
Introduction
Tension-type headache (TTH), also referred to as muscle contraction headache, stress headache, or psychomyogenic headache, is thought to be the most common type of primary headache. The history to distinguish whether it is of primary or secondary type is most important in the evaluation of these headaches. The new-onset headaches and severe headaches are red-flags and should undergo assessment as potential secondary symptoms. The exact cause of TTH is rather poorly understood. Numerous theories have been proposed for the usually presumed pathophysiology of TTHs, but the exact pathophysiology remains unknown. The mainstream treatment options for TTH are nonsteroidal anti-inflammatory drugs (NSAIDs). TTH causes significant morbidity, resulting in absent workdays and reduced productivity. It also leads to increased stress and mood disorders.1
Physicians suggest that most headaches are diagnosed entirely on the patient history and that physical examination rarely provides clues to the diagnosis. Physicians also recognize that tension-type headache is the most common form of headaches, which is characterized by bilateral mild to moderate pressure. The recognized sources of tension headaches are likely the nociceptors in the pericranial myofascial tissues. (Hainer & Matheson, 2013)
A detailed system of classification and operational diagnostic criteria for headache has been published by the International Headache Society. It is based upon clinical consensus.2
"The exact mechanisms of Tension-type headache are not known. Peripheral pain mechanisms most likely play a role in infrequent episodic tension-type headache and frequent episodic tension-type headache, whereas central pain mechanisms play a more important role in chronic tension-type headache. Increased pericranial tenderness is the most significant abnormal finding in patients with any type of tension-type headache: it is typically present interictally, is exacerbated during actual headache and increases with the intensity and frequency of headaches. Increased tenderness is very probably of pathophysiological importance. ICHD-II therefore distinguished patients with and without such disorder of the pericranial muscles, a subdivision that is maintained in ICHD-3 to stimulate further research in this area.2
Physicians rely on favorable responses to medications as indicators that there is no primary (serious) etiology behind the patient’s headache. They recognize the importance of understanding the underlying pathophysiology of headache and the rationale for current pharmacologic therapies. “There are no prospective randomized controlled trials, evidence from meta-analysis from randomized controlled trials, or well-designed cohort studies to support or refute the practice of using response to therapy in nontraumatic headaches as an indicator of the absence of any potential underlying pathologic entities.”3
Clinical Case
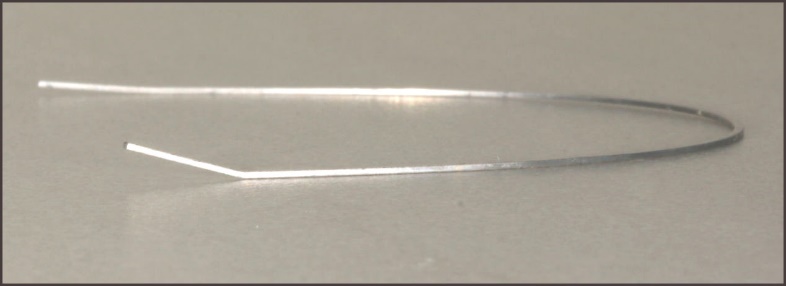
A Caucasian, 37 years old “middle-aged” female patient, who was undergoing active orthodontic treatment with non-removable appliances on both arches, was seen two weeks prior to the emergency for the checkup and appliance activation. At that regular orthodontic control appointment, new rectangular NiTi 0.017 x 0.025 inch wires were placed on both maxillary and mandibular arches. There were no complaints, no sign or symptom at the appointment. Two weeks later the patient communicated with complaints of sudden severe headaches and jaw muscle pains that she had trouble controlling with over-the-counter analgesics. She reported her sleep was not restful, and she had missed work due to the severity of her debilitating pain. Her pain started over the weekend, suddenly, without any apparent reason. Four days after the onset of pain we saw the patient. It was obvious she was in discomfort and agitated. She indicated that the constant severe pressure was on her forehead radiating to the temples and the back of the head, all were bilaterally. Her cheek muscles were tender. She had difficulty concentrating from the pain and needed to lay down regularly during the day. She was unable to work. There were no complaints of toothaches. Despite trying various over-the-counter analgesics (like acetaminophen, ibuprofen, naproxen) she found no relief. Her medical history was non-contributory. She is an active healthy person. Clinical examination revealed severe tenderness to all the muscles of mastication, including the masseter, the temporalis, and the pterygoid muscles. Every palpation led to a retraction movement by the patient to avoid the sensation of the palpation. Intraoral examination was inconclusive. The orthodontic hardware looked normal without any breakage, but a small bend was present in the mandibular wire between the last two right molars, teeth 46 and 47. See Figure 1.

Based on the history, clinical examination and the classification of the International Headaches Society, a working diagnosis of infrequent episodic tension-type headache associated with pericranial tenderness was established.2 Based on the Research Diagnostic Criteria for Temporomandibular Disorders, the patient presented with myalgia, myofascial pain and headaches attributed to TMD.4 Neither of these two classifications suggest any pathophysiological explanation or suggest any possible etiology regarding the patients’ complaints. They simply name the conditions based on history, signs and symptoms. They omit all objective digital data obtained with Biometrics.5
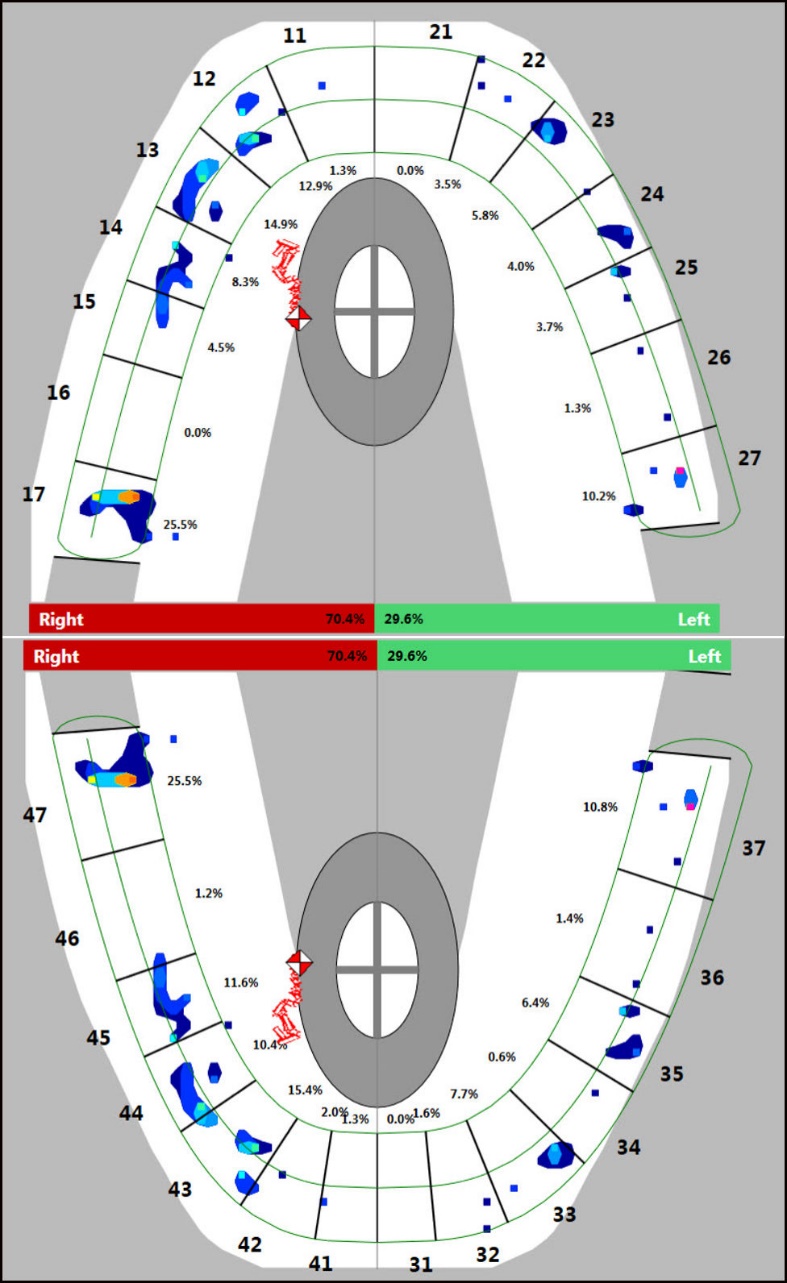
To obtain more objective information about the clinical presentation, it was decided to proceed with a digital occlusal analysis with T-Scan Novus Version 10.0.30 (Tekscan, Boston, MA). The recording of the maximum intercuspation and bite force was revealing. The forces of occlusion were significantly uneven with 70.4% right to 29.6% left, overloading the right side of patient. The last mandibular molar was receiving 25.7% of total occlusal force. See Figure 2. The first reflex could have been to intervene with an occlusal adjustment using a hand piece and reducing the excessively strong contact, but it was decided to simply remove the orthodontic wires, both the maxillary and the mandibular instead. The presence of a significant upward bend on the right side of the mandibular wire that would be situated between the first (tooth number 46) and second molar (tooth number 47), was discovered.
_recording_of_the_maximum_intercuspation.jpeg)
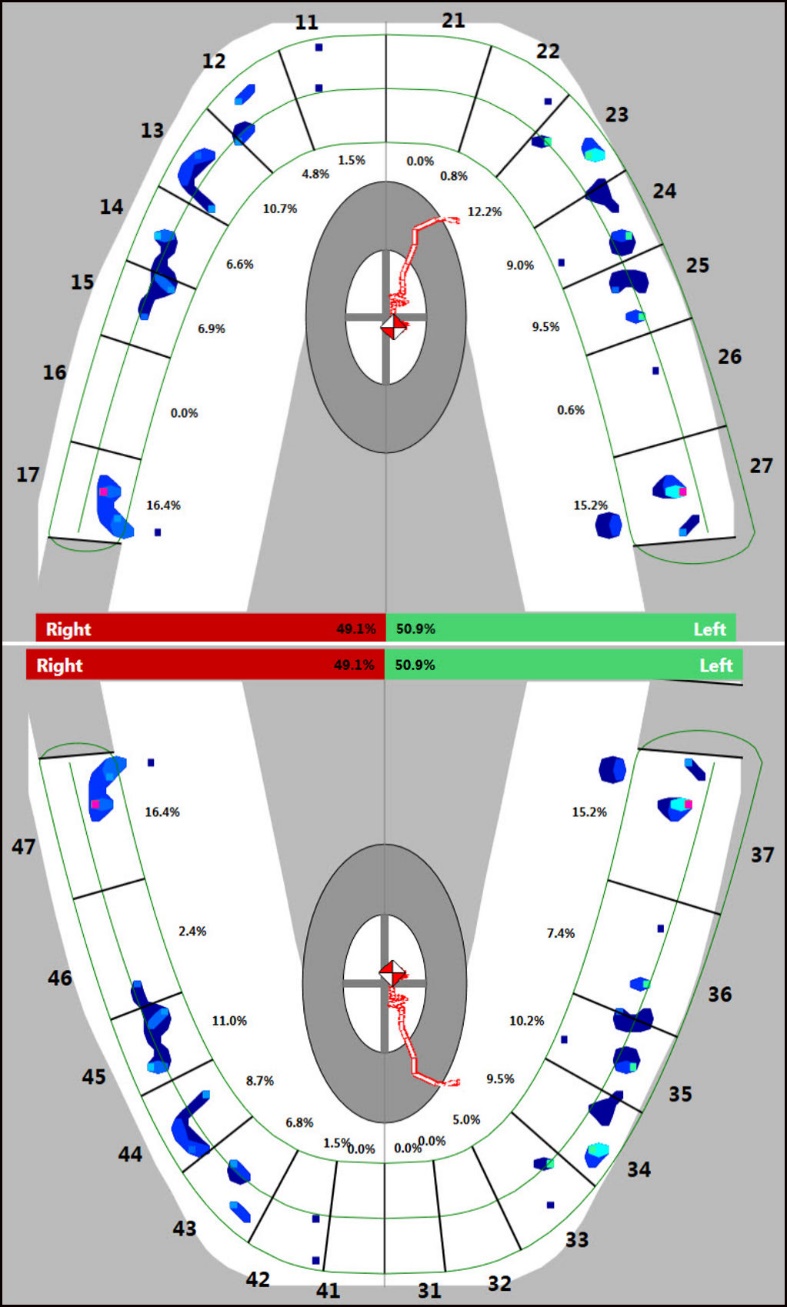
See Figure 3. This corresponded exactly to the tooth with the most relative occlusal forces. New unbent 0.017x0.025 NiTi wires were substituted and a new digital occlusion recording was performed with T-Scan, version 10.0.30 (Tekscan, MA, USA). The Forces of occlusion were changed, now to 49.1% right to 50.9% left, the second lower right molar (tooth number 47) no longer victim of excessive occlusal forces. See Figure 4. Within a few minutes, the patient explained that all the pressure was fading away, dissipating. When she left, she was visibly relieved and denied any pain.

_after_.jpeg)
Discussion
The resolution of the patient’s complaints with the re-distribution of occlusal forces through a change of orthodontic wires suggests a role for dental occlusion in the clinical presentation of orofacial pains. The asymmetries of occlusal forces between the left and right side of the dental arches, as well as the displaced position of the center of force (not centered) favoring the right side clearly indicate an unbalanced occlusal force profile. According to the recently published research on subjects seeking orthodontic treatment, the baseline Right-Left side Force Imbalance was roughly 56% on the greater force side in all three Angle’s classifications.6 This indicated moderate Right-Left side force imbalance at the initial exam.7 The same study indicated the presence of the first contacts occurring on the first mandibular molars. Both reported conditions are in agreement with the fact that diagnosed force imbalance in this orthodontic patient is very likely to cause of her cephalgia.
The significant force imbalance was associated with the patient’s complaints, which resolved after the re-establishment of an equilibrium facilitated by the change of the orthodontic wires. This clinical case also points out the possible contribution of orthodontic tooth movements to temporomandibular disorders, myalgia and to cephalgia. Skeptics may want to invoke causality; where one would argue that the change in symptomatology may not necessarily be the result of the clinical intervention, that this may simply be due to a placebo effect, not a modification of the forces of occlusion through the biomechanics of orthodontic wires. There is always someone willing to entertain logical arguments, especially logical fallacy experts, but the facts presented here through objective measurements, may trump any dogmatic opinions.
The role of dental occlusion in temporomandibular disorders and in orofacial pains represents a divisive subject in the dental profession. An erroneous and misleading review of the literature does not help by aggravating this situation. In one fallacious publication, the authors concluded that “This manuscript reviewed the literature on the association between features of dental occlusion and temporomandibular disorders. Based on findings, which support the absence of a disease-specific association, there is no ground to hypothesize a major role for dental occlusion in the pathophysiology of TMDs.”8 This paper has been since invalided by more recent publications exposing its flaws, omissions and logical fallacies. One of them clearly established the inadequacies underlining that the review represents an example of selection bias, with the omission of a large portion of the dental occlusion literature that best describes the relationship between occlusion and temporomandibular disorders (TMDs), notably the computer guided occlusion measurements of T-Scan studies of occlusal forces and timing. The erroneous conclusion of an incomplete review led to the lack significant association between occlusal features and all TMDs, therefore occlusion cannot be an etiological entity. The authors remind that an "association does not equal causation and that the reverse, a lack of association, does not eliminate an etiologic role, especially when there are 40 different TMDs conditions. In fact, the fourteen T-Scan studies ignored by these authors have thoroughly established the role of the precise dynamic measurement of occlusion in relation to specific TMDs conditions.9 Another author similarly and painfully reveals that this paper represents a bias review with cumbrous conclusions based upon the fallacious assumption that etiology cannot be ascribed to any occlusion factor that does not have a strong association with the entire category of temporomandibular disorders. Inasmuch as association does not equal causation, the entire premise of the review is false to begin with. Furthermore, it is again revealed that the systemic review omitted all Biometrics literature that measured the biomechanical and physiological relation between occlusion and temporo-mandibular disorders. This is an egregious example of the classical fallacy Cerasus Legend (suppressed evidence).10
Another review of the literature on the role of dental occlusion and temporomandibular disorders concluded however that this review of the current literature specifies, even though the etiology of TMD is understood to be multifactorial, that completely discounting the role of occlusion may be a highly inappropriate interpretation of published data. And that “a clear correlation between occlusion and TMD has not been clearly evident in the dental literature due to omission of the specific research principles and techniques outlined herein, it has, nevertheless, been proven in scores of independent research investigations conducted worldwide. A reform of occlusion/TMD research protocol is needed for progress in the field.”11
Digital occlusal parameters are clearly establishing the role of dynamic occlusion in the pathophysiology, by objectively measuring and quantifying parameters such as time and relative forces. In a study it was found, that “among the dynamic occlusal parameters evaluated centric slide and balancing side interferences were found to be highly influential in TMD etiology. TMD patients had prolonged occlusion and disclusion times compared to healthy TMJ patients.”12
The use of Biometrics, notably digital occlusion recording such as T-Scan, in a comparative study, demonstrated the existence of a relationship between the complaints of TMD patients and occlusion parameters; the centre of occlusal force distance and the occlusal forces’ asymmetry index in TMD patients with pain in the temporomandibular joint (TMJ) were significantly higher than in the control group.13
Diagnosis has the goal of integrating the disorders affecting an individual, clarify the type of pains present, and the needed treatments. Myalgia and myofascial pain represent pain that originate from muscles. Myalgia refers to muscle pain without a specific etiological or causal mechanism. Myofascial pain is described as spreading or referring pain, yet without any reference to a specific mechanism, causal or etiological pathophysiology. There is also an absence of evidence suggesting any treatment is preferred to treat either myalgia or myofascial pain. Currently, the biopsychosocial orofacial pain care model for myalgia preconizes self-management for symptom control and behavioral therapy.14 The clinical relevance and practicality of applying the biopsychosocial approach to all TMD is questionable.15
Super elastic nickel-titanium (NiTi) alloy orthodontic wires (0.017 x 0.25) can generate during loading, extrusive force of 4.98N at 4 mm of deformation.16
The accidental bending of the mandibular wire unilaterally on the right side, induced a displacement of the second mandibular molar with a tipping movement leading to the mesial inclination of the tooth. This uncontrolled tipping can be described as a mesiolingual inclination and elicits a movement of the tooth by exerting a three-dimensional displacement. The initial accidental orthodontic tooth movement is produced by elastic deformation of the periodontal ligament.17 The periodontal ligament has been thoroughly studied and described as a space ranging from 200 to 500 microns.18 It is understood that the periodontal ligament mechanoreceptors play an important role in the sensori-motor control of the muscles of mastication.19 Some authors have provided a hypothesis to explain the clinical presentation of patients who may feel pain both from the PDL and from other oral structures during orthodontic tooth movement. It involves both peripheral and central mediate contributions of the nervous system.20
Although the exact extrusive forces or displacement of the accidental bent in the patient’s wire was never measured directly, the result was objectively quantified by the digital recording of the relative forces of occlusion with T-Scan, Version 10.0.30. As continuous wires exert forces in all three directions acting at every bracket/tube, these forces are difficult to quantify. The change of the distribution of these forces, through the change of orthodontic wire, lead to a resolution of the patient`s pains and complaints. Newton’s third law states that for every action, or Force, in nature, there is an equal and opposite reaction. The V-bend accidentally incorporated into the wire has created an added system of forces with tipping and rotation of both the first premolar and second molar on the right side. The latter experienced distal cusp extrusion. It may also be noticed that the first premolar on the same side experiences 8.2% of relative force. The continuous wire system is a force system that cannot be directly quantified and is not a simple summation of V-bend systems. Thus, multiple effects are exerted on all teeth surrounding the wire bent. Although after wire adjustment both, the first premolar and the second molar had significantly lower relative force levels and centre of force was re-centered. What is the reaction of the stomatognathic system to the new orthodontic forces generated by the accidental bent of the wire? The exact answer in terms of Physics or Biophysics is well beyond this paper and perhaps the dental profession, but the consequences in terms of orofacial pains are obvious and clearly reported by the patient. The new accidental orthodontic forces were well beyond the adaptive capacity of the stomatognathic system of this patient, which lead to a cascade of clinical signs and symptoms that did not resolve with self-medication or palliative home care. What behavioral changes could the suffering patient modify to alleviate the pain? After too many days of unresolved symptoms despite the best efforts of the patient, a dental consultation was scheduled as an emergency, due to the debilitating circumstances for this orofacial pain/ortho-dontic patient.
The biometric digital recording of occlusion revealed the obvious asymmetrical distribution of the relative occlusal forces between the right (70.4%) and the left side (29.6%) of the dental arches and the excessive relative load of the second molar of the affects side (25.7%). These asymmetries of relative forces must require an adaptation or reaction of the stomatognathic system, according to Newton’s Third Law. The stomatognathic adaptive motor syndrome accounts for the changes observed in the clinical case presented here.21 Whereas the biopsychosocial models fail to provide any useful clinical guidance. According to a recent publication, “Since orofacial pain is unlikely to be cured, given current knowledge, patients need to play an active role in using strategies to reduce their pain or the impact it has on their life. This is known as self-management and provides a firm foundation for tailored medical management strategies. Biopsychosocial considerations have an important role in supporting successful self-management.”22 This biopsychosocial approach to orofacial pain regresses the profession to pain management, with little hope for the suffering patient, whereas physical corrective procedures, addressing the etiology, should be considered the standard of care.15
A clinical intervention, through the change of the damaged orthodontic wire, lead to the re-establishment of the symmetry of relative occlusal forces, 49.1% on the right and 50.9% on the left. The elimination of the forces applied by the bent orthodontic wire was sufficient to regain an even distribution of the occlusal forces. This obviously relates to Newton’s third law. The adaptations, or mis-adaptation, to the previously applied forces from the bent wire, were no longer necessary, and within minutes, the patient’s complaints dissipated. Peter Dawson has explained that the removal of occlusal interferences leads to an immediate relief of pain.23 In a classic textbook, Occlusion, Ramfjord and Ash, explain that TMDs are consequences of any disharmony in the functional relations between the teeth and support structures, the masticatory muscles, the maxilla and mandible, the TMJ, and all the neurovascular supply to these structures.24
The mechanisms of craniofacial and the major contribution of the fifth cranial nerve has been reviewed and described in detail.25 Putative and theoretical explanation for the pathophysiology of primary headaches are what is currently available today. Peripheral and central sensitizations with possible imbalances between the sympathetic and parasympathetic neural systems are possibilities, but the exact mechanisms remain unexplained.26 A broad classification of headaches divides them as primary, without any underlying cause, and secondary, the result of another pathology. Primary headaches include tension type, migraine, and cluster headaches. Nociceptors are absent in the brain parenchyma, thus primary headaches pains are thought to originate in surrounding structures, including blood vessels, meninges, muscles, facial structures surrounding structures and cranial or spinal nerves. But the pathophysiology of primary headaches remains not fully understood.27
One literature review erroneously concluded an absence of any role for dental occlusion in all temporomandibular disorders. Therefore, the use of occlusal equilibration in treatment or prevention of TMDs should not be recommended. The author negates occlusion with respect to the pathophysiology of all temporomandibular disorders and states that it is an “old precepts of gnathology,” without any biological rationale.28
It is accepted that temporomandibular disorders is a non-specific collective term for musculoskeletal conditions related to pain and dysfunction of the temporomandibular joints, masticatory muscles and associated structures. Some groups have suggested that the pathophysiology of painful temporomandibular disorders is biopsychosocial and multifactorial, without any one specific etiological factor or factors. They suggest the existence of predisposing, initiating and perpetuating factors with peripheral and central mechanisms, but caution of the ongoing investigations to clarify the exact causal pathway and mechanism-directed diagnosis and treatment.29
It is obvious that the pathophysiology of orofacial pains remains unclear, unknown, and elusive. To exclude the occlusion as an etiological factor is obdurate, astigmatic fanaticism and potentially harmful to suffering patients. The advance of computer guided occlusion measurement, with the biometric instrumentations like T-Scan and BioEMG III (BioResearch Associates, Inc., Milwaukee, WI), continue to provide objective data and evidence towards a definite role for dental occlusion in orofacial pains. Dr. Robert Kerstein has published a detailed clinical case on the occlusal management of headaches.30 His work spans multiple decades and culminate in a collection of volumes.31 Others have replicated the research findings of Dr. Kerstein, adding objective data and support to the role of occlusion in the pathophysiology of temporomandibular disorders.32 Computer analysis of occlusion and computer guided occlusal intervention was also instrumental towards the resolution of headaches in another clinical case.33 The benefits of computer guided coronoplasty have been documented and demonstrated beneficial initially and over extended time periods in myofascial pain patients.34 Further support towards the contribution of occlusion in temporomandibular disorders and the clinical efficacy of digitally measured occlusion and computer guided coronoplasty was granted in randomized controlled trial.35 One of the major papers describing the use of the T-scan digital occlusal analysis in Orthodontics describes the purposeful wire bending procedures at the detailing stage which dissipates forces of occlusion and balances Right-Left side force imbalance. Thus, wire bending effects could be beneficial for redistributing occlusal forces and decreasing the excessive relative forces, as well as finding teeth primarily occluding during the initial closure and preventing from proper mandibular placement against the upper arch.7
Conclusions
The infrequent episodic tension-type headache associated with pericranial tenderness inflicting an orthodontic patient, does not have an exact pathophysiological or etiological cause base on all the publications related to the classification of the International Headaches Society. According to the Research Diagnostic Criteria for Temporomandibular Disorders, the patient presented with myalgia, myofascial pain and headaches attributed to TMD, yet there is no exact pathophysiological or etiological cause for any of these diagnoses, all based on signs history, signs and symptoms.
The technological advances of digital biometrics are granting the clinician a powerful and objective means to measure and quantify the occlusion, providing further useful information in the examination, diagnosis, and treatment of orofacial pain patients. The clinical case presented here is an example of the power of T-Scan, a digital measuring tool. Without the objective data and information, it provided, it would have been impossible to discern the discrepancy and disequilibrium of the forces of occlusion that lead to the symptomatology and complaints of the orthodontic patient. The biopsychosocial approach to pain management and treatment, based solely on the diagnosis of infrequent episodic tension-type headache associated with pericranial tenderness would have been inadequate to address the etiology or primary causal biomechanical issues of this orofacial pain/orthodontic patient. It is imperative that the dental profession and especially the orofacial pain component of dental medicine relegates old concepts, abandons disparate opinions and adopts the digital Biometrics for the benefit of the patients. It is insufficient to describe all the temporomandibular disorders and headaches solely in term of signs and symptoms. This method of diagnosis provides no insight into the pathophysiology and cause of the disorders and limits treatment to pain management. Resolution requires a different approach to examination and diagnosis, one focused on objective and quantifiable measurements and data that provide information on the etiology and pathophysiology; that is the contribution of digital Biometrics. This presented clinical case demonstrates the immediate resolution of the signs and symptoms with a correction of excessive relative forces of occlusion brought by a faulty and accidentally bent orthodontic wire. This objectively measured and presented clinical case should awake the minds of the profession and open the eyes of the clinicians and academics to the reality of the factual contribution of occlusion as a common etiological entity with respect to many orofacial pains, temporomandibular disorders and headaches.
Conflict of interest statement
The authors declare no conflict of interest.
Funding
No funding was provided for this case study.