Background
Many authors have hypothesized that Somatic Symptom Disorder (SSD) is an etiology of temporomandibular disorders (TMDs) due to underlying psychosocial distress. The most prolific taxonomic classification, the RDC/TMD and its recently updated version, the DC/TMD, are heavily dependent upon this assumption under the so-called biopsychosocial paradigm. However, while there is no doubt that the psychosocial and emotional distress associated with pain interfere with patients’ perceptions of their own symptoms, the assumption that TMD is a form of SSD is sorely lacking in empirical evidence.
Introduction
Temporomandibular Disorders (TMDs) are a category of at least 40 distinct conditions negatively affecting the function of the stomatognathic system.1 Many TMD conditions include internal derangements of the articulating disc within the temporomandibular joint that is often followed by degenerative changes in the joint.2,3 The degenerative progression is most strongly related to disc displacement without reduction.4 Some studies have found that TMDs are likely to result from the partial or complete loss of molar dentition causing mainly muscular symptoms (orofacial pain).5–7 Others have found that occlusal interferences to function can precipitate TMDs,8–11 while divergent studies have been unable to find any etiologic relationship with occlusal variables,12 especially within short-term and pilot studies.13 A separate skeletal structural issue related to the masticatory system is Angle’s occlusal classifications. There is some support for the premise that Class II occlusal arrangements have a greater propensity toward developing substantial TMDs symptoms.14
Congenital conditions such a cleft lip and cleft palate have been shown to reduce the quality of life and masticatory function even after treatment.15 Ehlers-Danlos syndrome is another genic disorder that increases the propensity toward developing TMDs.16 One recent study concluded that single-nucleotide polymorphisms can aid or abet the development of TMDs after orthognathic surgery.17 Abnormal growth and development have also been identified as contributors to TMDs conditions. Bacterial infections have been found to be significantly more prevalent in TMDs patients than in healthy subjects.18–21
Psychoneuroimmunology has theorized that emotional stress can be either an etiologic factor or an exacerbating factor in precipitating or perpetuating TMD and chronic orofacial painful conditions.22–24 Somatization, recently renamed as Somatic Symptom Disorder (SSD), has been proposed as a primary etiology of at least some TMDs and orofacial pains.25 The Research Diagnostic Criteria (RDC/TMD),26 in Axis II, has recommended the Beck Depression Inventory-II to measure depression and the subscale of the SCL-90 to evaluate somatization.27 However, it is common knowledge that SSD cannot be distinguished just by symptoms from underlying physical disease because they share the same symptoms. It was stated in the RDC/TMD that the SCL-90 does not measure somatization. In fact, psychiatry understands very well that all possible physical sources of symptomology must be disavowed before testing for SSD is likely to be efficacious.
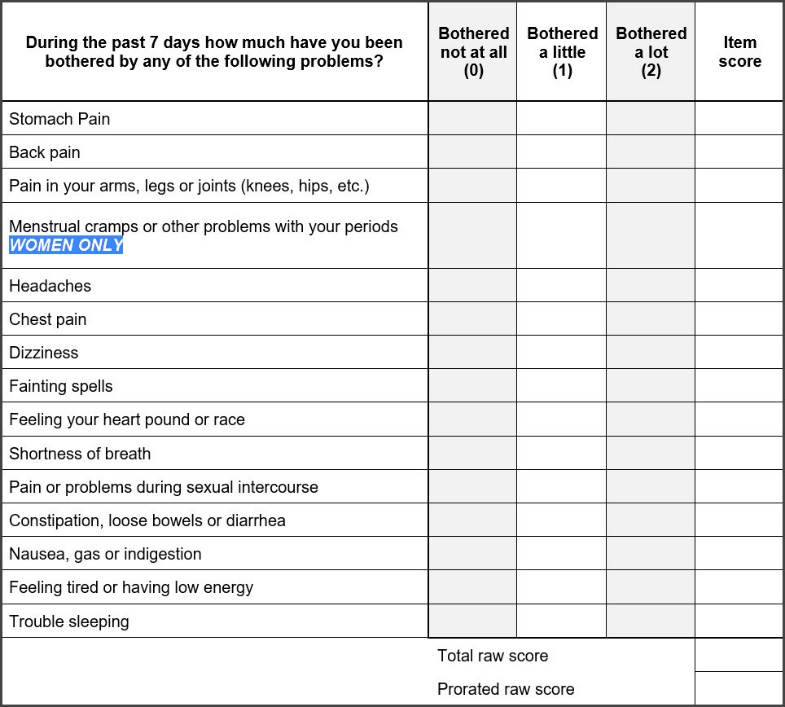
The Patient Health Questionnaire-15 (PHQ-15), validated by testing a large normal population, is a fifteen-question anamnestic instrument used by many psychiatrists and psychologists to evaluate SSD in the absence of a detectible indication of physical etiologic symptoms.28 See Figure 1.

Each question is supplied with three possible answers; 1) not bothered at all, 2) bothered a little, or 3) bothered a lot (during the past 7 days). The totaled score ranges from 0 to a maximum of 30. Normative scores across the population are generally less than 5 and increase gradually with age.
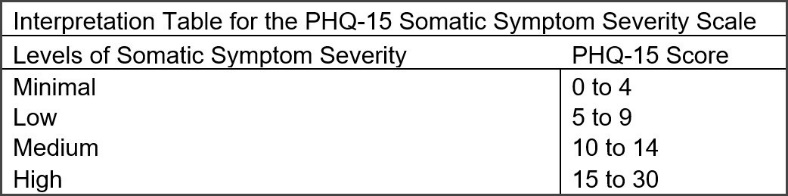
Moderate SSD is indicated by scores from 10 to 14, while a score of 15 indicates a percentile rank between 92.8 and 99.7.28 Higher scores = higher probability. See Figure 2.

With so many factors potentially contributing to TMDs it is not surprising that controversy has been the most common overall result of TMDs research. A previous study utilizing the Beck Depression Inventory-II compared depression scores from TMDs subjects pre to post successful physical treatment. While most of the subjects had exhibited moderate to severe depression pre-treatment, successful physical treatment reduced all of their levels to within normal limits, removing depression by itself as a potential etiologic factor for the group.29
Objectives
The objectives of this research were; 1) to evaluate whether the PHQ-15 might be diagnostically valuable even prior to any physical treatment of the many different types of TMD conditions and 2) to assess the amount of change in the “somatization scores” between the pre and post treatment states. The Null hypothesis = No change in PHQ-15 scores after physical treatments that reduce symptomology.
Methods
For this study six private practices specializing in the treatment of TMDs patients were recruited from four countries (U.S.A. Mexico, Brazil and India). Two of the practices (PT & BS) focused specifically on treatment of TMDs patients without serious TMJ involvement, which might be as well described as Orofacial Pain due to a preponderance of orofacial, painful, muscular symptoms and an absence of TMJ pain. Their treatments were limited to adjusting the occlusion using a well-established protocol for the T-Scan (Tekscan, Inc. South Boston, MA USA) commonly referred to as Immediate Complete Anterior Guidance Development (ICAGD).30–37
The other four practices were focused on arthrogenous TMD patients, most of whom had some stage of Internal Derangements of the TMJ from relatively acute to end-stage chronic conditions. Their treatment methods were varied and included the individualized application of ULF-TENS, orthotics, NSAIDs, exercises and in some cases orthodontics and/or prosthodontics for the final restoration of normal function.38–42 These four private practices were dissimilar, geographically separated and not linked in any manner with separate treatment philosophies and methods. This was intentional to include a variety of treatment methods from a non-uniform group of practitioners.
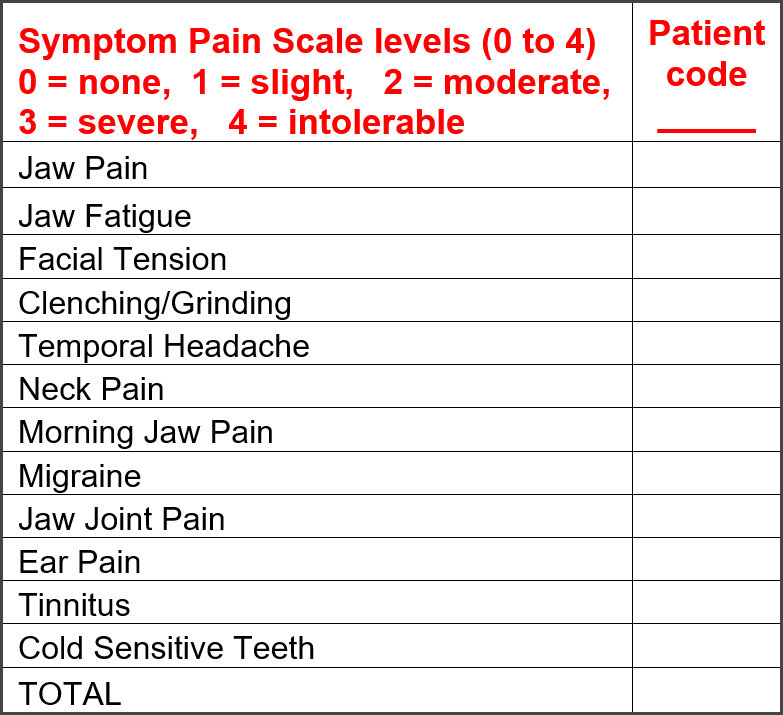
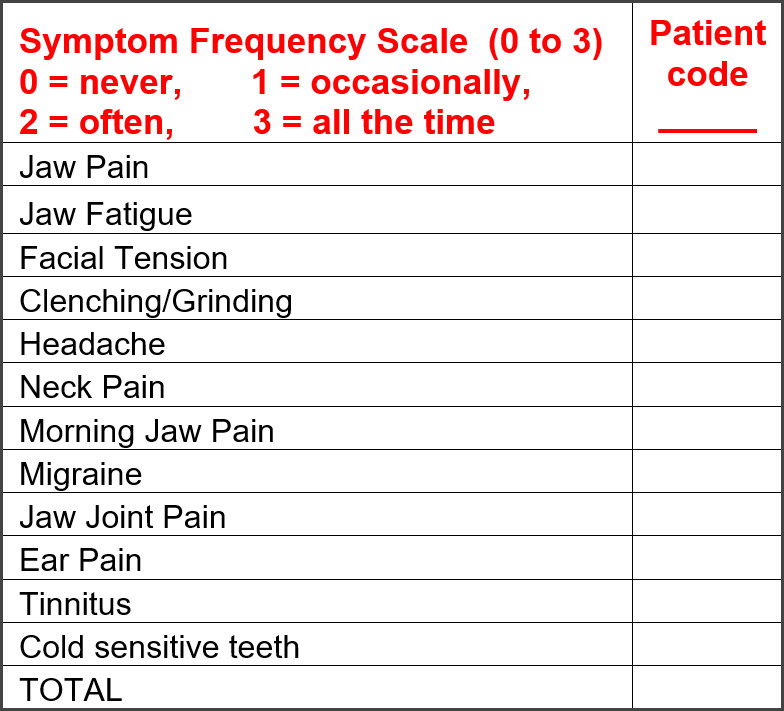
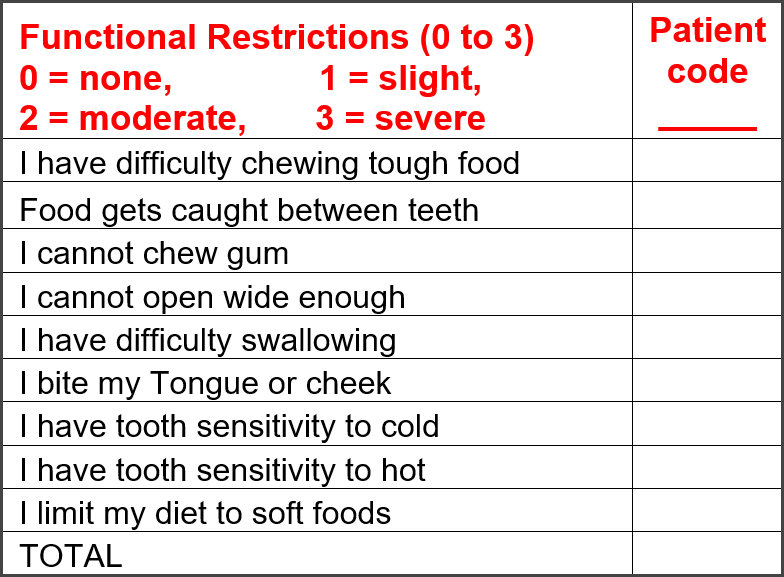
To document the symptom levels prior to treatment each practice agreed to an anamnestic survey of each patient’s Pain Intensity, Symptom Frequency and Functional Restrictions. See Figures 3 to 5. The questions used were taken from popular symptom surveys (RDC/TMD). After each patient had signed informed consent and agreed to treatment, they were also given the PHQ-15 instrument to respond to. All four of these anamnestic instruments were re-utilized approximately 3 weeks after initiation of treatment and at 3 to 4 months post-treatment at a follow-up appointment.



All patients were recorded pre-treatment, post-treatment and at follow-up with Joint Vibration Analysis (JVA) to evaluate TMJ function.43–57 At the same appointments masticatory function was also assessed with combined Electrognathography (EGN) and electromyography (EMG) recordings of gum chewing.58–69
This was done to evaluate; 1) the function of the TMJ and 2) the quality of mastication of a soft bolus using BioPAK software (BioResearch Associates, Inc. Milwaukee, WI USA). The recordings were repeated at each appointment and at the follow-up appointments. These data will be reported on at a later time.
For the purpose of this report, the only data analyzed were subjective reports from the patients. Consequently, the Wilcoxon Sighed-Rank test was selected for the strictly intra-patient comparisons, making each subject his or her own control. No separate control group was enlisted due to the treatment efficacy focus of this protocol and the fact that somatization was the key factor in question. Alpha = 0.05.
A total of 82 patients participated, 61 females and 21 males at a ratio of 2.9:1. The mean age was 43.4 (+/- 17.2) years with a range from 14 to 76 years and a median of 42. While the distribution is not a normal one, it does represent the entire range of likely candidates. This is a little older group than many previous TMD studies, which have had their mean ages in the mid to late 30s. Patients were selected sequentially as they agreed to participate. Although not a random process it fairly represents the TMD population both for patients with TMJ involvement (43) and those without TMJ involvement (39). An IRB Exemption for this study # BIRB/100Z/2019 was received.
Results
Significant improvements were observed in all symptom categories. Total pain intensity scores were extracted from the Symptom Pain Scale levels that were reported pre-treatment, 3 weeks post treatment and again at 3 – 4 months post treatment. See Table 1.
In addition to their recording pain scores, each patient was required to record the frequency of their symptoms, which was tracked prior to and throughout treatment. See Table 2.
The group’s Functional Restriction median scores were also significantly reduced by the treatments. See Table 3.
The PHQ-15 scores were reduced significantly after all the treatments were provided and continued to significantly reduce 3 – 4 months later at the follow-up appointments. See Table 4.
A comparison of the results of treatment between the two groups manifesting either; 1) occluso-muscular or 2) TMJ internal derangement symptoms is shown in Table 5. Those cases that had primary occluso-muscle symptoms and no substantial involvement of the TMJ had their Disclusion Times Reduced (DTR) with (ICAGD) Immediate Complete Anterior Guidance Development.29–32 The TMD subjects with substantial TMJ involvement (Internal Derangements) were treated with orthotics, TENS, NSAIDs, exercises and other commonly applied methods. Most of these primarily arthogenous patients also had secondary muscular pain complaints that were significantly reduced by treatment as well. It can be seen from this comparison that the orofacial pain patients responded more quickly and to a greater extent within 3 weeks and at the 3 to 4 months timepoint.
Discussion
TMD and orofacial pains that are associated with occluso-muscular TMD symptoms have previously been shown to be significantly reduced up to five years and longer after ICAGD treatment.70,71 However, these changes do not occur instantaneously, but require some period of time for full recovery. Treatment by appliance also requires six to twelve months to complete recovery.72 This time is required for healing, especially in avascular tissues such as the TMJ with slow metabolite infusion.73 A period of up to six months to successfully reduce painful symptoms in TMD cases is commonly observed. This suggests that attempting to measure SSD in TMD patients prior to any physical treatment would most often produce a false positive SSD indication due to the established, treatable TMD physical etiologies. Pain is purely subjective and the etiology can only be determined if the pain can be relieved by some physical change. Removing the pain pharmacologically does not reveal the etiology, but masks it. Based upon the results of this investigation we reject our null hypothesis of no significant change in PHQ-15 scores.
The Symptom Frequency scores improved significantly after treatment and continued to improve significantly even up to the follow-up appointment three to four months later. This supports the concept that the group responded to all the treatments by reducing the frequency of their symptoms significantly, but symptom reduction is not instantaneous. It took 3 – 4 months for the symptom frequencies to completely subside after the physical treatments, which is a common finding in many TMD treatment studies.74,75
The goal of evaluating functional restrictions is to reveal whether the subject is experiencing difficulty chewing, swallowing, has excessive tooth sensitivity or has been avoiding any tough foods. Although the term functional restriction is often applied just to a limited range of motion, it would be a more appropriate indicator if applied to masticatory capacity. When capacity is only based upon the subjective reporting from the patient, it is a weaker measure than when an objective method is used.76 However, even the subjective indications of reduced functional restriction in this group were highly significant at the three to four months timepoint for both groups.
Likewise, the PHQ-15 scores followed the same pattern as all the symptom scores, starting with a high pre-treatment median score of 10 (58% > 10). See Table 4. This suggests that testing for SSD prior to any physical treatment would have falsely identified 58 % of the group with a medium degree of somatization.25–28 However, the scores decreased significantly until at the three to four-month timepoint they reached a median score of 4 (only 11% remained > 10). The seven subjects scoring highest at the three to four months timepoint started with a median Pain score of 27 and ended with a median Pain score of 15. It is likely that additional time will be needed to further resolve those difficult cases.
Since the cases were identified as either; a) occluso-muscular TMD/orofacial pain, without any serious TMJ internal derangements or b) as arthrogenous TMD, with definitive internal derangement, it was possible to evaluate the two outcomes separately. See Table 5. These analyses suggest that arthrogenous TMD cases may be more difficult to treat successfully or may require a longer recovery time post treatment than the occluso-muscular cases. Since each groups’ symptoms differed (with or without substantial TMJ involvement) it is reasonable that their responses were different. In both types of TMD cases, any attempt to evaluate for a Somatic contribution to the symptomology must wait until after maximum medical improvement has been achieved. Otherwise, the presence and/or extent of any Somatic Symptom Disorder may be grossly overestimated.
Comparing one obvious difference between the 2 methods of treatment, the ICAGD is focused on the occlusion, specifically occlusal interferences to masticatory function, while the orthotic approach is focused on correcting the maxillo-mandibular mal-relationship. From the data in this study, it appears that these two conditions can instigate both muscular and arthogenous TMD symptoms. In the latter case, adding the ICAGD focus on the occlusion may have further improved the outcome.
Limitations
While the ICAGD treatments are standardized and have been successfully reported from different practitioners in previous studies,33,35–37 the other four practices providing orthotic-based treatments were quite diverse and the patient populations included TMJ internal derangements that may be more complicated to treat. Since this study focused on treatment outcomes with the subjects only being compared to themselves, no control or placebo group was included. This was also the design because it can be very difficult to maintain an active placebo treatment for several months, especially for TMD subjects.
Conclusions
Since the PHQ-15 median score of this group of TMD subjects dropped from 10 (medium SSD) to 4 (normal) after physical treatments, a premature attempt to test for SSD using PHQ-15 would have misclassified 58 % of the group as medium level SSD. At the three to four months timepoint 11% were still scoring at a medium level of SSD, but difficult TMD cases may need a longer period to be fully resolved. The fact that even these resistant cases had significantly reduced their scores from a median of 20 to a median of 14 (p = 0.0116) suggests that they had physical etiologies that responded to the physical treatments.
It is clear that with both types of TMDs cases, any attempt to evaluate a patient for SSD must wait until after maximum medical improvement has been achieved. The use of the PHQ-15 or any similar instrument as an initial diagnostic tool is not justified. These results also support the concept that uncontrolled structural and functional factors such as arthrogenous and occluso-muscular TMD/orofacial pain can contribute substantially to the onset of a faux-SSD. For all of the reasons stated above the null hypothesis was rejected.
Clinical Significance
The data in this report supports the theory that the diversity of TMD symptoms can best be explained as predominantly due to untreated physical problems, not any psychosocial etiology. While occluso-muscular TMD responds quickly to ICAGD treatment, the symptoms continue to reduce for at least 3 – 4 months post-treatment. When correcting a maxillo-mandibular mal-relationship, some added attention to the end-point of occlusion is usually indicated. These concepts will be elaborated upon in Part II.
Post script - Behavioral & Social Sciences Summit: In October 2020 the Behavioral, Epidemiologic and Health Services Special Interest Group of the International Association for Dental Research sponsored a Summit with the purpose of arriving at a consensus statement on the future directions for the behavioral and social sciences in oral health. See https://www.bsohsummit2020.com/ for the Summit details. The consensus suggestions included:
-
Behavioral and social factors are critical interactive determinants of dental, oral and craniofacial health including gender, race and socioeconomic status, but simpler more testable theories are needed.
-
Use of multiple and novel methodologies in social and behavioral research and practice related to oral health is needed in order to determine oral health: Adoption of methods for testing theories related to the cognitive, affective, and motivational basis of behavior.
-
Development and testing of behavioral and social interventions are needed to promote oral health for racialized and ethnicized groups, refugees, rural populations, people with disabilities, those with low income and low literacy, and others who are minoritized or marginalized.
-
New dissemination and implementation research for oral health will be required to achieve optimal oral health globally. Impactful dissemination and implementation (D & I) research in oral health will prioritize meaningful involvement of stakeholders, consideration of global and local context, contemporary study designs, characterization of causal mechanisms, and precisely specified and high-quality methods.
All of these suggestions are generalized in character with no specific agenda or design for implementation. While patient behavior is certainly important in self-care and thus prevention, no indication how psychological therapy can effectively treat dental, oral or craniofacial diseases and disorders is mentioned. This consensus does not at all acknowledge that oral diseases and disorders routinely have physical etiologies that must be corrected before applying psychological therapy as has been recognized by Psychiatry in Medicine.77
Declaration of conflicts statement
John Radke is the Chairman of the Board of BioResearch Associates, Inc. All other authors reported no potential conflict of interest.
Funding Statement
No funding of any kind was received in support of this research activity.