



INTRODUCTION
Prosthetic complications are a major problem for implant prostheses. High fracture rates and porcelain chipping are common,1–12 with multiple unit fixed partial dentures being the most prone to prosthetic complications.8 Peri-implant bone loss has also been reported as a post insertion implant complication.1 A 2018 systematic review reported metal-ceramic implant-supported fixed dental prostheses (FDPs) had a 5-year ceramic fracture and chipping rate = 11.6%, while zirconia implant-supported ceramic fracture and chipping rates = 50% (p < 0.001). Further, 4.1% of the zirconia FDPs were lost, while only 0.2% of the metal-ceramic implant FDPs were lost. The authors suggested that veneered zirconia should not be considered as the first occlusal material option.4
Additional long-term prosthetic studies confirm that high complication rates plague implant-supported restorations.2,5,8–12 In a 10-year study of 397 implant-supported reconstructions, over 25% of the studied restorations sustained mechanical complications. The most frequent complication was ceramic chipping (20.31%), followed by occlusal screw loosening (2.57%), and loss of restoration retention (2.06%).8 In another 8-year study of 114 implant-supported full-arch immediate load prostheses, 54% of the implant restorations sustained some form of mechanical failure, with prosthesis fracture being the most common complication.5 And, immediate load All-on-Four/Six restorations appear to be highly prone to prosthetic breakage (Figure 1).7 Although Implant Prosthodontics has improved digital tools, “the Digital Work Flow”, has not improved complication rates, despite guided surgery and improved implant placements based upon bone quality and prosthetic convenience.1,2,4–14

Excessive occlusal force loading on implants has been implicated in the failure of occlusal materials and implant de-osseointegration, with generalized agreement that early implant failure and prosthesis material fracture is associated with overload.13 The absence of periodontal ligaments around restored implants results in a lack of normal proprioception, with patients exhibiting an inability to sense the degree of force delivered occlusally to an implant prosthesis.15 That lack of sensibility compounds the inherent rigidity of an implant prosthesis. Further, a clinical report using the T-Scan 10 digital occlusal analysis technology (Tekscan, Inc., Norwood. MA, USA) at case insertion illustrated that implant occlusal contact forces rise very quickly, because the rigid implant systems poorly absorb the applied occlusal forces.16
Although it has been suggested that implant restoration design features may theoretically reduce occlusal stress (increase the number of supporting abutments, stagger implant positions, increase implant body width, decrease occlusal table width, minimize the number of pontics, remove cantilever occlusal contact, minimize lateral excursive contacts, and minimize bruxism and clenching effects),17 these prosthetic design features alone cannot lessen occlusal contact forces solely by design. To control occlusal force successfully, one must measure between occluding implants the actual relative contact forces and pressure distribution of all occlusal contacts, and then contour those occlusal contact shapes so that low relative occlusal forces load an implant prosthesis.
Managing interocclusal contact force control is possible using the T-Scan 10 Novus system (Figures 2ab). The HD Novus sensor, when interposed between occluding implant crowns, can record 256 levels of relative occlusal force in real-time. The T-Scan system has been repeatedly evaluated for its’ occlusal force reproduction,18–24 has been involved in dental occlusion studies,25–27 Temporomandibular Disorder (TMD) treatment studies,25–35 and implant research studies and clinical reports.3,36–41
_the_small_hd_novus_sensor_being_loaded_into_the_t-scan_10_recording_handpiece._b)_the_n.jpeg)
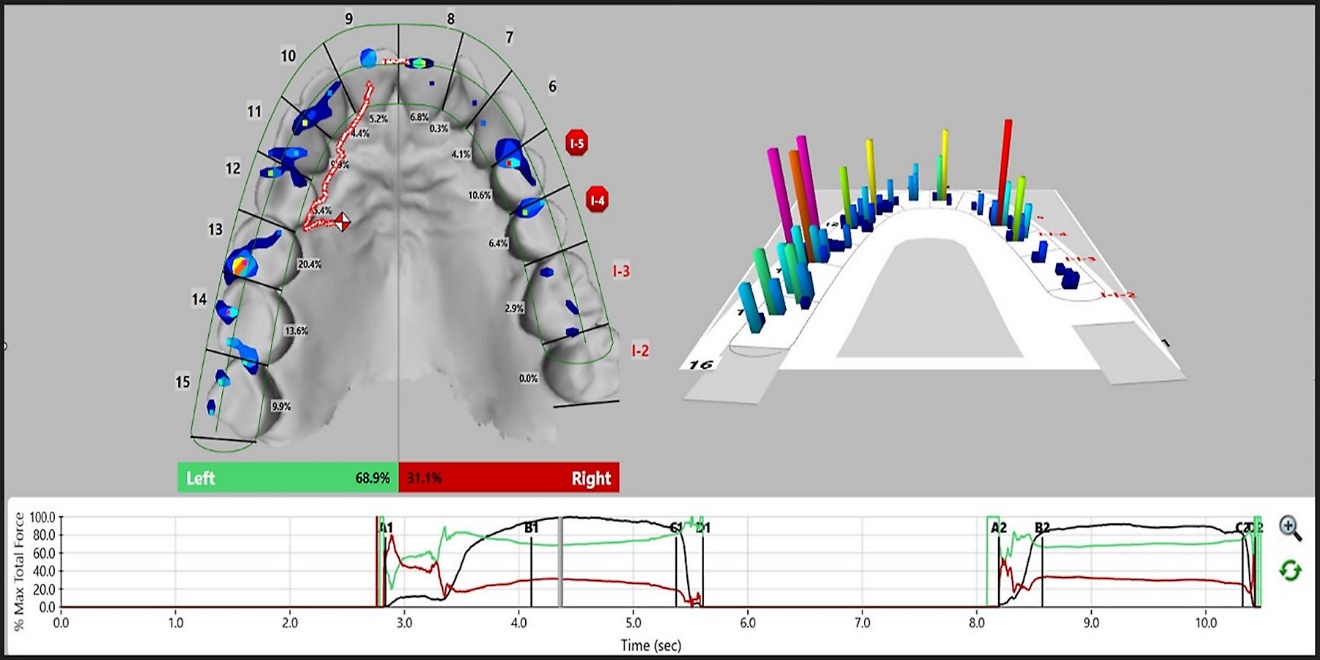
T-Scan data can guide occlusal adjustments to make targeted corrections to occlusal force excess.42,43 And the desktop software contains an Implant Warning alert (Figure 3) that detects when an implant is sustaining high occlusal force, is time-early, or occludes faster compared to nearby natural teeth.44

One element of why excessive occlusal loading occurs on dental implants that has not yet been implicated in the literature, but likely contributes to the many reported material and osseointegration complications is the subjectivity employed when occlusal adjustments use traditional occlusal indicators.39–41 Studies show articulating paper or film, silk ribbon, occlusal wax, silicone imprints, articulated stone casts, shim stock, and intraoral scanners (IOS), do not in any way record, measure, or digitally represent occlusal contacts.45–48 (See Figure 4.) Although some IOS prognosticate an “Occlusogram,” the intraoral scanning is done with all the teeth apart, so no actual interocclusal forces can possibly be recorded.

And despite the widely held (incorrect) beliefs that articulating paper marks indicate occlusal contact force intensity based on their size, shape and color depth,49–54 multiple studies have proved that no correlation exists between mark size or color depth and the applied occlusal load.45–48 (See Figure 5a.) In one bench study, as the applied occlusal forces were doubled and tripled, the articulating paper marks decreased in size.46 In another study, when the largest and darkest articulation paper mark was compared with that same tooth’s force percentage, a low etiological relationship was found between mark area (size) and force. The largest paper mark was matched with the most forceful tooth only 38.3% of time.45 The authors determined only 6% of the mark surface area could be explained by applied occlusal force, while 94% of the mark area resulted from other factors unrelated to the applied occlusal force (paper thickness, surface wet/dry, tooth morphology, and cusp angle). The authors stated that “the size of an articulation paper mark was an unreliable indicator of the applied occlusal force, that should not be used to guide treatment occlusal adjustments.”45
._the_maxillary_contact_i.jpeg)
As most implant prostheses are installed primarily with Articulating paper, which measures nothing occlusal other than contact area,59,60 damaging occlusal forces are likely left in place when implant prostheses are installed only with Articulating paper (used with or without shim stock). The unaddressed damaging high-force contacts would contribute to the high reported mechanical complication rates.1–12
To date, there are no implant prosthesis survivability and complication studies that have used the T-Scan technology at the delivery of the implant restorations, which could improve implant complication rates. As such, the purpose of this study was to compare the T-Scan 10 against Articulating paper only case insertions, to determine if computer-guided occlusal adjusting significantly reduced implant complications.
MATERIAL AND METHOD
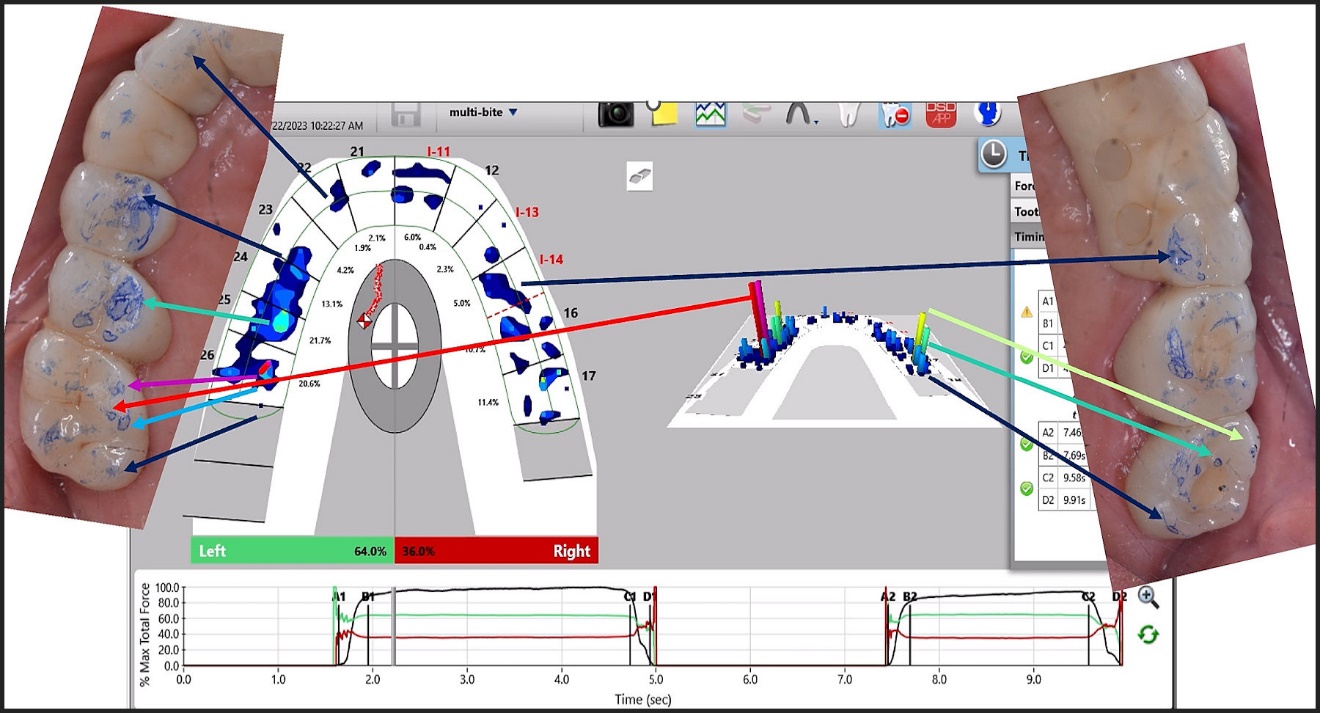
A multi-office clinical study was performed, in which the gathered data was part of each clinician’s daily implant practice procedures. Six clinicians well-trained in T-Scan implant procedures were recruited to install their single and multi-unit fixed partial denture implant cases. Alternating cases were completed using the articulating paper only method (traditional ink marking of the implant occlusion and then subjectively selecting contacts for adjustment), with the next prosthesis being installed using the T-Scan + Articulating paper computer-guided method. (See Figure 5a.) In both methods, each clinician utilized their routine occlusal adjustment marking strips/films/paper to create contact ink markings, such that the marking materials were not standardized. In the 2nd method, T-Scan recordings were made of the implant prostheses to detect high force and early occlusal contacts. Then, the isolated problem contacts were marked with clinician’s same articulating medium and targeted for adjustment determined by the computer metrics. (See Figure 5b.) Despite their clinical appearance, non-forceful ink markings were not treated so that only T-Scan-determined high-force problem contacts were adjusted.42,43

Any mechanical complications that transpired after insertion were collected in Excel Sheets (Microsoft Corp., Seattle, Washington, USA). The numbers and types of complications encountered by all clinicians were compiled for statistical analysis at 6 months, 1 year, 2 years, 2.5 years, and 3 years.
The Mechanical Complications compiled were
- Porcelain Fracture
- Metal Framework Fracture
- Abutment Fracture
- Screw Fracture
- Screw Loosening and prosthesis mobility
- Un-cementation requiring Re-cementation
- Functional pathology – Difficulty chewing with the new prosthesis
- Post-insertion repeated occlusal adjustment from a lack of patient occlusal adaptation
RESULTS
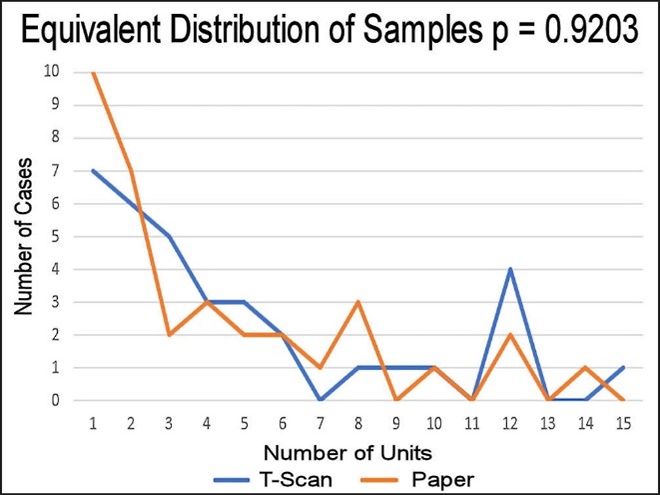
A total of 306 units were installed (143 with Articulating paper-only, and 163 with T-Scan + Articulating paper). By alternating the selection of the method used (T-Scan or paper only) a random distribution occurred, as there was no significant difference in the distribution of the types of prostheses that comprised both groups. This ensured that the numbers of single unit or multi-unit fixed prostheses per group were statistically similar (Mann-Whitney U Test p = 0.92034). (See Figure 6.)
__and_.jpeg)
The Sign Test assessed the 8 types of complications and determined significantly fewer complications occurred with the T-Scan + Articulating paper method (Table 1; p < 0.00716).
-
The complication rate for the Articulating paper-only units was 35/143 = 24.5 %.
-
The complication rate for the T-Scan + Articulating paper units was 3/163 = 1.8 %.
DISCUSSION
The findings of this implant complications study are unique, as this is the first complication study that used T-Scan to install implant restorations compared to using traditional non-digital occlusal indicators, with statistically significant differences found between the 2 methods. This study tracked complications using a subjective case insertion approach (Articulating paper-only) and a measured case insertion approach (T-Scan + Articulating paper). The results clearly indicate that using a measured method that targets problematic occlusal contact forces greatly reduced implant complications compared to occlusal adjustment using subjective interpretation of paper marks. Recently published Systematic Reviews confirmed that much scientific evidence supports use of T-Scan in dental treatment, because it measures relative occlusal contact forces and timing objectively, accurately, and repeatedly.42,43
The most frequently reported complication was screw loosening (23 times in the Articulating paper-only group; 1 time in the T-Scan + Articulating paper group), which is typically the 2nd most frequent complication following porcelain chipping.1,4,8 Screw loosening results from cyclic restoration torque under occlusal loading. Cyclic Torque results from loading a prosthesis with poor occlusal balance and non-centered occlusal forces, or from repeated lateral excursive contacts pressing the restoration off the center axis of the implants. The unbalanced occlusal forces move the restoration inwards toward any overloaded implants, and outward away from any less loaded implants. This repeating cycle slowly over time, backs some of the screws out of some of the implants. If one tightens the screws down and then they re-loosen, the torque is still present, and no amount of screw tightening will be able to counter the off-center loads that create the repeating torque.
In the Articulating paper-only group, there was no measured control over excursive contact force, nor was there any way to assess the occlusal force distribution between the right and left arch halves. The Articulating paper-only group encountered unknown occlusal forces because ink marks do not predict force levels.45–48 Whereas in the T-Scan + Articulating paper group, excursive contact duration load levels, plus the right side-to-left side overall occlusal force distribution were both measured and corrected with computer-guided occlusal adjustments, thereby lessening the torque, and hence statistically lessening the screw loosening.
The T-Scan HD Novus sensor (Tekscan, Inc., Norwood, MA USA) is a sophisticated electronic printed circuit with 2200 recording sensels (0.5 mm2 /sensel) per sensor, that accurately and repeatedly records 256 occlusal contact force levels across time from within contacting and excursing opposing teeth, without sustaining significant sensor breakdown.42,43 (See Figures 2a and b.) The 100 micron sensor thickness is a positive sensor attribute, that houses and protects the printed electronic components of the recording grid within a flexible and compressible Mylar substrate, while maintaining sensor structural integrity despite being repeatedly crushed between teeth.18–24,42,43 When combined with the T-Scan 10 analysis software, a clinician can accurately isolate and target excessively forceful contacts that potentially create mechanical complications on implant restorations.
Studies repeatedly show when occlusal adjustments are based on the Subjective Interpretation of paper mark color depth, and size, frequent incorrect contact selection occurs,55–58 because paper mark size and color depth do not depict a contact’s occlusal force content.45–48 (See Figure 5a.) When occlusal contact force diagnostic errors are made, incorrect contacts will be selected for occlusal adjustment, which likely contributes to untoward mechanical implant complications. Further, the removal of occlusal veneering materials from areas on implant restorations that do not need occlusal force reduction will weaken the veneer material, leading to early material failure and shortening the lifespan of the prosthesis.
Most importantly, subjective occlusal adjusting creates the very real possibility that the adjustments did not treat the true areas of excess occlusal force, because the paper marks did not appear to be “forceful looking.” An example of this can be seen in Figure 5b, where the highest force contacts were 2 small markings on the left 1st molar palatal cusp. Whereas the very large left premolar ink markings were measured as low and moderate force contacts. If the 1st molar palatal cusp is not treated because the ink marks are “small” and “light”, excess force will be left on the implant restoration. Then, ongoing localized, cyclically repeating, high occlusal force will overload the 1st molar. This could lead to the screw loosening observed in the Articulating paper-only subjective group.
Alternatively, the occlusal force data from T-Scan 10 precisely identified where the excessively forceful contacts were located. (See Figure 5b.) Then these specific contacts can be targeted objectively, while any low force occlusal contacts are left untreated, regardless of how the ink marks appear. In this specific study, employing a non-subjective (objective) quantifying occlusal indicator (T-Scan 10) to guide the selection of implant contacts for occlusal adjustment produced statistically fewer complications. This computer-guided method is minimally invasive, whereas the Subjective Interpretation of paper marks is more invasive because frequently, clinicians subjectively choose the wrong contacts.55–58
In this era of the Digital Workflow, when Implant Prosthodontics is seeking high precision prosthesis-driven implant placements, and CAD/CAM milled prostheses are machined to very high tolerances, that clinicians are Subjectively Interpreting articulating paper marks to adjust the final phase of implant prosthesis construction (as if it is a valid approach to manage occlusal forces), seems wholeheartedly counterproductive. Studies show the Subjective Interpretation of ink markings method is tantamount to “guessing poorly” when dentists choose contacts.55–58 Further, what is being “measured” by the ink marks is only contact area; not occlusal force levels, timing, or occlusal balance. Therefore, it is in Dental Medicine’s best interest to recognize that Subjective Interpretation is a highly flawed, and problem-causing method, because it lacks true measurements of occlusal function, and only marks the contacts with ink.
Instead, clinicians should perform occlusal adjustments by using the Articulating paper solely to ink mark the contacts and use the T-Scan 10 data to accurately determine the true problem occlusal contacts for adjustment. As this study illustrated, combining T-Scan data with Articulating paper is a statistically better method, that will likely improve the survivability of many implant restorations for many implant patients and practitioners.
LIMITATIONS
Despite there being multiple practitioners reporting on their complications, there were low numbers of complications compared to levels reported in other studies. These clinicians are leaders in implant prosthodontics, with high level clinical skills when installing their cases.
The sequentially alternating implant restoration insertion procedure helped to standardize and equalize the use of the 2 insertion methods, but the numbers of reported implant units varied by practitioner, as not all clinicians installed equal numbers of implant units. To counter this clinician case number variability, all units per insertion method were totaled, regardless of prosthesis size and unit numbers, and a long-term period of complication observation was employed (3 years).
Another possible limitation was that the calibrated T-Scan clinicians made all the recordings and performed all the implant adjustments on all their own implant prostheses. Different clinicians would be expected to produce somewhat different occlusal force distribution and timing outcomes, rather than obtaining exactly the same occlusal end-result per implant case. T-Scan treatment end-result precision depends on the skill of the clinician working with T-Scan force and timing dynamic datasets. Varying T-Scan skills per clinician could affect the complication rates of the different clinicians. However, the low numbers of complications seen with the T-Scan + Articulating paper method indicated that calibrating the clinicians in T-Scan competency minimized the clinician variability. Therefore, this study’s results may not be representative of all outcomes by all clinicians, who may practice without undergoing definitive proper T-Scan training and T-Scan coursework.
CONCLUSION
Over a 3-year period of observation, employing the T-Scan + Articulating paper method at implant case insertion statistically lessened the mechanical complication rate in differing fixed-in-place implant restorations, compared to using the Articulating paper-only method. Improving the Standard of Care in Implant Occlusion requires recognizing that Subjective Interpretation is a highly flawed, and problem-causing method that should be replaced with a measured occlusal adjustment method; one where Articulating paper solely ink marks the contact locations, but that the occlusal analysis and adjustments of problematic occlusal contacts is performed computer-guided.
DISCLOSURE
The statistician, Mr. John Radke, is the Chairman of the Board of Bioresearch Associates, Inc., Milwaukee, WI, USA.