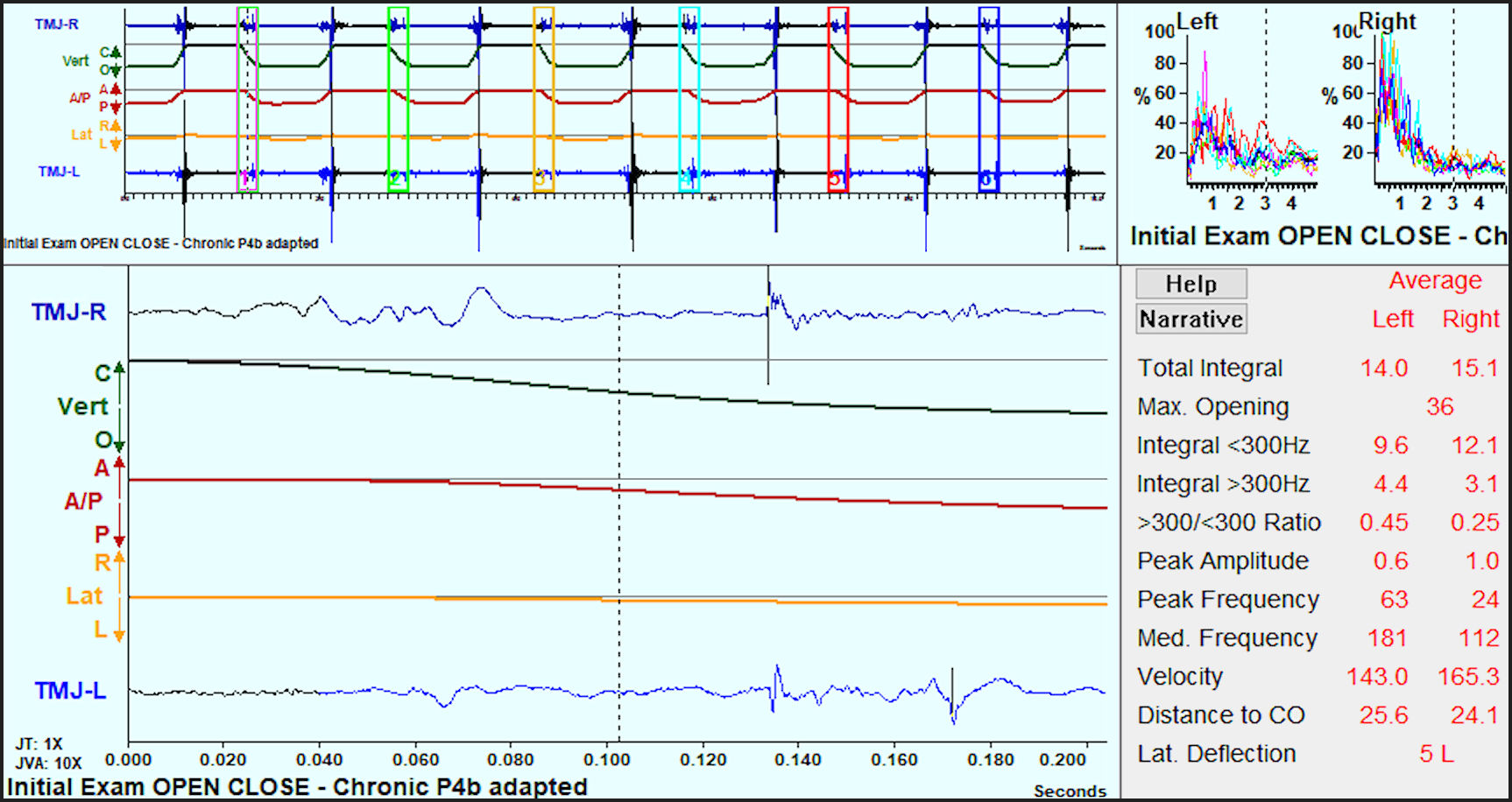
The reality is that jaw tracking, coupled with Joint Vibration Analysis, is very often used as a quick and inexpensive screening test to differentiate whether an MRI (for internal derangements) or a CBCT (for a degenerative condition) is more likely to further enhance a patient’s diagnosis. See Figures 2A & 2B. In this example of a chronic disk displacement without reduction, the JVA and Jaw Tracking motions indicated good adaptation of the TMJ, negating the need and the expense of MR imaging. However, if MR imaging had been pursued instead without jaw tracking, it is very likely the DD would have been discovered, but inconclusive data regarding the degree of successful adaptation of the TMJ would have been captured. JVA with jaw tracking provides information that can enhance the accuracy of a clinician’s understanding of the current dynamic functional status of the TMJs and reveal a situation when there is no need for intervention.

__no_.jpg)
Note: Static greyscale images of the TMJ closed and open require a knowledgeable and experienced radiologist or experienced TMD-treating clinician to spend the time to subjectively “interpret” the images, combine the interpretation with other sources of information and then decide if the disk is in a normal relationship to the condyle, is abnormally related, is well adapted and then whether any treatment is likely to improve the functionality of the TMJ. This analysis is required because treatment of TMJ is not always successful.11 Likewise, the interpretation of jaw motion recordings also requires an understanding of normal movements during various activities, information that is rarely present in dental schools’ curricula.
The patient’s reported history and clinical evaluations have repeatedly been shown to be less than sufficient for accurate diagnoses.12–14 Compared to Axis I diagnoses of the RDC/TMD, tomograms often produce unexpected findings.15 The Axis I diagnostic criteria for the most common TMJ intra-articular disorders from the recently updated DC/TMD have been described as “appropriate for screening purposes only”16 and that “a definitive diagnosis for TMJ intra-articular disorders requires computed tomography or MRI.”16 With respect to the diagnosis of arthritis/arthroses, CT is decidedly more reliable.17–19 JVA with JT is ideally suited to provide the information necessary to choose the best imaging technology for a specific patient’s condition.
JT records also provide significant information about the smoothness or erratic nature of joint function and movement variability that is not available from any other source. TMDs do not always involve the TMJs. Unless one is prepared to image every TMDs patient, including those with normal functioning TMJs, some less costly and more convenient method of detecting joint damage is highly useful. Jaw tracking with JVA is designed just to detect damage in the TMJ, but JT mastication analysis can reveal the quality of overall masticatory function.
JAW TRACKING DIAGNOSTIC CONTRIBUTIONS
In direct contrast to imaging, Jaw Tracking, which can be done quickly and inexpensively in a private practice setting, detects the abnormal mandibular deviations and deflections that are commonly associated with TMJ dysfunction. When applied together with JVA, the JT can reveal TMJ damage with high sensitivity and specificity.20 The specificity with respect to normal control subjects has been previously measured at 98.3 %,21 only rarely resulting in any false positive indications. Damaged TMJs that adapt successfully can still function very effectively and not require treatment (F4). See Figure 3.

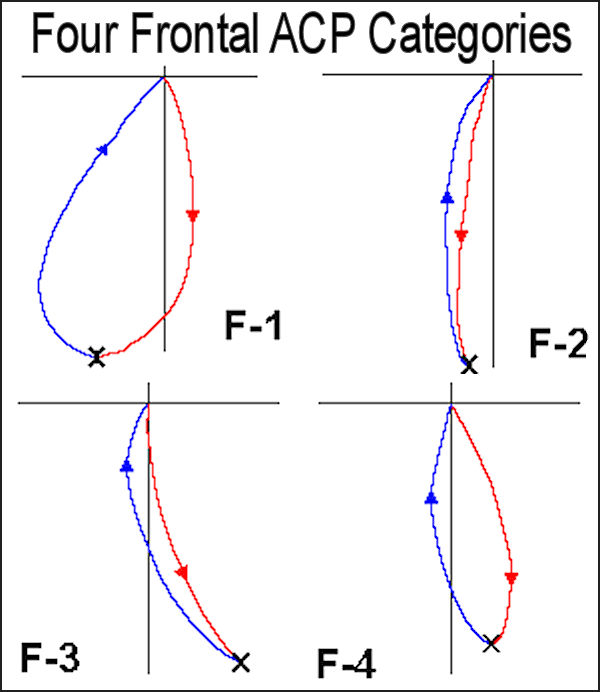
In addition to detecting the presence of internal derangements, JT chewing records can be used to evaluate the masticatory functional capability of the patient,22,23 By recording mastication, the JT can be very useful in evaluating the degree of successful adaptation. The characteristics of the Average Chewing Pattern (ACP), such as velocity, smoothness, variability and a restricted envelope of motion reflect the overall conditions within the TMJ.24 Frontal plane Average Chewing Patterns (ACP) comprise four categorical conditions. See figure 4.

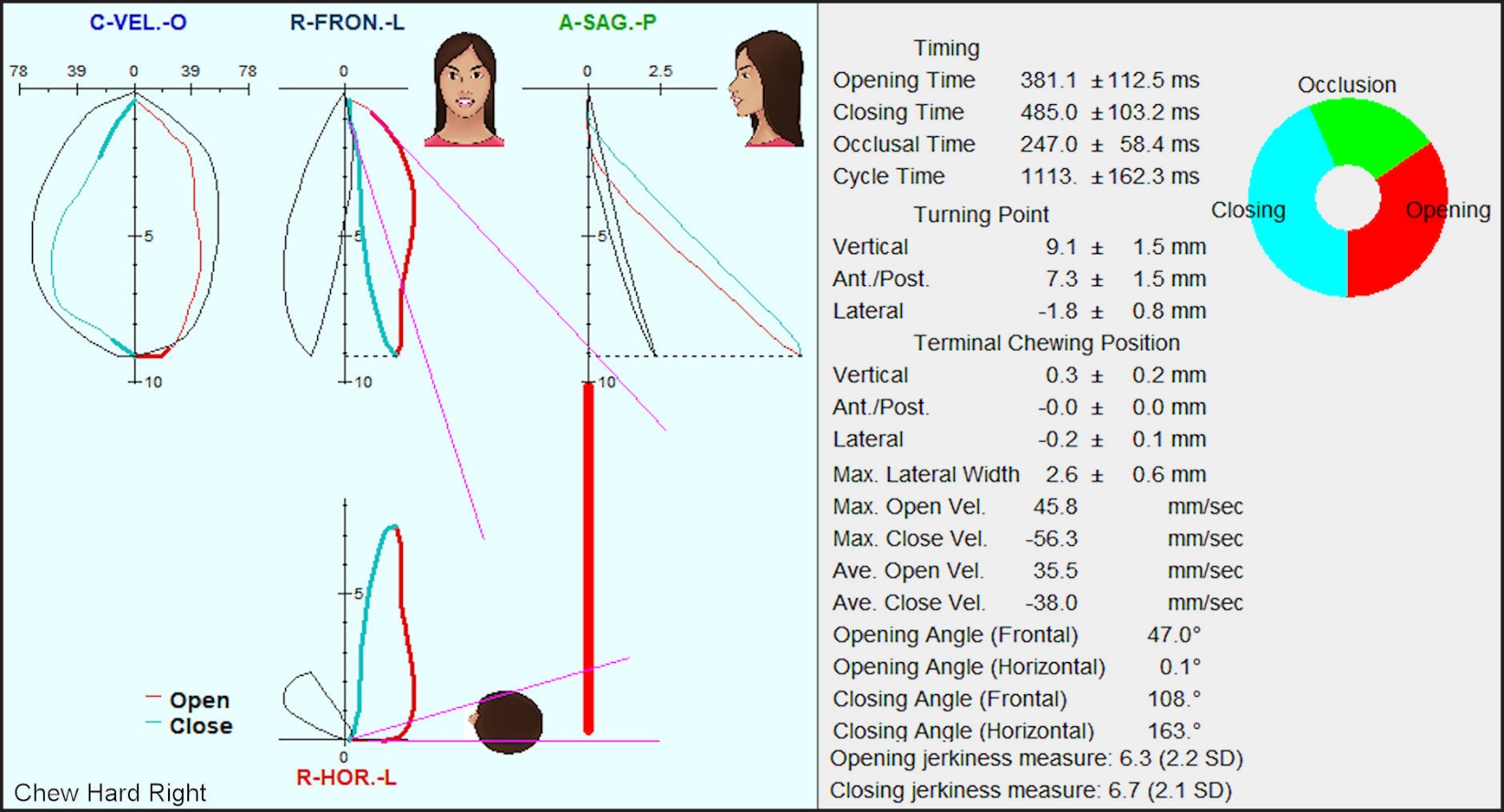
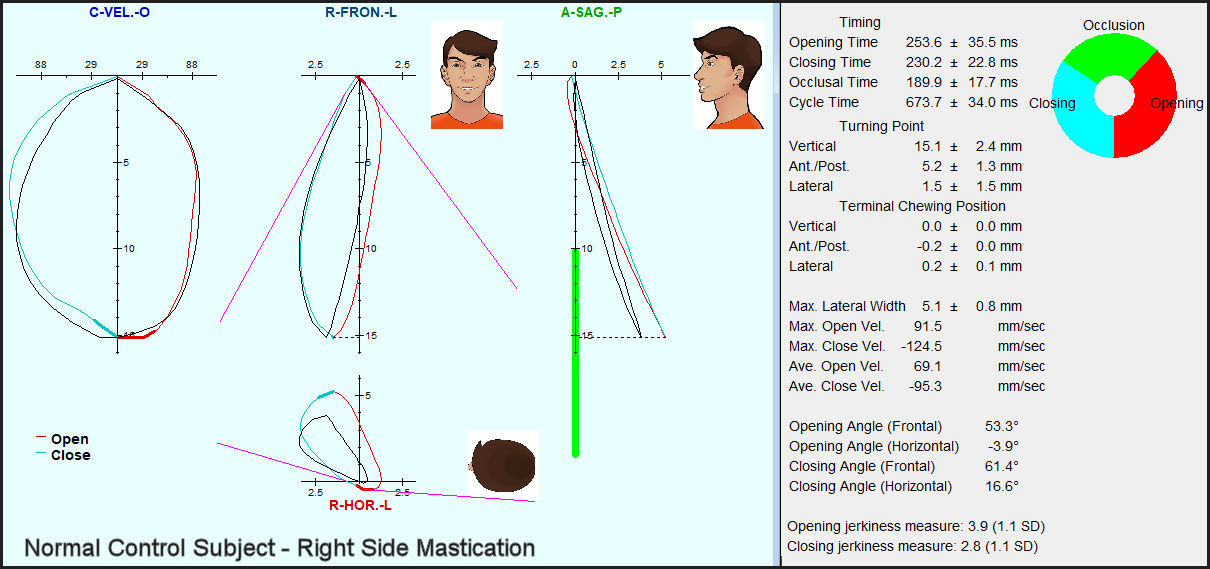
The normal pattern has been labeled as F1. A patient with a reducing displaced disk chewing on the unaffected side exhibits a distorted opening path due to the reduction (F2). Unilateral non-reducing displaced disks (DD) distort the ACP by deflecting the Turning Point toward the affected side (F3) when the subject is chewing on the unaffected side.25 A patient with well-adapted bilateral non-reducing displaced disks produces an ACP that appears closer to a normal pattern (F4). TMJs, that are poorly adapted reduce the patient’s ability to masticate, which may lead to secondary gastrointestinal and/or nutritional deficits.26 See Figure 5. A sample of a control subject’s ACP is useful to discover how an undisturbed masticatory pattern appears. See Figure 6. The astute dentist understands that the primary purpose of the masticatory system is mastication and that a dentist’s first job should be to restore and maintain good masticatory function. Perhaps the most important fact overlooked by Costantinides, F. et al in their Systematic Review of Jaw Tracking is that the value of Jaw Tracking with respect to TMD is not limited to just distinguishing the type of internal derangements of the TMJ. The JT evaluation of masticatory function not only provides a pre-treatment assessment of the TMD patient’s functional capability, but also provides a reliable post treatment outcome measurement of the success or failure of any TMD treatment. Since the first critical purpose of the masticatory system is efficient mastication, measuring that seems to be the most obviously important feature of any Jaw Tracking device. Since the cost of obtaining a Jaw Tracking record is such a tiny fraction of the costs associated with an MRI, many TMD practices actually record Jaw Tracking for free because it can save valuable time, expense and provide an objective measure of improvement after all treatment is completed. While no dental practice can afford to purchase an MRI machine and few have a purchased a CBCT, a Jaw Tracker can be obtained with a comparatively minor capital investment.


MRI DIAGNOSTIC CAPABILITIES
An MRI is represented as a series of pictures that are slices through the TMJ and requires an astute “read” before any information is available. For most cases, a highly skilled radiologist or highly experienced TMD practitioner must interpret the images to provide a reliable MRI “Read.” A majority of dentists do not and most cannot consistently read all of the pathology from an MRI. The forced objective of concluding with categorial results, (DD with Reduction, DD without Reduction, Degenerative Joint Disease, etc.) makes the process inevitably prone to errors because the nature of the TMJ is not categorical. There are many possible degrees of conditions and combinations thereof present in the TM joints (even just between non-displacement of the disk, partial or complete disk displacement with or without reduction).
Since there is no universal agreement as to exactly what is the “normal” position of the disk, a marginally normal/abnormal position will always be in contention. A review of the literature did not provide evidence to support or refute an association between joint effusion and self-reported TMJ-pain or between joint effusion and arthralgia as implied by the RDC-TMD.19 In spite of limitations and the cost of getting an MRI in terms of time, material and convenience, for the patient with significant non-adapted TMJ damage, an MRI can be very beneficial in revealing the patient’s actual TMJ morphology and physiology. The improved understanding can lead to more effective treatment decisions.
CONCLUSIONS
Comparing MRI and Jaw Tracking as if they were alternative stand-alone diagnostic tests for TMD is absurd. Each device has its unique capabilities and both can contribute to more accurate diagnoses. It is understood that TMD represent a category of at least 40 distinct conditions, many of which are primary conditions outside of the TMJ. While MRI reveals the morphology and physiology of the TMJ, Jaw Tracking can reveal the quality of overall masticatory function, which can be considerably more important to many TMD patients. No single device or diagnostic technique can accurately diagnose all TMD. Thus, multiple efforts must be completed to achieve a reliable, comprehensive diagnosis, which preferably should precede treatment. Jaw Tracking adds substantially to the diagnostic process.
It is not reasonable to approach the TMD patient by “trial and error,” or by applying a standard conservative treatment to see if the patient gets better or worse. It is preferential to first develop a thorough diagnosis and to understand all of the factors present, which allows the development of a corrective treatment plan rather than being limited to “managing patient symptoms palliatively.” That is, the diagnosis should precede treatment and not be based upon the success or failure of one “usual or customary” treatment. Palliative treatments should be limited to emergency measures for an acute situation or terminal conditions, just as they are in general medicine. Instead, treatment should be definitively focused on the individual patient’s etiologic factors once they are understood. Thus, MRI and Jaw Tracking both routinely provide important information that is used every day by thousands of clinicians who insist on accurate diagnoses prior to initiating TMD treatment.