



INTRODUCTION
The International College of Cranio-Mandibular Orthopedics (ICCMO) published a position paper in 2011 which acknowledged the importance of dental occlusion in TMD and asserted the effectiveness of a physiologic and functional approach to TMD treatment.1 The paper emphasizes that a therapeutic neuromuscular orthosis, combined with diagnostic data, and treatment modalities like Ultra-Low Frequency Transcutaneous Electrical Neural Stimulation (ULF-TENS), often results in a successful treatment outcome. This conclusion supports the scientific validity of the physiological/functional basis of TMD, rather than a somatic symptom disorder etiology.
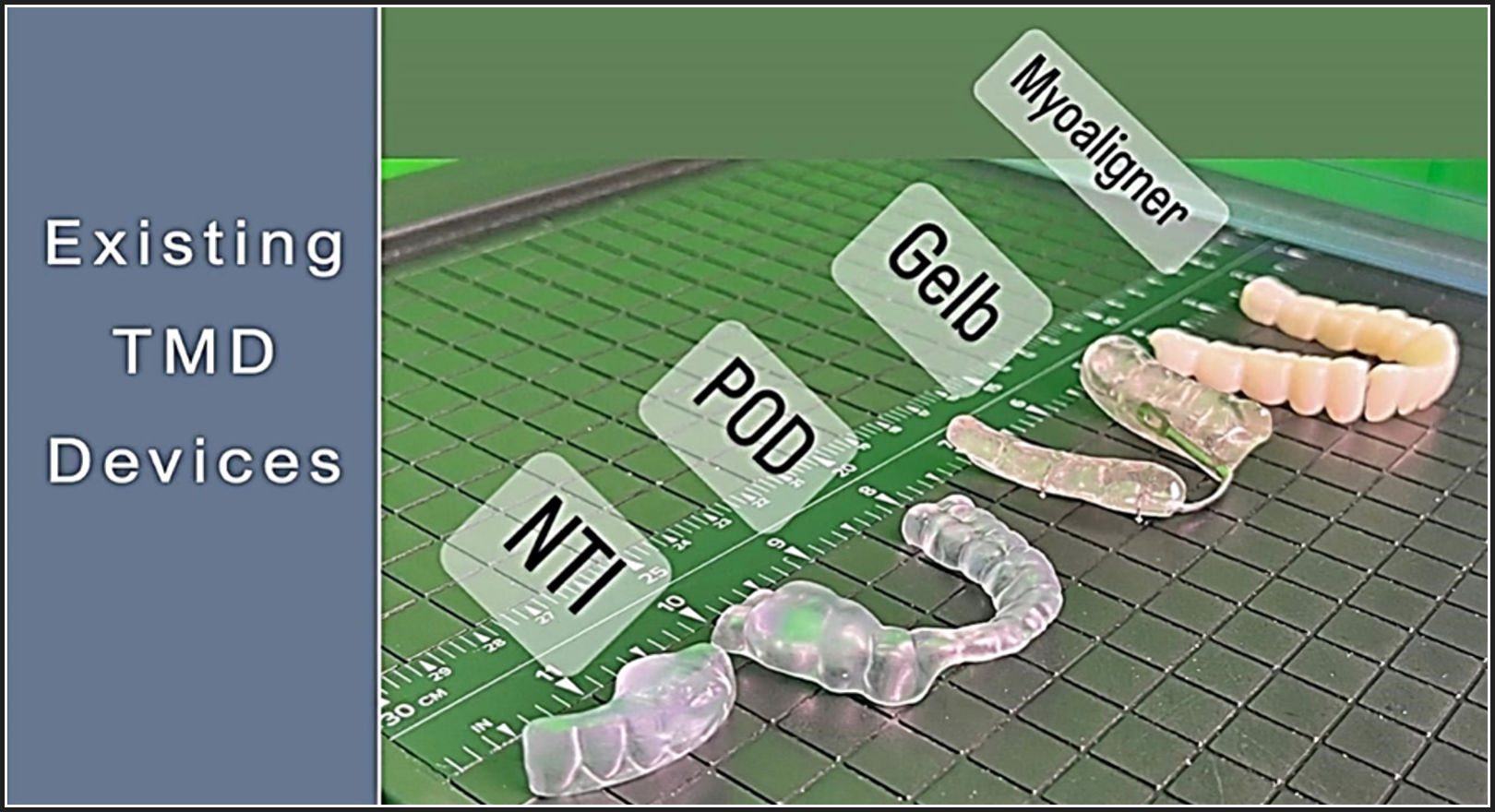
Unlike many other TMD orthotics, such as the flat-plane Michigan splint, which may be limited to nighttime wear, Myoaligner® orthotics are designed to be worn day and night. See Figure 1. This contributes to the re-programming of muscle memory, healing and bio remodeling of hard and soft tissue, as others have also observed.2 Another unique feature of Myoaligner is the 3-part segmented design which allows for the natural flexion of the mandible, avoiding muscle compensation at a moment in time, leading to enhanced functionality and comfort while minimizing orthotic failures.

Mandibular flexion (MF), a biomechanical phenomenon where the mandible deforms due to masticatory muscle contractions. This deformation can impact clinical outcomes, particularly in implant and prosthetic treatments.3 Dividing long spans in prosthetics can help mitigate the stress caused by MF.3
Based on the research on mandibular flexion and its implications for full-arch rehabilitations, the unique segmented design of Myoaligner may be preferred over traditional full-arch unsegmented orthotics for several reasons.
Full arch orthotics may create a rigid structure, depending on the material that does not accommodate the natural flexion and movement of the mandible. Although not well established in the literature, flexural stress on the mandible may lead to stress on the TMJs and masticatory muscles such as the masseters and temporalis muscles, during parafunctional activities like clenching and grinding. Myoaligner orthotics are designed with 3 separate lines of draw for the anterior and both posterior segments of the arch, while full arch orthotics must be designed with one line of draw. A wider occlusal table could potentially hinder tongue function and may require accommodation.
Oral-pharyngeal reflexes are often nociceptive and can be triggered by the presence of foreign objects or other stimuli within the mouth.4 Traditional bulky orthotics can inadvertently stimulate these reflexes, leading to discomfort or involuntary muscle responses. The Myoaligner’s segmented 3D design protocols aim to maximize tongue space occupation by minimizing material use and avoiding triggering of protective oral-pharyngeal reflexes, thereby ensuring comfort and preserving essential oral functions.
Myoaligner devices can serve as a functional solution that provides pain relief, allowing patients to speak, and swallow with ease supporting myofunctional treatment objectives. By addressing poor jaw alignment around the clock, the process of bio remodeling of the injured TMJ tissues is expected to be accelerated, offering patients improved compliance and faster relief. Santiago et al showed that functional appliances may be formational appliances.5
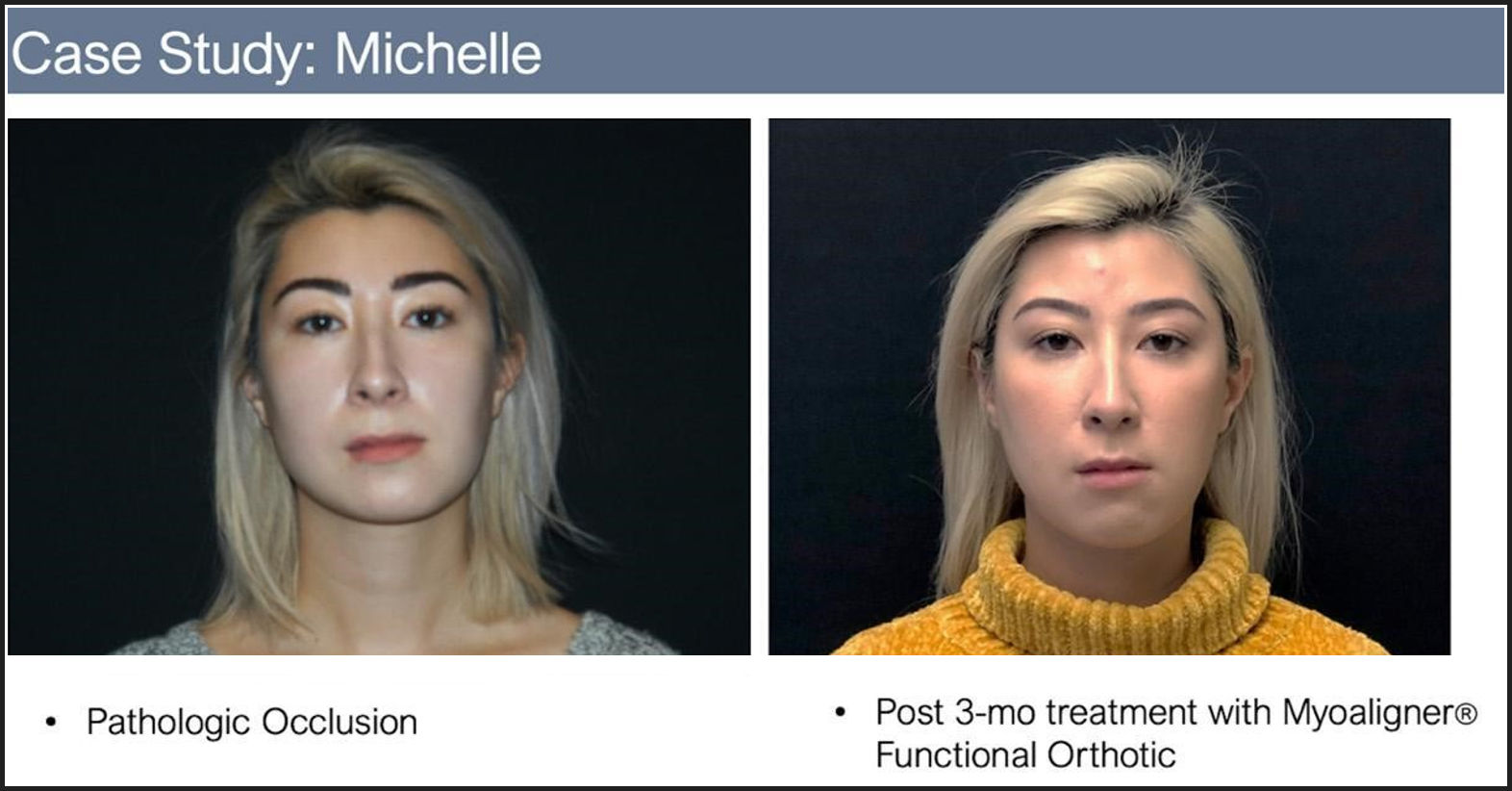
The subject in this case study, Michelle, came to me seeking a non-surgical option for addressing her facial asymmetry, left posterior crossbite, and canted smile, that was causing pain, discomfort, and cosmetic issues for the patient. See Figure 2. Michelle had been told her only option was jaw surgery with its many risks including pain, bleeding, infection, time for recovery, as well as the irreversibility of the procedure. This was not a case for any simple irreversible treatment, minimal occlusal adjustment, but a major TMD/orthognathic surgical correction. She was provided with a minimally invasive alternative option using the Myoaligner treatment protocol. A nighttime only appliance might have reduced the pain if used for the rest of her life, but it could not have corrected this degree of maxillo-mandibular mal-relationship. This patient also desired cosmetic improvement as much as pain relief.

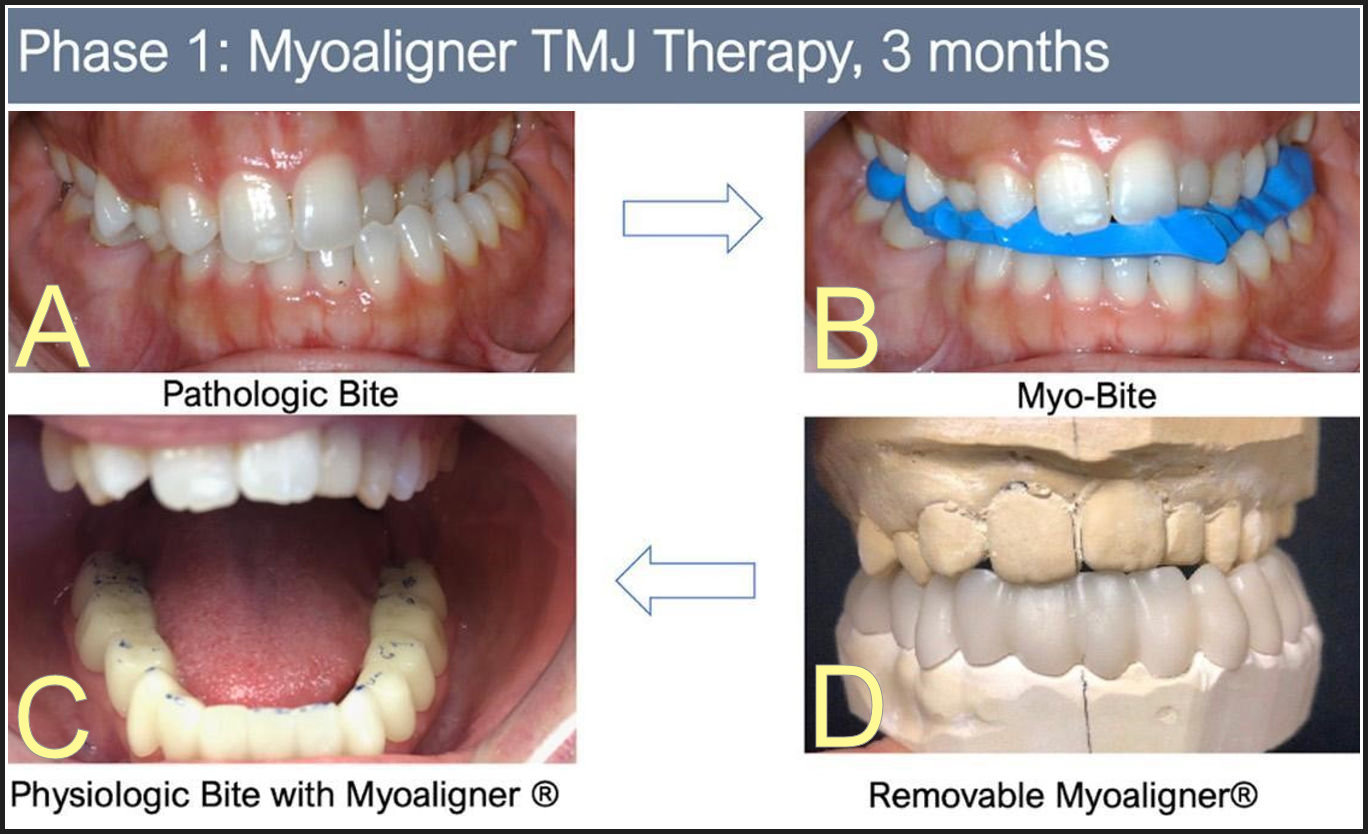
In phase one of her treatment, Michelle’s physiologic bite “Myobite” was recorded, and a Myoaligner fabricated. Following 60 minutes of treatment with ULF-TENS, the patient’s left side decompressed by moving in all three planes, positioning the mandible into a more ideal physiologic rest position. Physiologic rest is defined as the position of mandible where the muscles are at rest; where her mandible should be resting all day long except for when she chews or swallows.6 The “Myobite” position was achieved by recording the position of the mandible on physiologic trajectory 2 mm above physiologic rest, to allow freeway space. These images, See Figure 3, show the dramatic change in occlusion and decompression of the posterior space of Michelle’s TM Joints which immediately alleviated the TMJ pain and discomfort she was experiencing.
_and_myobite_in_place_(right).jpg)
Michelle’s Myobite was obtained using ULF-TENS (Myotronics, Inc. Kent, WA, USA) to relax the musculature while taking a bite registration. Ulf-TENS has been FDA cleared for relaxing all masticatory and facial muscles innervated by the 5th and 7th cranial motor nerves,7 including the lateral pterygoids, because the stimulation is neurally mediated. The resulting movement is upward and forward because normal closing muscles overpower their antagonist opening muscles, unless they are in spasm, in which case there is instead an opening motion until relaxation of the elevators has been accomplished. Anatomically, it is impossible to stimulate the motor fibers of the trigeminal nerve within the TMJ before it trifurcates into v1, v2 and v3 and not produce contractions in every muscle that it activates.
ULF-TENS has also helped in the determination of a therapeutic occlusal position for several decades by using a patient’s own muscles to produce a muscle-compatible intercuspal position.8 The neuromuscular centric braces the condyle against the eminence rather than the posterior wall of the fossa, compressing the posterior attachment tissue as the original “rearmost centric relation position” did. This places the condyles similar to the Dawson model, and for TMD patients it especially accommodates well adapted TMJs, “…adapted joints may within certain conditions function with the same degree of comfort as intact, properly aligned condyle disk assemblies in centric relation.”9 Additionally, the neuromuscyular centric position has been demonstrated to reduce movement-evoked pain in patients with TMD, and improving jaw motor function.10
Neuromuscular dentistry, as described by Ira L. Shapira, focuses on the significance of the entire stomatognathic muscular system in determining the mandible’s best jaw position when the teeth are not in occlusion. The concept emphasizes the importance of the rest position, where the teeth are positioned in preparation for the next closure, but not in occlusion, by maintaining a balanced and minimized muscle tonicity.11
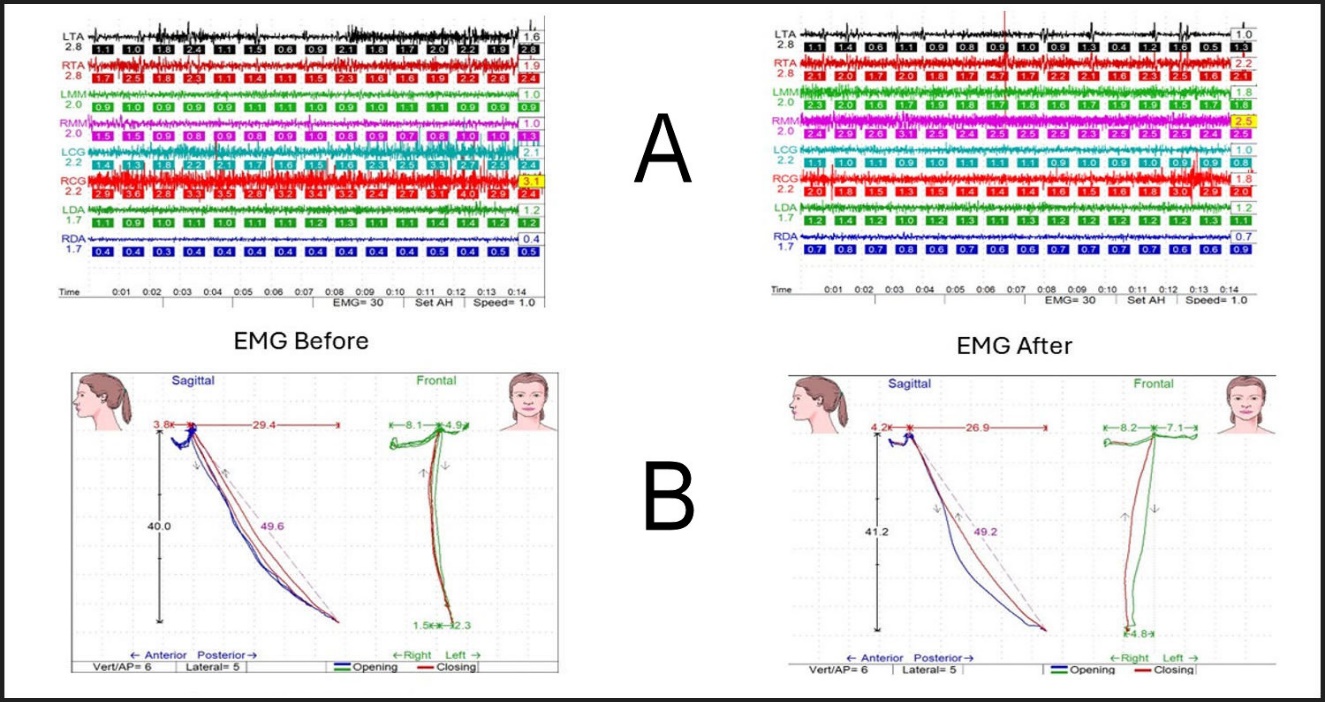
The ICCMO position paper on neuromuscular dentistry and the role of the autonomic nervous system discusses the importance of sphenopalatine ganglion (SPG) blocks and neuromodulation in managing various orofacial pains, including those associated with TMJ disorders, headaches, and migraines.1 It underscores the significance of the trigeminal nerve in these conditions and explains how neuromuscular dentistry employs ULF-TENS to relax all masticatory and facial muscles and modulate the autonomic nervous system, thereby addressing both structural and physiological aspects of pain.12 A patient’s physiologic occlusion can be confirmed with additional objective data and diagnostic modalities such as electromyographic (EMG) clench tests, sonography, and computerized jaw tracking.13
Cooper’s 2004 study, published in the Journal of Craniomandibular Practice, provides valuable insight into the parameters that dentists utilize in assessing patients’ masticatory systems with bioelectronic instruments.14 Despite the availability of these instruments for well over 30 years, there has been minimal guidance published on physiological norms. According to the survey administered to an international group of dentists, parameters for electromyographic rest and clench values, and mandibular tracking were quite consistent.15 This consensus may serve as an important guide in the evaluation and treatment of patients with temporomandibular disorders and orthodontic issues. See Figure 4.
Dental orthotics that are based on electromyographic data can establish neuromuscular balance, reducing cranio-cervical pain by reducing muscular hypertonicity.16 The positioning of mandibular condyles can significantly affect masticatory muscle activity. Studies show when mandibular condyles are placed in a neuromuscular position, the efficiency of masticatory muscle recruitment during clenching is the greatest.17,18 Consequently, any therapeutic approach should aim to improve muscle function by ensuring proper condylar positioning as a first step.19 Appliances designed to maintain the mandible at its most physiological position can alleviate TMD symptoms. This strategy has been found to reduce headaches and other TMD-related pain significantly.20,21
In harmony with the current research on mandibular orthotic appliances, Michelle’s symptoms were relieved within 90 days (about 3 months) of treatment with a 3 segmented Myoaligner orthotic covering the entire lower arch. Visible improvements began with the return of facial symmetry, alignment of the head and neck, and an improved smile. See Figure 5.
.jpg)
Malocclusion can lead to descending compensation, starting with altered jaw position and tension in the head and neck muscles, progressing to compensatory curves in the spine, and eventually causing pelvic tilt and leg length discrepancies.22 Conversely, ascending compensation begins with a short leg or tilted pelvis, resulting in pelvic tilt, spinal curvature to balance the tilt, and further extending to neck and head adjustments, potentially causing malocclusion. Both patterns demonstrate the body’s interconnected compensatory mechanisms, affecting posture and leading to musculoskeletal pain.23,24 Addressing posture during the orthotic phase of treatment is crucial for maintaining overall balance and stability. Specific muscles that connect the hips to the spine, such as the iliopsoas (the strongest flexor of the hip) and quadratus lumborum (lateral flexion of vertebral column with ipsilateral contraction), play critical roles in maintaining proper alignment. Trigger points in these muscles can lead to referred pain patterns that affect the cranial region and lead to myofascial pain and dysfunction as outlined by Drs. Travell and Simons.25
Cooper and Kleinberg in 2008 showed that transitioning to a neuromuscular-based occlusion can significantly reduce or eliminate symptoms of Temporomandibular Disorders (TMD).26 A removable mandibular orthotic appliance that could continuously be worn by the patient was used to stabilize the mandible in its physiological position. After three months of full-time appliance usage, the new therapeutic positions remained intact and were associated with improved masticatory muscle activities. Furthermore, patients reported an overwhelming relief of symptoms, including reduction of headaches and other pain symptoms. See the sequence illustrated in Figure 6.
_a_pathologic_bite__b)_neuromuscular_bite_registration__c)_physiologic_myoaligner__d)_re.jpg)
In Michele’s case Myoaligner segmented orthotics served the patient as an invaluable tool in finding relief in a noninvasive and functional manner, as well as setting the stage for predictable results in phase two orthodontics and/or restorative treatments. By stabilizing optimal jaw alignment before teeth movement, neuromuscular orthotics secure the "myocentric position" for successful and predictable orthodontic treatment. The segmented design of the Myoaligner® allows for its use during palatal expansion, but currently, no other removable TMD device can offer that flexibility.
Michelle, wore her Myoaligner during the day while she underwent orthodontic expansion treatment with an upper DNA device provided by VIVOS Therapeutics, Inc. Michelle’s orthodontic expansion treatment was provided by my practice associate, Dr. Terry Lynn Tennant. See Figure 7.
_pretreatment__b)_after_8_months_of_treatment.jpg)
The Myoaligner® device was used in each phase of Michelle’s complex occlusion and airway treatment. In phase one, it was used on the lower arch to establish a stable physiologic occlusion, guiding the mandible to open and close on the most physiologic trajectory. Such protocols in phase one orthotic therapy may potentially contribute to bio-remodeling of the TM joins,27 reprogramming muscle memory, as well as much needed pain relief.
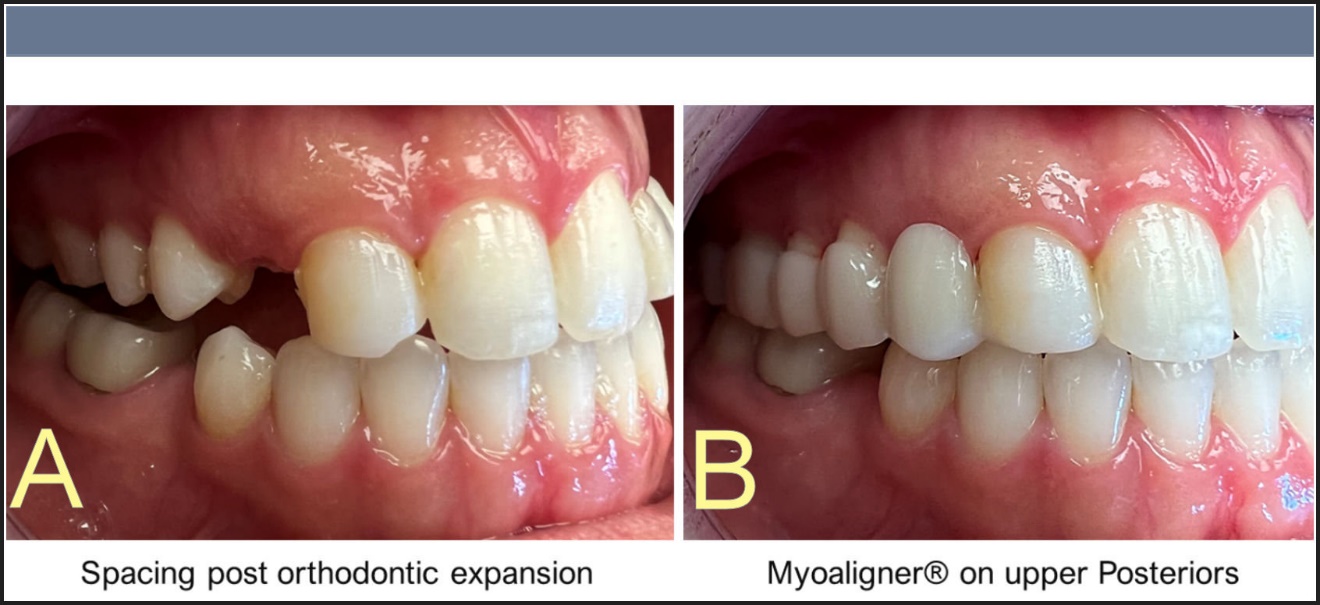
During her orthotropic phase two of the treatment, Myoaligner was used on the lower arch day and night to stabilize the muscles and joints while expansion occurred at night with an upper DNA device. The daytime orthosis facilitated the cross bite jump on the left side by allowing alterations to the device as needed to free up space for tooth movement. Upon completion of orthodontic treatment with Invisalign Clear aligners, during phase three of treatment, a new Myoaligner device was introduced to the upper posterior segments of the arch, to provide a transitional aesthetic solution for the spaces that had formed during expansion as well as stabilizing the occlusion. See Figure 8. This method paved the way for final implants and restorative phase.
_post_orthodontic_expansion_b)_upper_posterior_myoaligner__filling_spaces___stabilizing_.jpeg)
The modular and segmented design of Myoaligner device provides the practitioner with another option that sets it apart from the traditional full-arch devices. This proprietary design enables Myoaligner® to be used on any segment of the upper or lower dental arch, providing support precisely where it is needed. The pioneering use of 3D algorithms in the creation of these versatile anatomical devices for the upper and lower arches combined with the physiologic treatment protocol allows for maximum accuracy and enables the device to be fitted over non-prepared teeth, eliminating the need for enamel alterations.
Additionally, the segmented design is expected to allow for the flexion of cranial bones during function for a more natural function; a feature that will be tested with future studies. With Myoaligner, the provider can expect unprecedented flexibility in treatment plans, enhancing patient comfort and optimizing outcomes.
It’s important to note that Myoaligner is backed by over five decades of research supporting the science of neuromuscular dentistry and anatomical orthotics. This extensive body of research validates the effectiveness of stabilizing the optimal mandibular posture during swallowing function, leading to improved patient outcomes and long-term success. Imagine the applications in sports science.
Consider the following research: Mouthguards designed using neuromuscular dentistry principles have been found to have positive effects on muscular endurance and anaerobic power. Their usage suggests potential benefits not only in TMD patients but also in sports science for performance enhancement.28,29 Alterations in the vertical dimension of occlusion and mandibular position have been found to impact isometric strength and postural stability. Appropriate corrections can lead to improvements in cervical flexor strength and overall stability.30,31
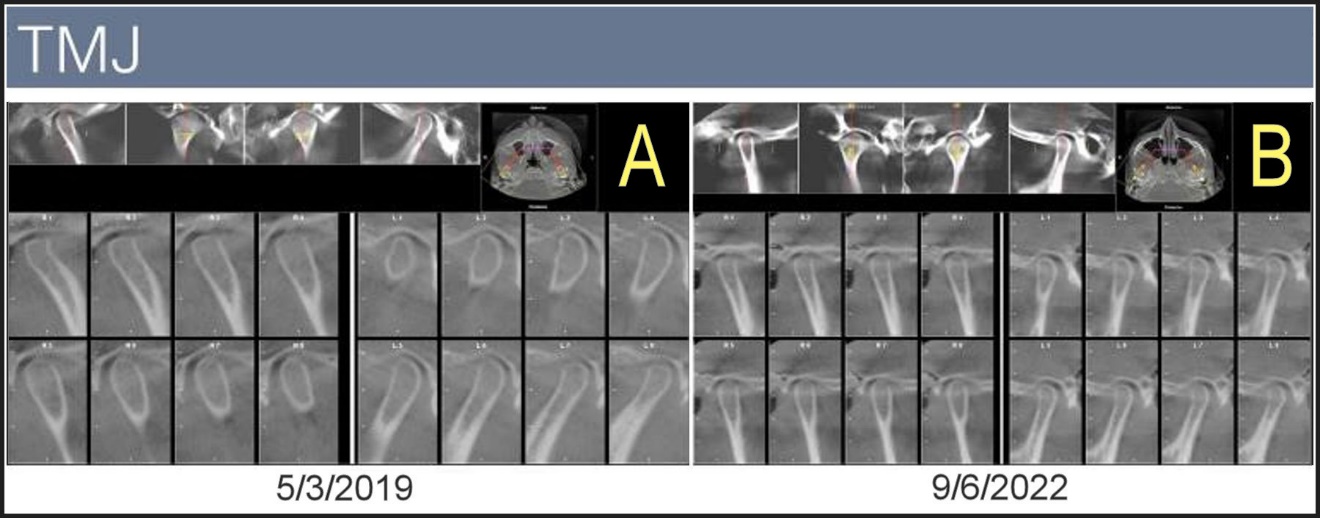
Clearly Michelle’s symptoms improved subjectively as reported by the patient, and objectively using data. With orthotropic and orthodontic treatments, we were able to alleviate life altering symptoms and improve not only her TMJ function and facial symmetry but her airway symptoms as well. The patient states her favorite part was no surgery, no pain, and minimal interruption of her daily life. Moreover, these anatomical orthotics not only provide a temporary stable occlusion, but also support the optimal position of the TM joints day and night. See Figure 9.
_pretreatment_images_of_the_tmjs__b)_improved_tm_joint_anatomy_after_3.3_years_of_treatm.jpeg)
The study by Vânia Cristina Pintaudi Amorim et al. examined how prosthetic rehabilitation affects condylar position in 12 women without temporomandibular disorders. Before and after fitting new maxillary complete dentures and mandibular removable partial dentures (RPDs), tomographic evaluations showed significant reductions in the previous distalization of condylar positions, indicating that altering occlusion through prosthetic rehabilitation can notably change condylar positioning.32
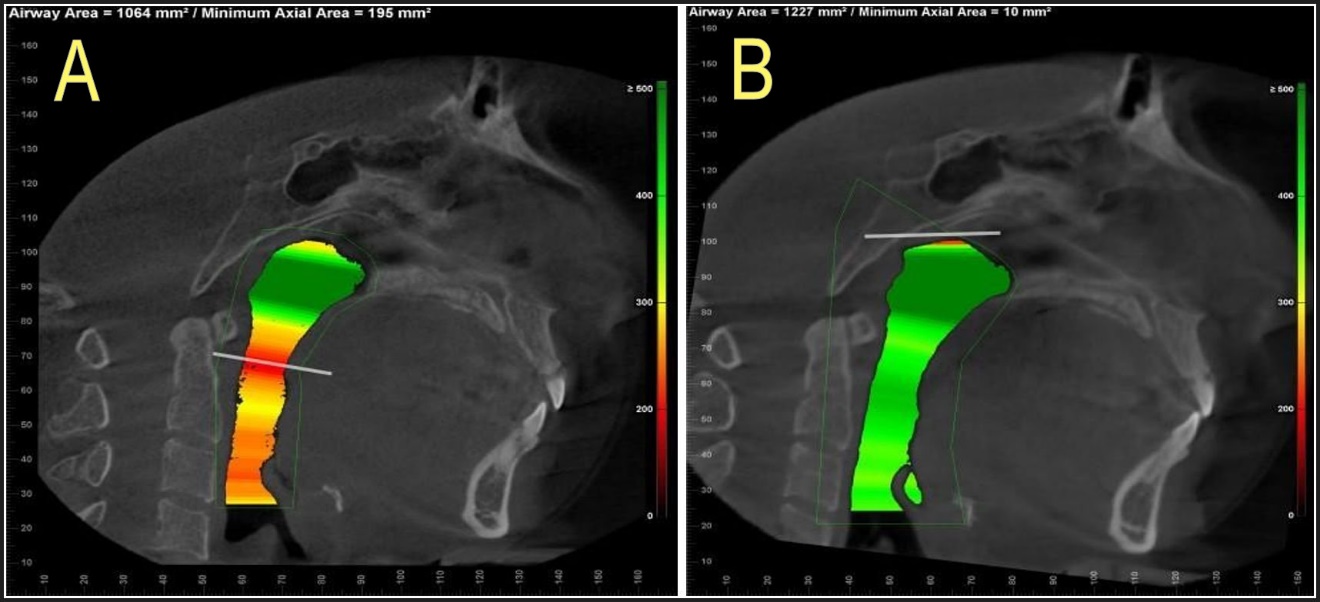
The CBCT scans before and after treatment show the intrusion of the mandible in the airway due to Michelle’s TMD before treatment. With Myoaligner® and her additional therapies in what could have been 18 months long treatment (treatment interruption by COVID), she had a dramatic improvement in airway volume. See Figure 10.

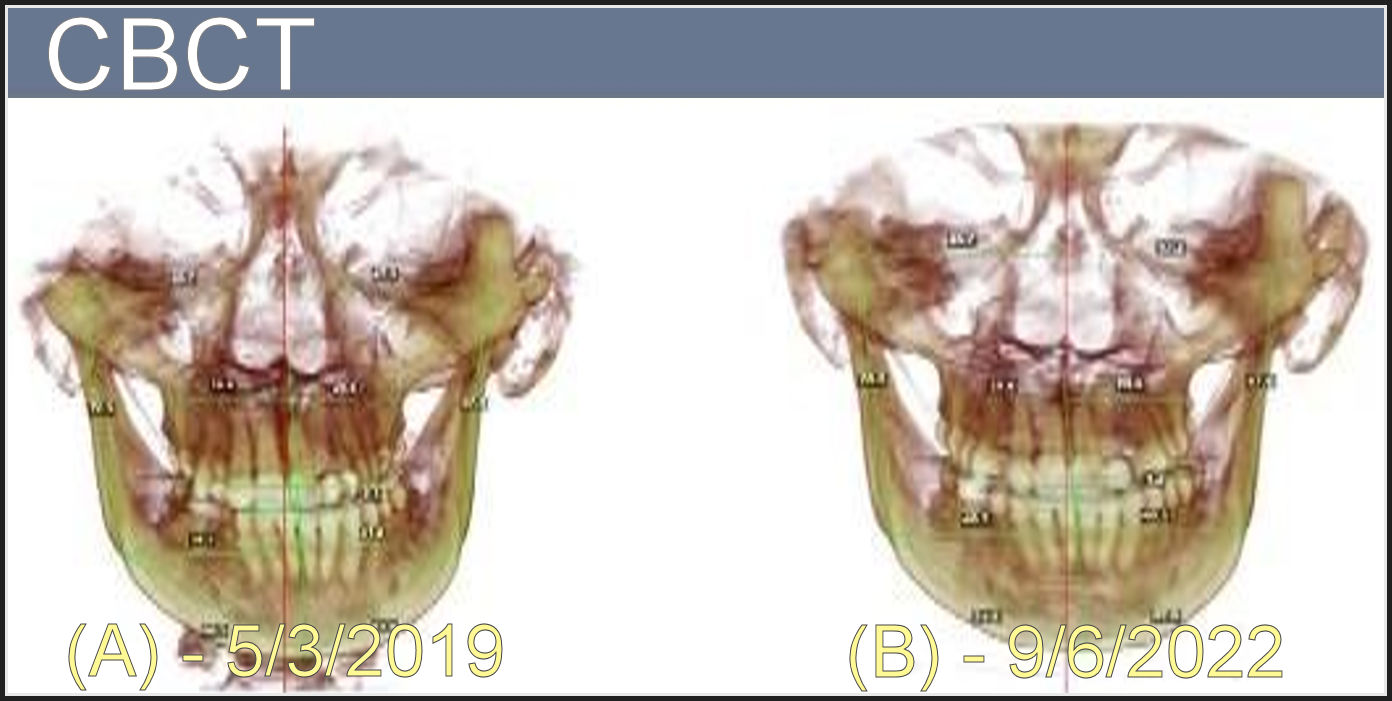
Note the dramatic movement of the impacted canine tooth that made it to the oral cavity by the end of palatal expansion treatment in this adult patient, further supporting the bone remodeling that takes place with biomimetic oral devices. See Figure 11. The panoramic x-rays also reveal dramatic improvements in the individual tooth alignments. See Figure 12.
_and_post_(b)_expansions_with_cbct_images.jpg)

By addressing both the functional and physiological aspects of TMD, the Myoaligner system enables you to deliver comprehensive care that goes beyond symptom management. Your patients can experience the transformative benefits of a treatment approach that considers the intricate interplay between jaw function, sleep quality, and overall health before they commit to long term non-reversible treatment options.
In my view, the Myoaligner system can offer your patients a treatment modality that aligns with established scientific principles and has a solid foundation in dental research. The integration of this methodology into your practice can help you elevate the level of care you provide, position you as a leader in the fields of Occlusion and TMD treatments once you see and report your results utilizing low liability and minimally invasive procedures. The segmented, modular design is meant to offer flexibility in treatment planning and provide space for correct tongue posture. Consider the value of its applications in complex implant or phased restorative cases!
In contrast to traditional full-arch appliances, Myoaligner’s segmented design offers a smaller occlusal table due to its unique design and multiple lines of draw per arch. This feature allows for a more precise fit, improved centric occlusal contacts, elimination of occlusal interferences, and optimal alignment of the jaw, while also creating additional space for the correct positioning of the tongue. Whether you follow a specific treatment philosophy or prefer a more flexible approach, Myoaligner can seamlessly integrate into your protocols, and provide a customized and effective treatment experience for your patients.
As dental professionals, our primary focus is providing the highest standard of care to our patients. Myoaligner empowers dentists to achieve this goal by offering a comprehensive, scientifically supported, and patient-centered solution for TMD and complex occlusal treatments with less risk.
CONCLUSION
Myoaligner is not just a device; it’s a comprehensive physiologic solution that caters to the diverse needs of patients. It opens a world of possibilities for restorative solutions, providing patients with a range of treatment options to suit their individual needs by giving results both subjective and objective, prior to initiation of irreversible treatments in dentistry. With the advancements in dental technology and 3D manufacturing, gone are the days of limiting orthotic devices to bulky, semi-anatomical devices that are often limited to nighttime wear.
DISCLOSURE
Dr. Maryam Motlagh, DMD, MICCMO is the inventor of the Myoaligner® and CEO, MyoHealth Technologies, Inc., Portland, OR USA. drm@myoaligner.com
FUNDING
No funding was received from any source for this project.