

INTRODUCTION
Temporomandibular Disorders (TMDs) are a collective that involves clinical problems associated with the muscles of mastication and the Temporomandibular Joint and associated structures.1 TMDs are known to have a high prevalence such that up to 75% of the population experience one or more signs of TMDs such as joint noises, pain on palpation, abnormal joint movements, or occlusal wear, while about 33% of the population exhibit at least one symptom associated with TMDs.2,3 However, those actually seeking treatment is much lower at about 5 to 7 %.3
Developing a robust diagnostic screening protocol for these common disorders has been challenging for dentistry. Researchers have proposed the Research Diagnostic Criteria for the clinical examination of TMD patients. However, validation studies demonstrated remarkably inadequate results.4 And the newly recommended Diagnostic Criteria (DC/TMD)5 also demonstrated poor sensitivity and/or specificity for clinical use, despite that it continues to be used for screening.6
Myofascial pain is one of the most common Temporomandibular Disorders, being a type of myalgia within the DC/TMD criteria.5 The etiology of myofascial pain is thought to be multifactorial including biological (e.g. occlusion, TMJ), behavioral (e.g. emotional, social), environmental, and cognitive.7,8 However, a 2024 systematic review by Lekaviciute et al., determined that occlusal factors are positively correlated with the development of TMDs. The authors specifically noted that occlusal factors play a role in bruxism, myofascial pain, arthralgia, and disc displacements.9
Removing posterior functional occlusal interferences and creating rapid (in time) anterior guidance control of excursive movements as a TMD treatment method has helped patients suffering from myofascial pain.10 Many studies have previously reported successful TMD treatment outcomes with computer guided occlusal adjustments.11–34 The Immediate Complete Anterior Guidance Development coronoplasty (ICAGD) is performed by occlusally adjusting the Disclusion Times of all premolars and all molars to less than 0.4 seconds per excursion, which has been shown effective in reducing myofascial pain.15–18 This therapy termed “Disclusion Time Reduction (DTR)” requires the T-Scan 10 (Tekscan, Inc., Norwood, MA, USA) synchronized to the BioEMG III electromyograph (BioResearch Associates, Milwaukee, WI, USA), to simultaneously record occlusal contact forces and the resultant muscle activity levels. Often DTR therapy can be accomplished solely with computer-guided ICAGD (reduction therapy). However, with cases that lack contacting anterior guidance surfaces, preliminarily bonding composite onto cuspids (additive therapy) is followed by ICAGD to clinically obtain specific, high-tolerance numerical occlusion parameter outcome measures (Occlusion Times ≤ 0 .2 secs.; Disclusion Times ≤ 0.4 secs.).11–34
OBJECTIVES
The objectives of this study were to test the efficacy of Disclusion Time Reduction (DTR) computer-guided occlusal therapy for accurately diagnosed Occluso-muscular Temporomandibular Disorders and 2) to determine the effects of DTR on the contractive functionality of the anterior temporalis and masseter muscles.
METHODS
Twenty-eight dentate patients suffering from myofascial pain were selected for this study after informed consent and ethical clearance were obtained. This clinical cohort study was conducted over several days at the Indian Dental Association Main Office in Mumbai, India, with one senior clinical advisor overseeing eight different dentists undergoing DTR clinical training. Included subjects who demonstrated significant Occluso-muscular symptoms were ICAGD/DTR-treated with the T-Scan 10/BioEMG III synchronization, which recorded subject occlusal contact forces and the associated muscle activities. See Figure 1. The pre and post treatment data from individual treated subjects was pooled together and analyzed as one treatment group.

Joint Vibration Analysis (BioJVA, Bioresearch Associates, Milwaukee, WI, USA) and CBCT imaging evaluated subject TM joint health, to rule out subjects with structurally compromised orthopedic conditions and to include solely patients with minimal intracapsular TMJ damage. Intraoral examinations ascertained that all included subjects were Angle’s class 1 anteriorly with contacting or nearly contacting anterior guidance surfaces, adequate mouth opening (> 40 mm), and limited occlusal wear.
Inclusion Criteria
-
Patients suffering from myofascial pain with a Class I anterior canine relationship.
-
Sufficient posterior intercuspation with limited occlusal wear.
-
JVA Total Integrals less than 80 KPaHz, with a mouth opening range > 40 mm.
-
Piper Classifications ranging from 1 through 3b.
Exclusion Criteria
-
Angle’s Class II and Class III anterior relationships with a lack of anterior contacting guidance surfaces, anterior open bite, and severe dental malocclusion
-
JVA Total Integrals greater than 80 KPaHz and/or with a mouth opening less of than 40 mm.
-
Severe occlusal wear
-
Structural deformities of the maxillofacial region and/or TMJs (Piper Classifications ranging from 3b – 5)
-
Subjects with a history of TMJ locking and/or previous surgery to recapture discs.
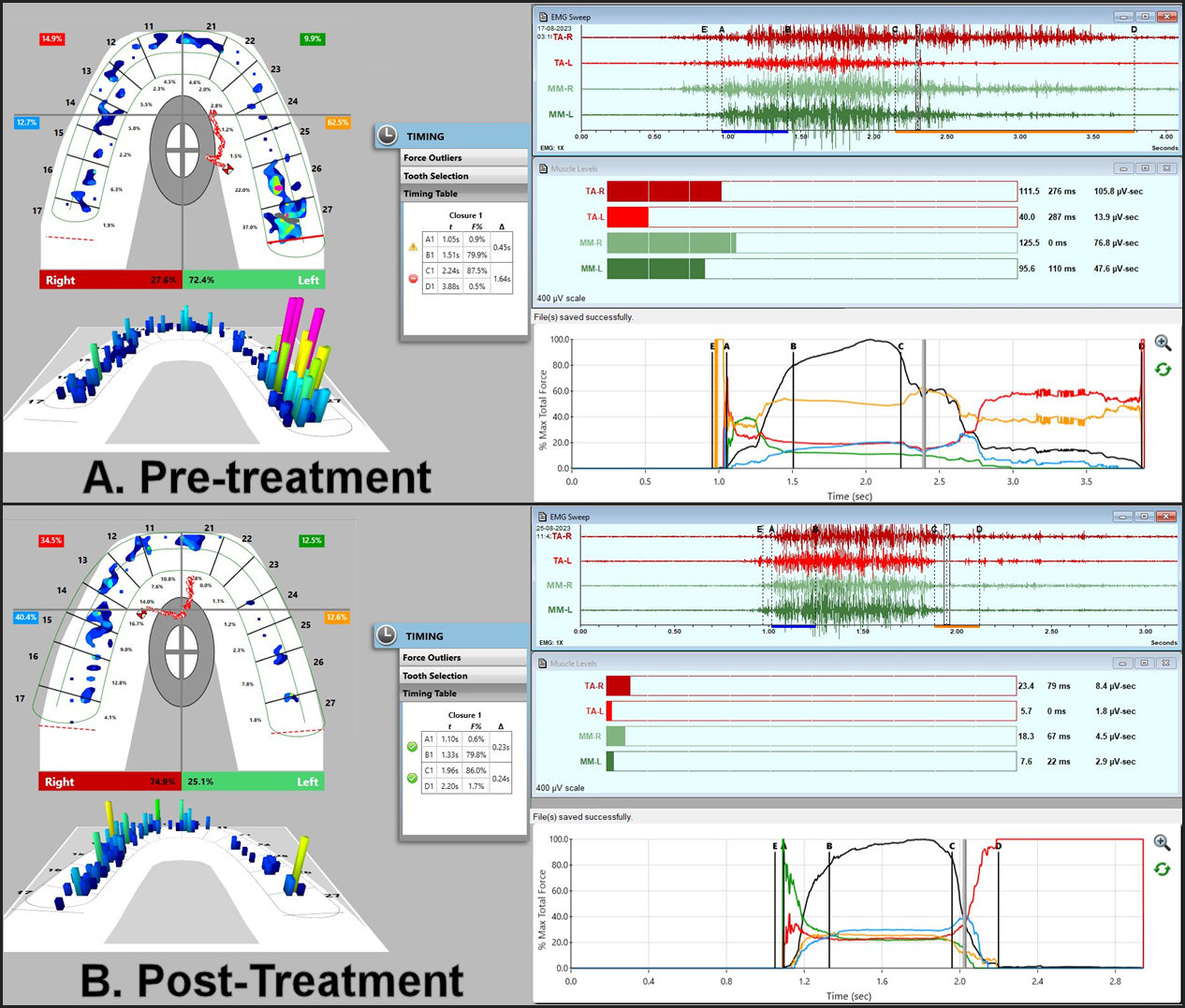
Two sets of pre ICAGD T-Scan 10/BioEMG recordings were made of subjects’ right and left lateral excursive movements to record their Occlusion Times and Disclusion Times, the muscle activity levels of the bilateral anterior temporalis and masseter muscles (see Figure 2), any COF Trajectory Mid-course Corrections, and the muscular effort expended from excursive commencement through to complete posterior disclusion. Once the ICAGD coronoplasty was deemed complete, identical post treatment recordings of the same occlusal parameters were obtained to compare to pretreatment. See Figures 3A, B.

**_t-scan_linked_to_bioemg_iii_displaying_a_right_lateral_excursion_pre-dtr._the_discl.jpg)
The compared functional Occlusal Parameters are defined below:
-
Occlusion Time (OT) - the amount of time required from first contact until all opposing contacting teeth reach static intercuspation (the A-B time duration in the T-Scan Force vs. Time graph, which precedes Maximum Intercuspation). A physiological OT ≤ 0.2 seconds).35
-
Disclusion Time (DT) - the amount of time duration during a lateral excursion when leaving MIP until posterior teeth are fully discluded from the anterior guidance (the C-D time duration in the T-Scan Force vs. Time graph). A physiologic DT ≤ 0.4 seconds.18
-
Mid-course Corrections - observed when the T-Scan Center-of Force icon starts excursively towards the molars, and midway through the excursion changes direction towards the cuspid, instead of following a straight movement towards the working side cuspid. Mid-course Corrections were treated statistically as a binomial distribution (0 = no kinks present in the COF trajectory progression; 1 = kinks were present in the COF trajectory progression).
-
Integrated EMG Muscle Activity Levels - indicates the muscular effort expended within an excursion during the C - D time duration within both the waveform EMG window and the T-Scan Force vs. Time graph. The individual muscles analyzed were the right temporalis (TA-R), the left temporalis (TA-L), the right masseter (MM-R) and the left masseter (MM-L).
-
Visual Analog Pain Scores – A subject self-reported ordinal number ranging from 0-10:
-
No Pain: 0
-
Mild Pain: 1-3
-
Moderate Pain: 4-5
-
Severe Pain: 6-7
-
Very Severe Pain: 8-9
-
Unbearable Pain: 10
After ICAGD occlusal adjustments were deemed complete, each subject self-reported their post DTR pain scores for comparison to their pretreatment scores.
Statistical Analysis
Statistical analyses were performed using the Wilcoxon Signed-Rank Test for intra-patient comparisons, which ignores all differences between subjects and does not require the data sets to be normally distributed. An alpha of p < 0.05 was chosen for significance.
The Null Hypothesis - No significant differences in the Occlusion Times, the Disclusion Times, the Mid-course Corrections, or the muscular effort expended within excursions will be observed from pre to post DTR therapy.
Alternate Hypothesis - Significant differences in the Occlusion Times, the Disclusion Times, the Mid-course Corrections, and/or the muscular effort expended within excursions will be observed from pre to post DTR therapy.
Description of the ICAGD coronoplasty
T-Scan 10/BioEMG III closure into MIP and excursive movement data was obtained prior to subjects undergoing ICAGD (Figure 3A), which is described here11–25: The 2 synchronized technologies recorded each subject’s occlusal force imbalances, their Occlusion and Disclusion Times, and any excursive COF midcourse corrections, and the effort expended during right and left excursions. Both the maxillary and mandibular teeth were air dried on one side of the mouth after which subjects closed into their Maximum Intercuspal Position (MIP) with 21-micron thick articulating paper (Accufilm II, Parkell Inc., Englewood, NY, USA) interposed between their posterior teeth. Then each subject moved into a right excursion all the way out to the tip of the right canine, then back into MIP, then moved outwards into a left excursion all the way out to the tip of the left canine, and then once again back into MIP. The pre-treatment T-Scan 10/BioEMG III recordings guided the clinician to adjust the frictionally engaged areas of the involved occlusal surfaces that were excursively ink-marked. All posterior working and non-working excursive interferences were completely removed up to and including the 1st premolars bilaterally, while the remaining centric stop contacts were shaped into small pinpoint contacts located on supporting cusps, marginal ridges and central fossae. When visually assessed complete posterior disclusion was achieved for both the working and non-working movements on the first treated side, the same process was repeated on the opposite side.12,13,20 Following bilateral visual disclusion from ICAGD, adjustments were made to the remaining closure into MIP contacts, and all teeth were polished and smoothed. Finally, the posttreatment recordings of the same excursive movements were obtained for comparison to the pretreatment condition (Figure 3B).
RESULTS
The post ICAGD means of the Occlusion Times (the closure-into-MIP in the A to B time increment of the right and left excursions) were significantly reduced (p < 0.003 right, p < 0.00004 left). The post ICAGD excursive right and left means of the Disclusion Times (the C to D time increment) were also significantly reduced (p < 0.00001 right; p < 0.00008 left). The post ICAGD means of the percentages of Mid-course Corrections during left and right excursions were also significantly reduced (p < 0.0013 right, p < 0.0082 left). See Table 1.
Post ICAGD within the left lateral excursions, the means of the muscular contraction timing onset delays were significantly reduced for both temporalis muscles (p < 0.00003 right, p < 0.00003 left) and both masseter muscles (p < 0.0023 right, p < 0.00051 left). Also, the muscular effort expended by all four muscles within left excursions was significantly reduced, indicating there was more efficient muscular fiber recruitment and reduced muscle loads applied to the occlusion (p < 0.00001 for all four muscles). See Table 2.
Post ICAGD during right lateral excursions, the timing onset of contraction was significantly reduced in both temporalis muscles (p < 0.00001 right; p < 0.00009 left), and both masseter muscles (p < 0.00041 right; p < 0.00107 left). And there were significant reductions observed in the muscular effort expended within right excursions in all 4 muscles post treatment indicating the computer-guided ICAGD occlusal adjustments physiologically lessened muscle loads (TA-R p < 0.00001, TA-L p < 0.00005, MM-R p < 0.00001, MM-L p < 0.00001). See Table 3.
The pretreatment group mean pain score of 6.2 (+/- 1.2) was significantly reduced by 4.9 (+/- 1.3) points to 1.3 (+/- 0.98) post ICAGD (p < 0.00001). The smallest reported post ICAGD VAS reduction dropped 2 points from 5 to 3, with the largest reduction dropping 7 points from 9 to 2. See Table 4.
DISCUSSION
These significant results are indicative of definite improvements in the efficient recruitment of muscles, their effective utilization, reduced muscle hyperactivity, reduced in muscular effort, and reduced orofacial pain after applying the ICAGD method implemented through DTR therapy. Therefore, the null hypothesis was rejected, and the alternative hypothesis was accepted.
In this present study, significant differences were noted in five parameters post DTR therapy, that all directly resulted from computer-guided, time-based occlusal adjustments that brought the Occlusion and Disclusion Times into proven-physiologic numerical ranges.11–34 The reductions in Mid-course Corrections represented smoother excursive function absent of prolonged in time posterior tooth friction. And the improved muscular timing contraction onsets denoted easier and quicker recruitment of muscle fibers, while the four muscles expended less muscular effort to make excursive movements. Importantly, all 28 patients experienced immediate pain reductions posttreatment (see Table 4).
Prolonged Disclusion Times are associated with masticatory muscle hyperactivity.11–34 This overuse of muscles eventually results in the pooling of lactic acid in muscles leading to ischemic pain. By removing working and non-working interferences from molars and premolars to obtain measurably short Disclusion Times (< 0.4 seconds), predictably reduces Occluso-muscular symptomology.18 This study demonstrated that very precise computer-guided micro-adjustments drastically improved muscle efficiency corroborating the findings of 3 prior Randomized Controlled Trials (RCT)21–23 and additional 1-year,24 3-year,25 5-year,26 and 9-year27 follow up studies.
A unique aspect of this study was the inclusion of expended muscular effort measurements whereby excursive muscle effort was reduced after the ICAGD adjustments. This conclusively supports that the occlusion is likely one very important contributing factor when diagnosing myofascial pain patients.
This study is also unique in that the DTR treatments were all performed by trainees learning clinical ICAGD procedure, who had never performed DTR treatment prior to their participation in this study’s DTR learning environment. DTR chairside education involves over-the-shoulder, computer-directed diagnostic and treatment procedures performed on a minimum of 3 Occluso-muscular TMD patients, aided by a knowledgeable, previously a chairside trained and certified DTR educator. This study’s subjects experienced definitive myofascial pain symptom resolution and quick subject well-being improvements, illustrating that the ICAGD coronoplasty can be effective even when being clinically learned. Many prior studies have reported rapid symptom resolution with statistically significant physical and emotional changes occurred during and soon after the first treatment session.11–34
Of importance is that ICAGD and DTR can only be successfully learned chairside while treating patients. Computer-guided high-precision occlusal adjustments are not possible to grasp technically by watching a videotape or by just reading textbooks or technique papers that conceptually detail ICAGD. For a dentist to become a truly competent ICAGD clinician (as this study’s participants experienced), the authors strongly recommend that practitioners undergo chairside ICAGD training.
Lastly, many additional studies have demonstrated the effects of DTR treatment on various TMD signs and symptoms. Yiannios et al., showed that patients who underwent DTR therapy for myofascial pain reported significant reductions in cold tooth hypersensitivity.29 And Sutter et al., showed that DTR therapy reduced the symptoms of Meniere’s Disease.30 In another DTR paper, patients with Trigeminal Neuralgia symptoms improved statistically after DTR.31 And Thumati et al., reported a statistical reduction in bruxism post DTR.32 Then in a multi clinic study, PHQ-15 (Quality of Life) score improvements were reported post DTR therapy and in subjects that wore a TMD appliance.33 Moreover, in a TMD patient emotional depression study, Beck Depression Inventory (BDI-II) scores significantly decreased after DTR treatment.34 This depression study’s findings brings forth the question of whether orofacial pain was the cause of the subjects’ depression? Or did the emotional depression result in the orofacial pain? Because the Beck Inventory scores markedly dropped from a physical treatment (DTR/ICAGD computer-guided occlusal adjustment therapy), there exists either a Central Nervous System component of TMD that is occlusally caused,35 or DTR therapy can positively affect depression status through some undiscovered physiological mechanism.
LIMITATIONS
This study was limited in its’ sample size, in that subjects were their own pre to post treatment controls, and there was a minimal follow-up duration. The fact that patients traveled to the treatment center from various, far away parts of the country made it challenging for the authors to perform long term follow-ups. More such studies with larger sample sizes and long-term follow-up durations should be undertaken in the future.
CONCLUSIONS
This study’s outcome significantly supports the reported efficacy of DTR Therapy and the ICAGD coronoplasty to alleviate myofascial pain symptoms in patients suffering from long Disclusion Times and masticatory muscle hyperfunction. Occlusal factors were the only treated component that subjects underwent, indicating that the dental occlusion was etiologic for the myofascial pain symptoms observed in this study’s population.
Conflict of Interest
The authors of this study declared no conflicts of interest.
Informed Consent
Informed consent was obtained from all participants of this study.
Funding
No company/person/entity provided any funding to carry out this research study.