



INTRODUCTION
MRI is considered by many as the theoretical “gold standard” for diagnosing temporomandibular joint (TMJ) conditions involving disc displacement with reduction (DDR) or without reduction (DD) and degenerative joint disease (DJD), but its cost and availability may present some challenges.1,2 However, a single examiner may not be too reliable when MRIs are used in a vacuum for TMJ diagnosis.3 Some consider cone-beam computerized tomography (CBCT) more reliable for detecting certain degenerative conditions.4 Thus, the combination of MRI + CBCT may be a better “Gold Standard.” Joint Vibration Analysis (JVA) (Bioresearch Associates, Inc. Milwaukee, WI USA) has emerged as a non-invasive and cost-effective alternative for dynamically assessing temporomandibular joint function.5 The JVA Flow Chart categories TMJ conditions according to the Piper Classification System using the patient’s Range of Motion, the vibrations’ calculated amplitude ranges, and the frequency characteristics as variables; 1) Total Integral, 2) Range of Motion, 3) the separate amount of energy above 300 Hz and 4) the Ratio of the energy “above 300 Hz / below 300 Hz.” The JVA Flow Chart categorizes TMJ conditions using these parameters.6 Figures 1 & 2.


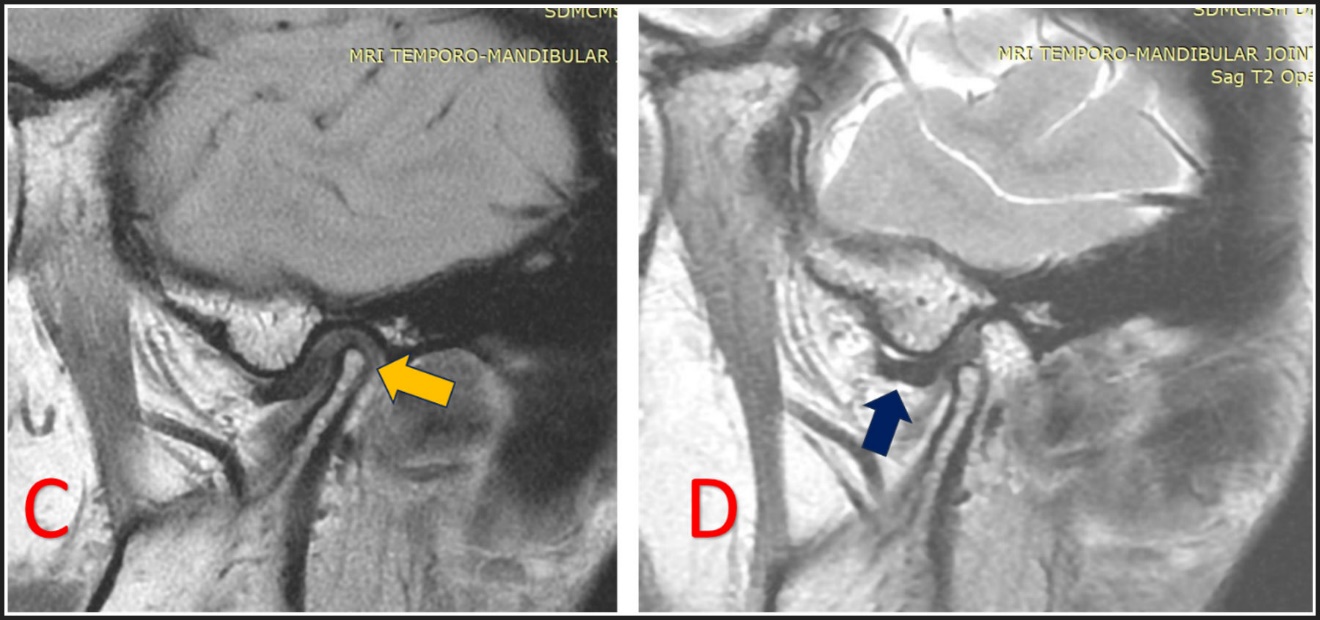
Temporomandibular disorders (TMD), which can affect 5% to 12 % of the population, often involve the temporomandibular joint (TMJ), occlusion, masticatory muscles, and all supporting tissues. These disorders are categorized into articular inflammatory conditions, (such as rheumatoid arthritis),7 and non-inflammatory, (such as osteoarthrosis) and non-articular types.8 The TMJ often produces various sounds, especially in cases of internal derangement where the disc is displaced, reduced, and/or folding.2 An accurate diagnosis of any TMD requires a comprehensive history, a physical examination, and supplemented by radiographic studies.9 Thus, MRI of the TMJ can play a crucial role in detecting disc displacement and assessing disc location in articular disorders. Its primary advantage is the use of non-ionizing radiation to produce high-quality soft tissue images. See Figure 3, 4 & 5.
MRI is also essential for identifying subtle osseous changes in the joint.9 Consequently, MRI has been considered the gold standard imaging technique for visualizing the TMJ, detecting inflammatory changes within the joint space, cartilage abnormalities, and positional alterations of the disc. However, its effectiveness is offset by its expense, a requirement of expert interpretation, and limited availability.9,10
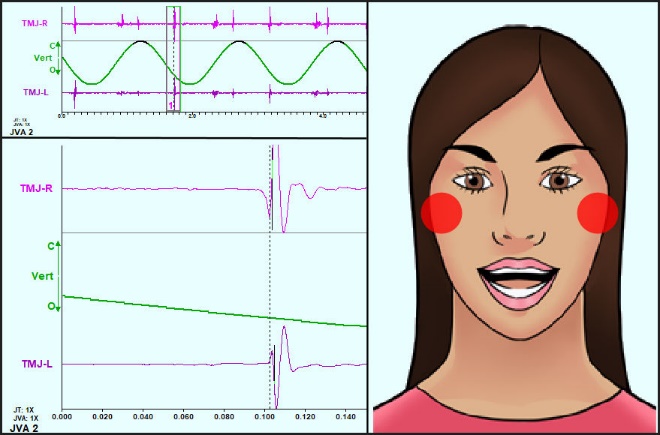
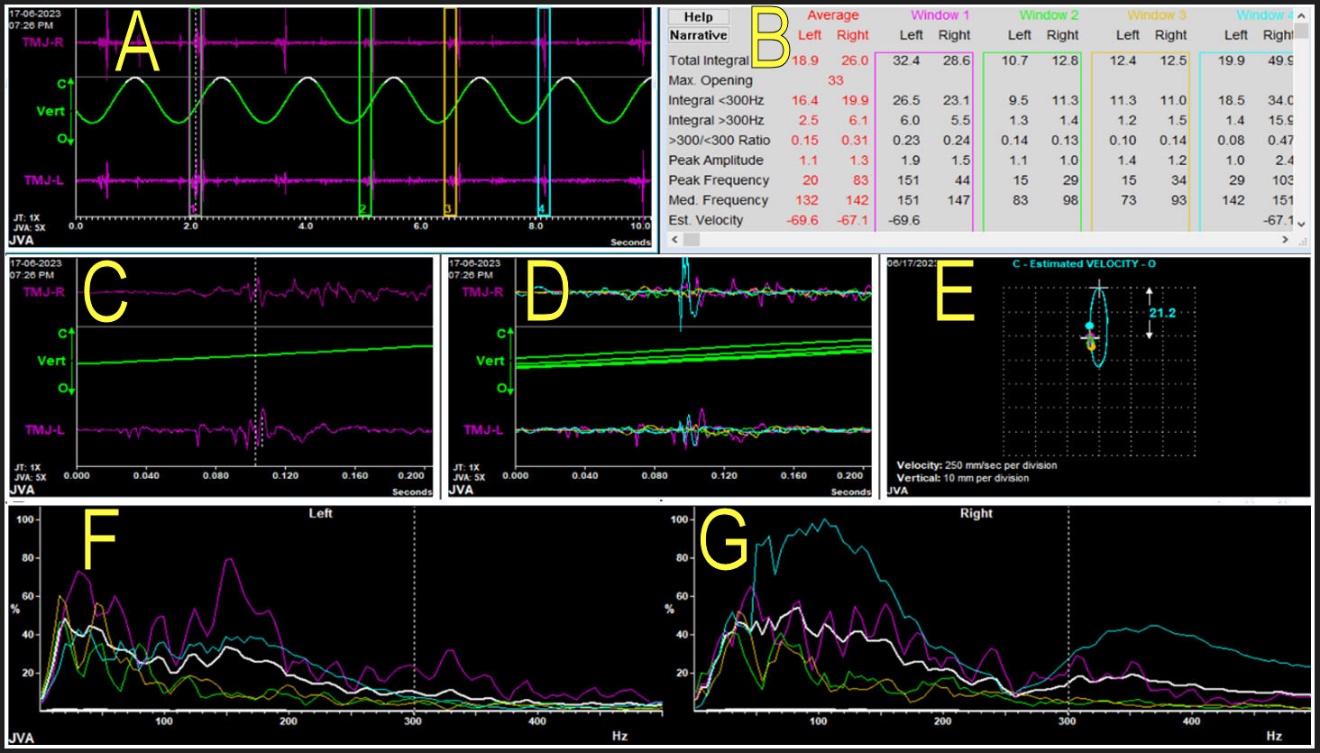
Hence-forth, in recent years Joint Vibration Analysis (JVA) has emerged as a recognized, non-invasive, cost-effective, and reliable auxiliary classifying method for TMJ analysis.9,10 It provides precisely calibrated data from the articular noises and friction making it a valuable tool for dynamically revealing various TMJ disorders with a high specificity (98 %) in TMD clinics.5,6,11,12 JVA records vibrations during mandibular movement from within the ipsilateral joint with a disorder, and simultaneously records all vibrational energy transferred to the contralateral joint, which aids in determining the disc displacement direction and morphological changes.13,14 Using the BioPak software (BioResearch Associates, Inc., Milwaukee, WI USA), JVA analyses the strongest vibrations to evaluate joint condition.9,14–16 See Figure 6

)_of_the_left_side_showing_a_compl.jpeg)

_shows_a_medium_intensity_vib.jpeg)
Parameters Included in the JVA Flow Chart17 See Figures 7 & 8.
a) Total Integral: This measures vibration intensity by summing energy across all frequencies, categorized into amplitude ranges correlated with TMJ conditions:
-
Small intensity (0-20 KPaHz): Indicates 1) normal joints (ROM > 40 mm), or 2) acute complete disc displacement (ROM < 30 mm), or 3) inactive osteoarthrosis (ROM < 40 mm).
-
Medium intensity (20-80 KPaHz): Indicates 1) loose capsules (ROM > 40 mm), or 2) chronic adapted permanent disc displacement (30 mm < ROM < 40 mm), and/or 3) osteoarthritis (> 300 Hz).
-
High intensity (80-300 KPaHz): Indicates 1) chronic adapted displaced discs reducing, or 2) maladapted non-reducing discs, and/ or 3) eminence click. (Note: Values near 80 indicate a long-term chronic condition, while values approaching 300 indicate relatively more acute conditions.)
-
Very High Intensity (300-1000 KPaHz): Indicates 1) acute reducing disc displacement, 2) with or 3) without chronic degenerative joint disease.
-
NOTE: KPaHz = KiloPascal x Hertz = units when Intensity is multiplied by Frequency
b) Range of Motion8,11: The normal range of motion (ROM) for the adult jaw typically extends from 40 mm to over 70 mm (mean value = 50 mm)17 and includes adequate lateral and protrusive movements. Most children exceed 40 mm by 5.2 years of age.18 Monitoring the maximum opening movement is critical as it indicates how the two condyles translate relative to each other. Balanced condylar translation results in a straight opening, symmetrical lateral movements and uniform protrusive movements. A unilateral anteriorly displaced disk caused by internal derangement restricts ipsilateral condyle translation, leading to lateral deflection towards the affected side during opening and protrusion, while limiting lateral excursion to the contralateral. Significant deflections and reduced ROM below 40 mm can hinder contralateral chewing, whereas minor deflections accompanying normal ROM could result from slight jaw asymmetry or slight hyper-translation of the opposite condyle. A well-adapted Chronic disk displacement can eventually exhibit nearly normal ROM over time (30 – 40 mm), but with lateral deflection in unilateral cases. Bilateral permanent disc displacement (DD) that is well adapted can allow normal function and when it does, represents a contraindication for any joint treatment.
c) Integral > 300 Hz Significance8,11,14,17: Vibrations caused by TMJ disc movement, loose capsule, or by the reduction of partial or complete disc displacement typically have frequencies below 300 Hz. Acute vibrations may produce additional harmonics above 300 Hz, as can TMJ degenerative changes. For reduction vibrations the Ratio >300 Hz/<300 Hz automatically compensates for harmonic content because the > 300 Hz harmonics are masked by the < 300 Hz vibration. When that doesn’t happen, it indicates a more severe degenerative condition.
d) Energy Ratio at Frequencies <300/>300 Hz:8,11,14,17 For medium, large, and huge vibrations, a ratio (> 300 Hz / < 300 Hz) exceeding 0.300 suggests potential joint degeneration. The ratio automatically compensates for harmonic content of acute reductions. The Ratio is disregarded when the Total Integral is below 20 to avoid distortion from system noise. In very small vibrations, the > 300 Hz Integral alone identifies degeneration, as background noise is automatically subtracted.
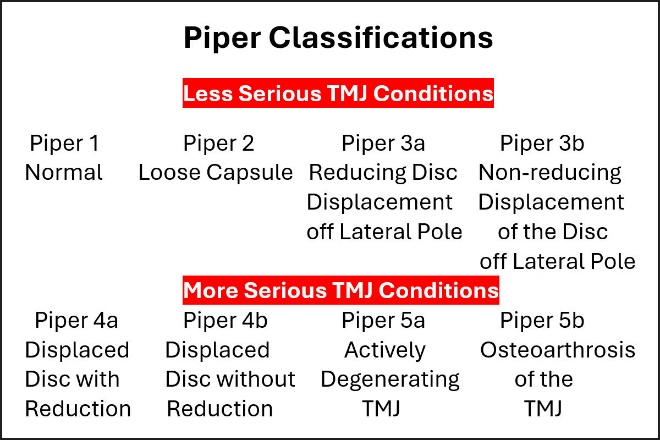
After evaluating these variables, the joints are categorized according to the Piper classification system.8,10,19 See Figure 7.
-
Piper Class 1: Normal Temporomandibular Joint
-
Piper Class 2: Loose capsule, disc may occasionally displace off lateral pole of condyle
-
Piper Class 3a: Consistent reduction of partial displacement off lateral pole of condyle
-
Piper Class 3b: Permanent partial disc displacement off lateral pole of condyle
-
Piper Class 4a: Disc reducing from anterior, lateral, medial or posterior displacement (DDR)
-
Piper Class 4b: Nonreducing complete disc displacement without reduction (DD)
-
Piper Class 5a: Displaced disc with actively adapting degenerative joint disease (DJD)
-
Piper Class 5b: Displaced disc with osteoarthrosis, adapted end stage of DJD


Because of the inadequacy of the RDC/DC/TMD Axis I clinical examination of TMD patients, added input such as MRI or CBCT are recommended.20 JVA serves effectively as a valuable screening tool in a clinic for identifying TMJ internal derangements and disc displacements. JVA is a comprehensive dynamic structural assessment of the joint before any intervention and often indicates the likely value of any added Imaging.
OBJECTIVES OF THE STUDY
The objective of this study was to assess the efficacy of the Joint Vibration Analysis (JVA) Flow Chart in distinguishing different types of internal derangements of the TMJ and degenerative joint changes by comparing its results with combined MRI and CBCT “gold standard” findings.
MATERIALS AND METHODS
Inclusion Criteria: Fifty-nine participants (40 Female) with symptoms including one or more of the following: pain, headache, ear pain, tenderness in the lateral pole of the joint, restricted mouth opening, reduced range of motion, clicking or crepitation, and structural changes such as disc morphology or condyle architecture (e.g., degenerative joint disease and osteoarthritis) were enrolled in the study.
Exclusion Criteria: Participants were excluded if they were using long-term muscle relaxants, had current neurological or cognitive impairments, presented with metabolic or nutritional factors indicating low muscular activity, lacked posterior teeth, experienced dental pain, had unstable dental prostheses, or reported any oral discomfort preventing maximal clenching.
Procedure
The participants underwent clinical assessment based on RDC/TMD criteria for internal derangements and arthralgia, followed by CBCT and MRI scans for comparative analysis. All participants provided informed consent in accordance with the seventh revision of the World Medical Association Declaration of Helsinki (2013), emphasizing the publication of studies describing any negative findings. JVA System (Bioresearch Associates Inc., Milwaukee, WI, USA) evaluation required placing equipment sensors over each temporomandibular joint’s articular capsule, positioned 15 mm anterior to the auricular canal.11 See figure 1. All subjects were seated upright and synchronized their mouth movements with a metronome on a computer screen. See Figure 2. The JVA program also includes a pacing metronome for the patient to follow to estimate jaw position at the onset of vibration. A recorded in-phase tooth tap vibration indicates that the patient successfully produced closure into the maximum intercuspation position (MIP).8,11 BioPak software recorded the vibrations, identified the most intense vibrations and calculated these variables: Total Integral, Integral >300Hz and the < 300/>300 Ratio, which, along with the Range of Motion, were applied to the JVA Flow Chart.8,11–14 See Figure 8. Specific waveforms were examined to detect and classify joint disorders such as inflammation, disc movement, disc displacement with or without reduction, and degenerative joint disease. Subsequently, results from both imaging and JVA were classified using the Piper classification system,8,11,19 which definitively categorizes TMJ conditions into 8 stages from normal to severe dysfunction. See Figure 7.
RESULTS
The JVA Flow Chart Piper classifications and Gold Standard imaging were in close agreement, with JVAs mean classifications only slightly less severe, compared to the combined MRI & CBCT Piper classifications. For the mean of the left TMJs (p < 0.4715) and for the mean of the right TMJs (p < 0.7279) the classifications were slightly less severe, but NOT significantly different See Tables 1 & 2.
The RDC/TMD Piper Classifications were significantly more severe than the Combined MRI & CBCT (gold standard) findings for the left TMJs (p < 0.04273). See Table 1. A significant difference was also found for the right TMJs (p < 0.0188). See Table 2.
When the OPG findings were compared to the CBCT findings from the left TMJ they were significantly less severe and less detailed. See Table 3. Likewise, the comparison of the OPG findings to the CBCT findings from the right side were significantly less severe and detailed. See table 4.
DISCUSSION
Joint Vibration Analysis was originally conceived as an intermediate capability between the inadequacies of the clinical examination of TMDs and the expense of precise sophisticated imaging technologies.5,11,17 JVA is currently used in many TMD clinics on a routine basis to document the conditions of all patients’ TMJs prior to any contemplated treatments.21 It is a one-minute test typically done by staff and read by the clinician using the JVA Flow Chart.21 There is no consumable cost to the JVA test, minimizing the per use cost. JVA allows the clinician to establish the normalcy of a new patient’s TMJs and to frequently monitor symptomatic TMJs economically and non-invasively over time all done within a clinic.
While a great deal of effort and resources have been expended on the RDC/TMD since 1992,22 as well as its renamed DC/TMD, the clinical examination portion using Axis I has been shown to have very inadequate sensitivity and specificity.23–25 The proposed revisions for the RDC/TMD for the DC/TMD have not improved it sufficiently for clinical usage.24–26 Although the DC/TMD has acknowledged that Imaging is needed to diagnose Internal derangements correctly, no indications have been established as to when or what type of imaging should be obtained. The data in this study confirm the lack of concurrence between the Axis I of the RDC/DC/TMD and Gold Standard Imaging.
“Axis I diagnostic criteria for the most common temporomandibular joint (TMJ) intra-articular disorders are appropriate for screening purposes only. A definitive diagnosis for TMJ intra-articular disorders requires computed tomography or magnetic resonance imaging.”27
The OPG x-rays were interpreted by experts, and they most often noted flattening of the condyle and occasionally an erosion. The mean number of findings from the OPG images was only 1.3 conditions/subject, while the mean number of findings from the CBCTs was 2.2 conditions/subject. See Tables 3 & 4. This represents a large degree of under reporting from the OPG data. Since Piper classifications were not derived from the OPG x-rays, no comparison could be made with the JVA Flow Chart designations.
LIMITATIONS
Since the MRIs and CBCTs were interpreted by expert clinicians it’s likely that less skilled interpreters could arrive at somewhat different results. The RDC/DC/TMD Axis I data relies solely on the subjective interpretive skill of the examiner, different examiners can produce very different results.22–27 JVA requires the operator to recognize and mark the same, most intense vibration in each cycle. Then the objectively measured values generated by the program must be manually input into the JVA Flow Chart. Less experienced operators could mismark the vibration data or mis-enter the results into the JVA Flow Chart. However, this process is straight-forward such that in most practices auxiliary staff can implement the JVA with the Flow Chart.
CONCLUSIONS
The mean JVA Flow Chart categorizations identified internal derangements of the TMJ comparable to gold standard imaging while indicating slightly less severity. However, the Axis I of the RDC/DC/ TMD did not agree with the gold standard imaging or with the JVA Flow Chart categorizations. The Axis I mean categorizations indicated significantly greater severity (e.g. often stage 4 instead of stage 3). The interpretations reported from the OPG x-rays included significantly fewer conditions (only about half) than those reported from the CBCT interpretations.
DISCLOSURES
Noureen Nahar, (MDS), Post Graduate Student, Department of Oral Medicine and Radiology, SDM College of Dental Sciences and Hospital, Sattur, Dharwad, Karnataka, India.
Atul P. Sattur, MDS, Professor, Department of Oral Medicine and Radiology, SDM College of Dental Sciences and Hospital, Sattur, Dharwad, Karnataka, India.
John Radke, BM, MBA, Chairman of the Board of Directors of BioResearch Associates, Inc. Milwaukee, WI USA
Krishna Burde, MDS, Professor, Department of Oral Medicine and Radiology, SDM College of Dental Sciences and Hospital, Sattur, Dharwad, Karnataka, India
ACKNOWLEDGEMENTS
The Piper Classification System was developed by Mark Piper, DDS, MD.19
FUNDING
No funding was provided from any source.