




INTRODUCTION
Human limb movements are successfully modeled based on the assumption that the central nervous system controls the movements by attempting to maximize movement smoothness. Chewing smoothness can be characterized by the mean number of transitions between acceleration and deceleration within a sequence of cycles. Jerk is defined as the rate of change in acceleration.1 It is the third derivative of movement after velocity and acceleration (in calculus Jerk = d3x/dt3) and it can be useful in measuring the jerkiness or inversely, the smoothness of a chewing motion.
At every change from acceleration to deceleration or vice versa, the Jerk function produces a peak. By simply counting the number of peaks in the Jerk function of a sequence and dividing by the number of cycles in the sequence, an objective measure of the amount of jerkiness within a chewing movement sequence can be calculated. Smoothness is a characteristic of good function and jerkiness is a characteristic of dysfunction. However, jerkiness also varies with velocity and acceleration. When reviewing this parameter, a smaller number indicates smoother function and a larger number is associated with dysfunction.
It has been determined that the smoothness of head movements is strongly related to the movement’s velocity, where fast movements are smooth and slow movements are jerky, with large amplitude movements being less smooth than smaller amplitude movements.2 The degrees of Jerkiness during chewing function have been studied in children and adults, with children showing generally more jerk cost.3
Jerkiness during chewing can be assessed either 3-Dimensional Jaw Tracking,3 or with a tri-axial piezoelectric accelerometer being attached to the skin of the mentum.4 The effect of tooth contacts on chewing Jerkiness has been studied as well, whereby differing experimental occlusal inter-ferences were introduced on both the non-working and working sides,5,6 and when single molar crowns of different anatomical cuspal forms were placed on maxillary and mandibular molars.7,8 One study revealed that introduced occlusal interferences induced a remarkable increase in the normalized jerk-cost (NJC), prolonged the duration of the decelerative phase, and lowered the peak velocity for jaw closing movements during chewing.6 It has been demonstrated that the placement of an anatomical crown produced less variability and jerk-cost compared to a flat occlusal crown.8 Additionally, the smoothness of the masticatory movements was improved more in subjects who received crowns on their mandibular molars, rather than those on their maxillary molar (regardless of anatomical crown form), although this study included a limited number of only 14 subjects.9
Normal mastication is a smoothly coordinated sequence of events with significant lateral movement.10 A previously described method for studying human mandibular motion in three planes of motion used magnet-based mandibular incisor point tracking referred to as Mandibular Kinesiography (MKG)11 or Electrognathography (EGN).12 When recording with EGN, subjects wear a headset that houses eight bilateral mandibular movement sensors, which record the movement that a magnet makes when anchored to the mandibular incisors as subjects unilaterally chew gum. It has been shown definitively that EGN recordings are measurably altered in the presence of masticatory dysfunction.13,14
The concept of Immediate Complete Anterior Guidance Development (ICAGD) has been described previously.15 A recent publication utilized this computer-guided occlusal adjustment method, with simultaneous electro-myography data capture of the masseter and temporalis muscle activity levels that occurred during unilateral gum chewing.16 The authors measured changes in the Average Chewing Pattern (ACP) in 29 muscularly dysfunctional TMD patients, from before to after the subjects underwent the measured, computer-guided occlusal adjustment procedure ICAGD coronoplasty. The authors reported that the subject group’s Average Chewing Pattern (ACP) shape, consistency, muscular coordination, speed, and vertical dimension were all significantly improved within one week’s time after undergoing ICAGD. The computer-measured and guided occlusal adjustments quickly and physiologically improved group chewing, without requiring the patients to wear pre- or post-treatment appliances, or being given any chewing training or instructions.16
ICAGD currently requires the T-Scan 10 computerized occlusal analysis system (Tekscan, Inc. S. Boston, MA, USA), be synchronized simultaneously with the BioPAK/BioEMG III electromyography system (Bioresearch Associates, Inc. Milwaukee, WI, USA). ICAGD is a computer guided, lateral excursion focused occlusal adjustment procedure. Its objective is to shorten the time of prolonged excursive posterior tooth contacts that occur during excursive movements by reducing opposing posterior occlusal surface contact friction (known as the posterior Disclusion Time Reduction).17 ICAGD is performed from the maximum intercuspal position (MIP), and has specific numerical timing and force distribution endpoints that objectively quantify that correct post treatment results were achieved during the rendered treatment.17,18 It is a very different occlusal adjustment procedure from traditional occlusal equilibration,19 since no CR mandibular manipulation is required or performed, and the CR-CO discrepancy is not treated in any part of the adjustment procedure.17,19 Since 1991, multiple published studies using the T-Scan computerized occlusal analysis system and the ICAGD measurement-driven occlusal adjustment procedure, have shown that rapid and lasting dysfunctional muscular symptom resolution can be accomplished.17,20–29
The results of the gum chewing study that utilized ICAGD with 3-Dimensional jaw tracking of the Average Chewing Pattern (ACP) were definitive, in that many differing statistically significant chewing parameter improvements were obtained shortly following ICAGD.16 However, Jerkiness of the subjects’ chewing function before and after ICAGD was not computed, or included in the results of that study.16
Specific Aims
To test the effects of (ICAGD) on the smooth-ness, the timing, and the velocity of gum chewing, within a group of patients diagnosed with occluso-muscle dysfunction (OMD).
Materials and Method
The pre and post treatment gum-chewing jaw motion records and EMG data sets of 29 muscularly dysfunctional OMD patients from the previous study group16 were selected for additional analysis. The included subjects all demonstrated chewing fatigue, chewing pain, or chewing weakness, and experienced ongoing head, neck and facial pain, headaches around the eyes, midface and temples, jaw tension, previous unsuccessful splint use, chronic pain medication ingestion, and/or mildly painful temporo-mandibular joints. All included subjects were required to have anterior teeth that coupled or nearly coupled. Excluded subjects demonstrated TM joint locking, disc displacement without reduction, bone-to-bone condyle to skull base contact, or reported a prior history of condylar injury or avascular necrosis.
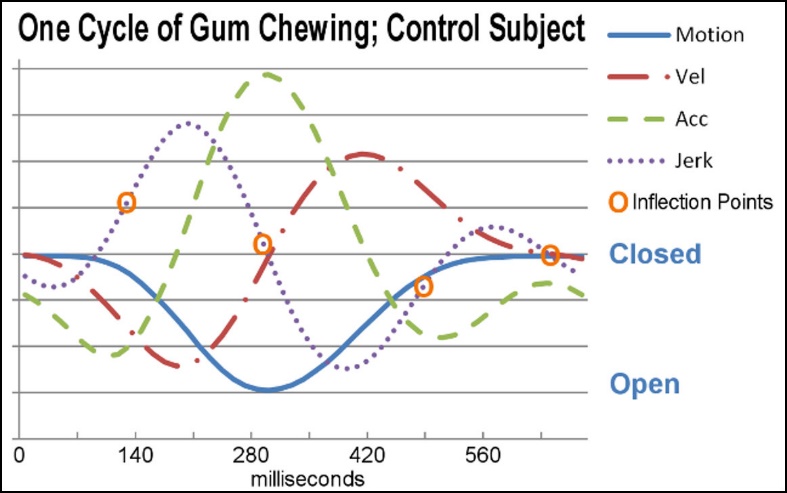
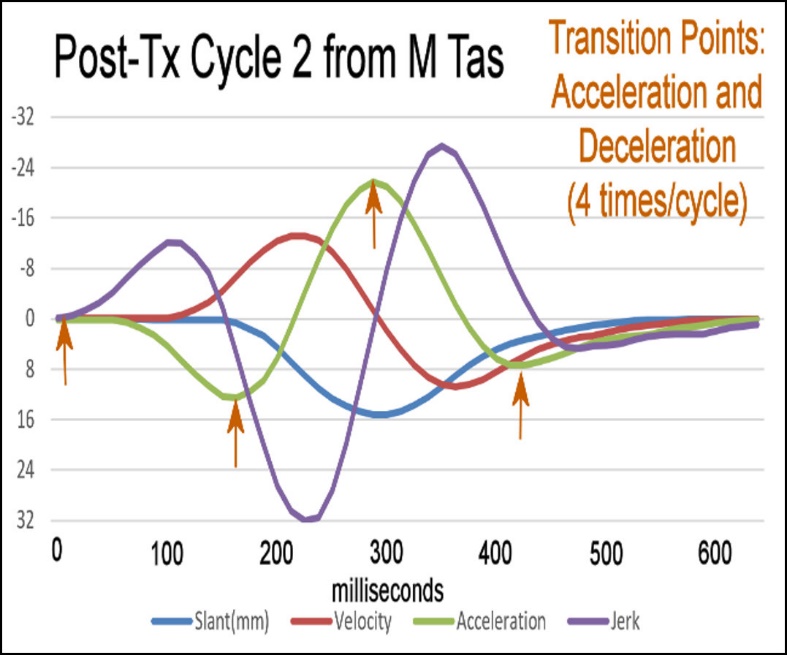
The same pre-ICAGD and post-ICAGD chewing data obtained from the 29 selected subjects in the prior Average Chewing Pattern (ACP) study16 were further analyzed to calculate their Jerk functions, cycle times, and velocities. The third derivative of motion (Jerk d3x/dt3) was calculated from the movement data for each subject’s pre and post ICAGD treatment chewing sequences. These included 15 cycles of chewing gum first on the left side, followed by 15 cycles of chewing gum on the right side. The calculation of Jerk was used to determine the number of transitions between acceleration and deceleration in each cycle. Each inflection point in the Jerk waveform represents such a transition. An ideally smooth cycle includes just 2 transitions in opening and an equal number in closing for a total of 4 inflection points/cycle. See Figure 1.
_subject_with_good_occlusion__a_normal_.jpeg)
Mean velocities and cycle times were calculated from each subject’s left and right chewing data prior to their ICAGD treatment, and separately from their comparable post ICAGD data (n = 58). The Wilcoxon Signed-Rank Test compared; 1.) the pre-treatment mean number of Jerk inflection points to the post-treatment mean number, 2.) the pretreatment cycle times to the post-treatment cycle times, (See Figure 3) and 3.) the pretreatment velocities to the post-treatment velocities. See Figure 4. The Wilcoxon Signed-Rank Test statistic was employed instead of the Student’s t test because the analyzed data did not fit a normal distribution, which is one of the requirements for applying the Student’s t test. (Alpha selected was 0.05)



This study followed the World Medical Associations Declaration of Helsinki in 1964 and its later amendments, for comparable ethical standards regarding the use of Ethical Principles for Medical Research Involving Human Subjects. All subjects were fully informed of the risks and benefits of ICAGD, and consent was obtained from all individual participants included in the study. The protocol for the original study was approved by the institutional review board at BioResearch Associates, Inc., Milwaukee, WI, USA (BIRB/90Z/2014).
Assessing Smoothness
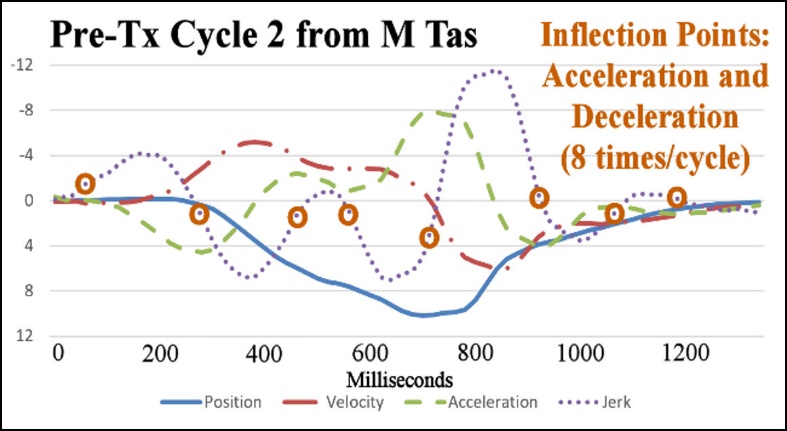
To assess the smoothness of a chewing cycle, it is necessary to identify the number of inflection points within the Jerk function, which indicates the number of transitions between acceleration and deceleration. In a normal control subject (Figure 1), the minimum number of inflection-points possible is two in opening (one for the acceleration and one for the deceleration), and likewise, two more inflection points in closing. When there are more than two inflection points in a half-cycle, it means that too many alternating accelerations and decelerations are occurring. Alternatively, Figure 2 shows a dysfunctional subject’s jerkiness with 8 inflection points present in one cycle, which is significantly more than in an ideal normal subject’s cycles.
Results
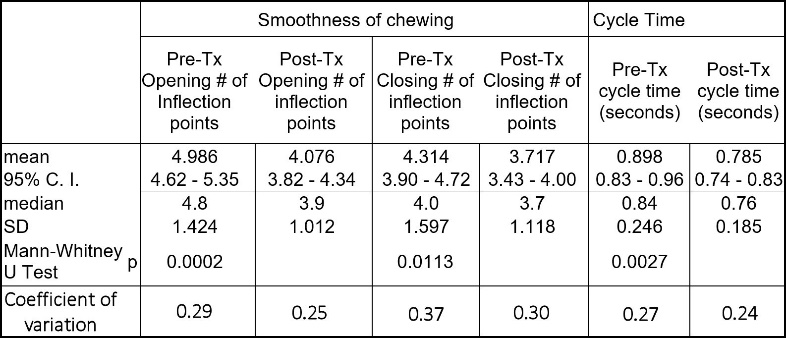
An eighteen percent reduction in the mean number of Jerk inflection points during opening was calculated after ICAGD (p = 0.00001). A fourteen percent reduction in the mean number of Jerk inflection points during closing (p = 0.00001) were found after the ICAGD occlusal adjustment. See Figure 3. The coefficient of variation was calculated with respect to the pre-treatment inflection points and the post treatment inflection points. In both cases the coefficients were reduced, inferring a reduction in the variability from cycle to cycle. This is one more indication of improved function.
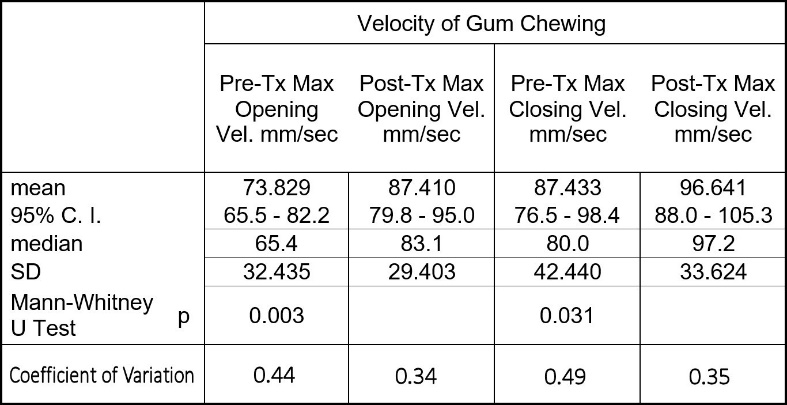
The mean cycle time of the group was reduced from 898 milliseconds to 785 milliseconds (p = 0.00001), which is close to the mean normal cycle time of 760 (+/-114) milliseconds.13 (Table 1). Again, the coefficient of variation was calculated and it was reduced after treatment. The mean opening velocity of chewing for the group increased from 74 mm/second to 87 mm/second, approaching the mean normal opening gum-chewing velocity of 110 (+/- 39) mm/second (p = 0.00001).13 The mean closing velocity increased from 87 mm/second to 96 mm/second, approaching the mean value of normal. See Figure 4.
Discussion
The results of this follow-on investigation indicate that the chewing jerkiness observed in the subjects improved significantly within one week after the subjects’ pre - ICAGD prolonged excursive Disclusion Times were shortened to < 0.5 seconds by ICAGD. For the group as a whole, there were significant reductions in the numbers of inflection points, both in the opening and in the closing portions of the cycles. The concurrent decreases in the chewing cycle times suggest improvement when considered with previous studies of normal cycle times.13 See Figure 4. Also, the increases in the mean opening and closing velocities suggest improved function as well.13 Also in Figure 4. Variability increases in the presence of dysfunction.13 The reduction in all of the coefficients of variation was another indication of improved function.
These results directly support the findings of the earlier Average Chewing Pattern (ACP) study,16 in that the jerkiness improvement observed mirrored the improvements seen in the same subject group’s many ACP parameters. Further, these results support the findings of previously published Disclusion Time reduction/ICAGD studies, where chewing improvements accompanied the reduction of many chronic muscular OMD symptoms.17,20–29
The results of this study also indirectly corroborate the findings of Yashiro et al., who found that introducing occlusal interferences worsened the jerkiness of chewing.6 ICAGD lessened the time the excursive movement surface friction occurred between opposing posterior tooth contacts, such that closure stops are left untouched during ICAGD, and minimal duration excursive tooth contacts remain.15 The entire ICAGD procedure is focused on removing all lateral occlusal interferences, from both the working and non-working sides up to and including the premolar teeth.15 So, instead of worsening jerkiness with additional interferences like Yashiro did,6 ICAGD removed all the existing prolonged duration interferences. The reduced jerkiness resulted from the lack of opposing excursive occlusal surface contacts, which were no longer present along the excursive pathways within the chewing motion pattern. This allowed the subjects to make freer entry into and out of occlusion, without having to muscularly avoid interfering occlusal contacts, which significantly improved the subjects’ chewing smoothness.
Figures 2 and 5 illustrate the changes in jerkiness and the difference in the smoothness between jerky (Figure 2) and not jerky chewing (Figure 5) brought about by the ICAGD coronoplasty in the same subject. Note how there are markedly fewer inflection points are visible after ICAGD (Figure 5). With a lack of noxious occlusal contacts occurring during the chewing movement, smoother motion patterns developed within just 7 days. Based on previous ICAGD studies, it is expected that improvements should continue for at least several months. Although the statistics stated in the Results and compiled in Figures 3 and 4 are all based the average of 30 chewing cycles per subject (15 Left and 15 Right), the single cycles shown graphically in Figures 2 and 5 are representative examples of the clear difference between the dysfunctional level of jerkiness and a normal level of jerkiness.
__after_icagd_treatment_demonstrating_a_normalize.jpeg)
Specifically, for this subject (M Tas) the pre-ICAGD mean chewing cycle time was 1.235 seconds (very slow), where mean normal is 0.760 (+/- 114)13 seconds. Post ICAGD, the mean chewing cycle was reduced to 0.905 seconds, which is marginally normal. The subject’s opening jerkiness was reduced from 6.0 to 3.7 after ICAGD (again marginally normal, 2.0 is perfectly smooth). And the post-ICAGD, closing jerk reduced from 6.4 to 3.6 (WNL). Normal asymptomatic subjects chewing gum usually present with jerkiness values between 2.0 - 3.5.
Additionally, post-ICAGD, the size of the chewing cycle increased from approximately 11 mm pre-ICAGD to almost 16 mm post-ICAGD at the Turning Point (the most open position, where the transition from opening to closing occurs within ae chewing stroke). This almost 16 mm chewing cycle size is near to the normal population mean chewing size value, for the chewing of one stick of gum.13 Furthermore, the opening velocity increased from 32 mm/second to 72 mm/second and the closing mean velocity increased from 45 mm/second to 73 mm/second. Both the increased size of the ACP and the increased velocity of chewing gum are common indications that chewing function has improved. Lastly, in the pre-ICAGD graph (Figure 2), in cycle 2 there are 8 transitions between acceleration and deceleration, which constitutes a very jerky motion pattern. However, in the post-ICAGD jerk graph in cycle 2 (Figure 3), there are only 4 transitions between acceleration and deceleration. Four transitions are the minimum number possible, and is considered the ideal smoothness for chewing function.
The pretreatment MIP occlusion is illustrated in Figure 6A, while Figures 6B and 6C show the right and left excursive relationships of the dentition. There is visible, bilateral posterior group function present in both excursions. Also note there were many abfracted teeth from the poor vertical tooth orientation. The severe tooth tipping and the worn guidance angles on both canines, depict the years of prolonged excursive friction that have been present in this subject’s excursive movements and chewing motions.

**__with_rig.jpeg)
**__with_l.jpeg)
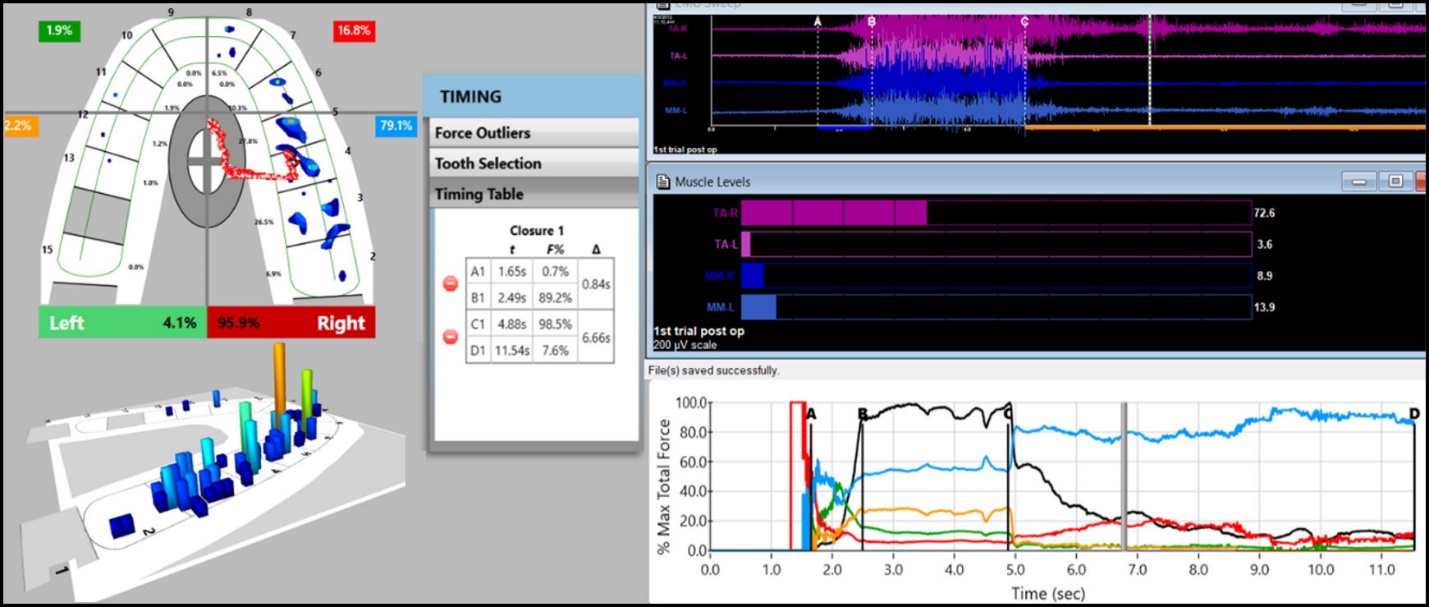
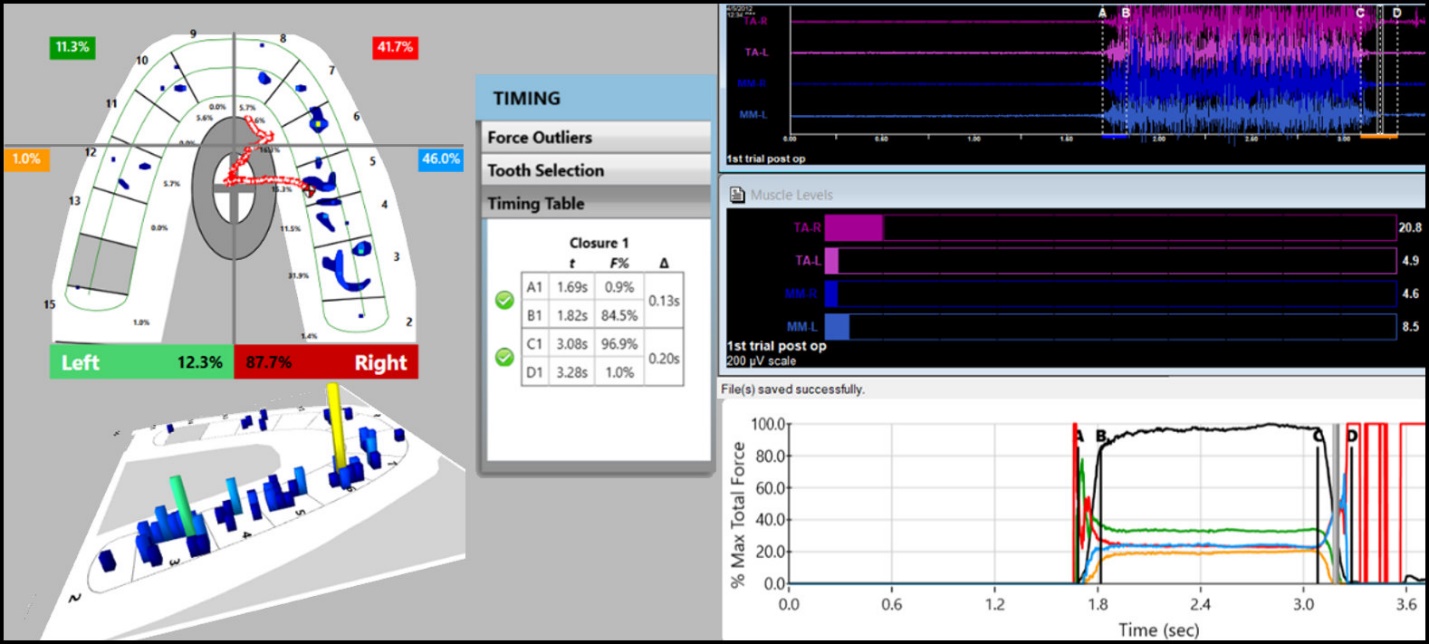
Of importance is that prior to ICAGD, subject M Tas’ Temporalis and Masseter muscle physiology demonstrated very high excursive muscle activity levels (Figure 7A; to the right of line C in the upper EMG pane). But after ICAGD the Temporalis and Masseter muscle physiology demonstrated markedly less excursive hyperactivity (Figure 7B; to the right of line C in the upper EMG pane). This reduction in excursive hyperactivity is the therapeutic effect that Disclusion Time Reduction creates physiologically, from within the patient’s Central Nervous System (CNS).25,30 With lessened hyperactivity, there is increased oxygenation from far less contractions metabolizing excess lactic acid buildup. The muscles then function excursively much closer to their baseline contraction levels required for chewing (Figure 7B), absent of excess contractions brought on by the prolonged duration frictional tooth contacts. This lessened excursive masticatory muscle hyperactivity, is what led to this subject’s smoother chewing cycles, as well as physiologically improving the entire subject group’s chewing smoothness.


The effect of ICAGD on chewing does not reduce the force that the muscles apply. In fact, very often the amount of force applied to the bolus increases, but the durations of the muscle contractions are reduced such that the overall muscular effort is reduced. In some cases, the largest reduction in activity occurs within the non-working side muscles that are supposed to be resting during chewing.
Figures 8A shows the pre-ICAGD friction present on the maxillary left 2nd premolar, that occurred in the right excursive (balancing side) movement. The v-shaped linear articulating paper marking represents the occlusal surface drag and friction that resulted when the palatal cusp of tooth #13 rubbed excursively against tooth #20, below.

Figure 8B shows a mid-ICAGD correction to the friction, has changed the markings to be more point contacts. There is late 1st premolar (#12) left working side guidance contact remaining, along with canine guidance ink markings visible on tooth #11’s incisal edge.
**_at_mid-icagd_correction_of_the_posterior_c.jpeg)
Limitations
As this is a follow-on study from a previous research project, no new data was gathered or employed. However, the 29 included subjects in the prior study generated a total of 1740 chewing cycles,16 which were analyzed for changes in jerkiness, cycle time and velocity from pre to post-ICAGD treatment. So that analyzed data was substantial, despite the fact that no new chewing data was obtained from the subjects.
A 2nd limitation was that for this group of re-analyzed subjects, some changed their chewing parameters on one side only, or changed only a small amount, while the group as a whole changed very significantly towards measured chewing improvements. See the p values in Figures 3 & 4. This may have occurred because some subjects may have had only one chewing side affected by prolonged interfering contacts, or had some minor, unilateral structural TM Joint issues that would have limited their bilateral improvements. However, all subjects were included in the computations and both the left and right sides were used within the tests. Although ICAGD treatment did not make all the subjects perfect or ideal bilateral chewers, their measured improvements were enough to return many subjects back to within their natural adaptive range, which ameliorated most of their symptoms.
A 3rd limitation was that subjects were their own controls and not statistically compared to any “Control group,” except where population norms were available. As this specific study attempted to determine a measured treatment effect (changes in the jerk, cycle timing, and velocity after ICAGD), using the subjects as their own controls was the most accurate statistical approach.
CONCLUSION
Within this group of muscularly dysfunctional subjects, the therapeutic effects of Immediate Complete Anterior Guidance Development (ICAGD) allowed these subjects to chew gum significantly faster and smoother. Following ICAGD, there was reduced masticatory muscular hyperactivity, and markedly lessened time-durations of noxious opposing frictional excursive occlusal contacts present within the chewing pathways. This allowed the subjects to chew faster, smoother and with less variability in just 7 days. These results strongly indicate that within one week following ICAGD, the group as a whole changed very significantly, improving their ability to chew gum significantly faster and smoother.
Conflicts Statement
The corresponding author (Robert B. Kerstein, DMD) is a Clinical Consultant for Tekscan, Inc., S. Boston, MA, USA, and has received an annual stipend from Tekscan. The second author (John Radke, MBA) is the Chairman of the Board of Directors for BioResearch Associates, Inc. Milwaukee, WI, USA, and receives an annual salary from them.
Acknowledgments
Tekscan, Inc. supplied T-Scan HD recording sensors for all occlusal analysis recording procedures. BioResearch Associates loaned a JT-3D jaw tracker (Electrognathograph) & BioEMG III electromyograph for all chewing function and muscle physiology recording procedures.
Funding Statement
No funding agency provided any monies in support of this research.