INTRODUCTION
Temporomandibular Disorders (TMDs) often appear to be complicated multifactorial conditions that may include disease but most often include only dysfunctions. A simplistic approach to categorization suggests that there are four types of TMDs, 1) muscular, 2) arthrogenous, 3) Somatic Symptom Disorder (SSD), and 4) combined.1,2 When muscles are hypersensitive to palpation in patients with no concurrent indications of TMJ involvement, muscular TMDs are often presumed. Joint noises, joint pain on palpation, limited and/or a deviant opening/closing pattern are the clinical indications of an arthrogenous TMD.3 When no physical etiologies are found to be present, (less than 1 % of the time),4 a diagnosis of SSD is possible. Somatic symptoms are often present with TMDs, but most often they are secondary to physical etiologies.
The diagnostic process should always begin with a medical history and proceed with a clinical examination. Internal derangements and other conditions of the temporomandibular joints (TMJ) have been reliably documented for several decades using every available imaging technology to improve on the documented inaccuracies of clinical examination techniques.5 Muscle function can be evaluated with electromyography, and deviant jaw motions may be recorded with jaw trackers resulting in objective data.
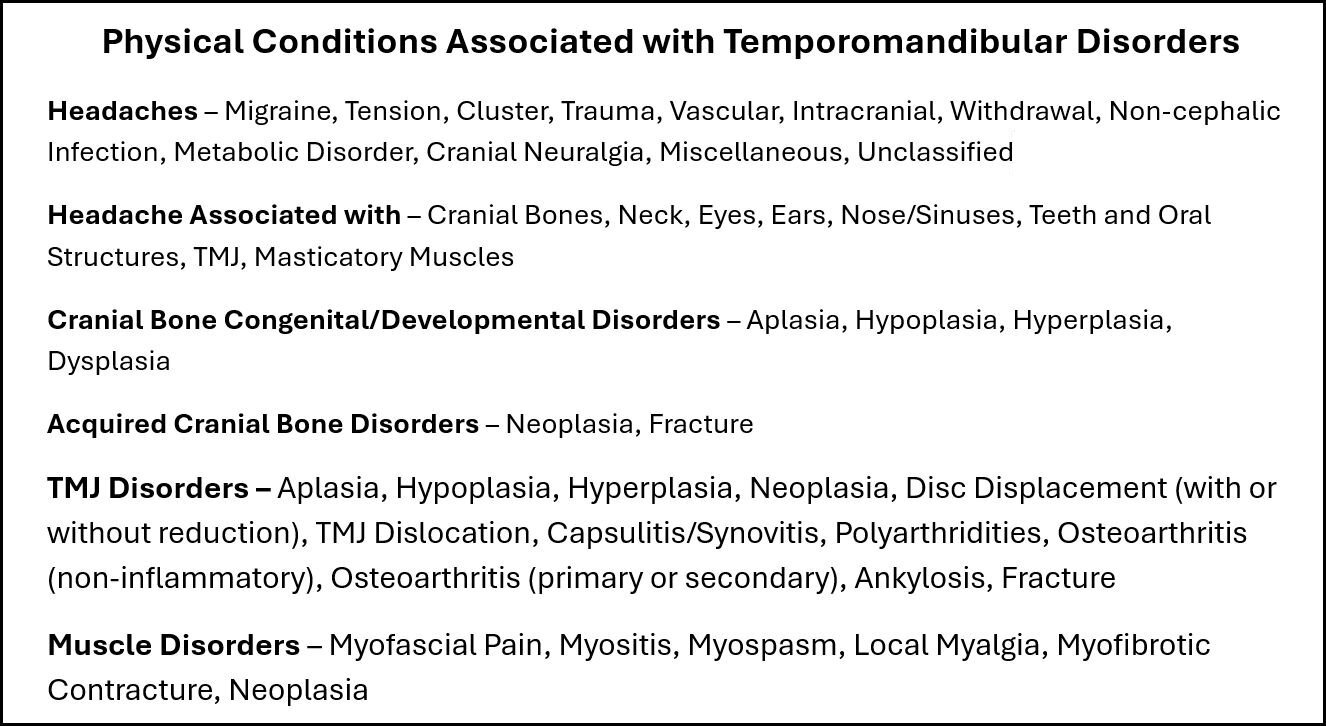
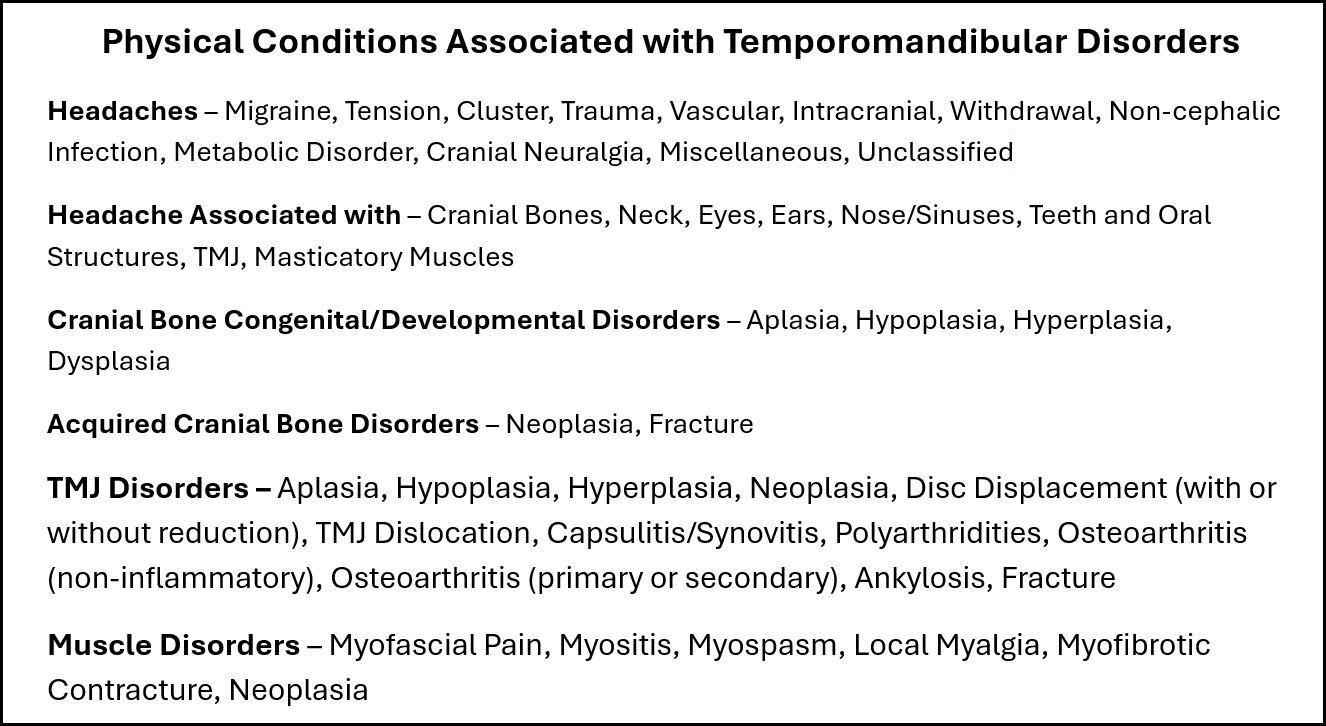
The category “TMDs” was created in 1982 to represent an umbrella term over all stomatognathic system disorders and has been previously described to encompass around forty different discernable physical conditions when a comprehensive diagnostic evaluation is undertaken.1 See Figure 1. In recent years some additional physical conditions such as Sleep Apnea, Trigeminal Neuralgia and Meniere’s Disease have been added to the list of probable TMDs.
While some TMDs include several factors, (multifactorial), other TMDs clearly respond very positively to a single efficacious treatment, suggesting that those TMDs are more likely unifactorial. The consensus among TMDs treatment providers is that no single etiology is universal to all TMDs and no single treatment is equally efficacious for relieving all TMDs cases. Therefore, it is essential to determine the etiology(s) present before the TMD treatment provider can select an efficacious treatment.
The stomatognathic system is very complex, highly innervated by seven of the twelve cranial nerves and the masticatory system is the most precisely controlled organ of all motile bodily functions. Consequently, it is highly sensitive to even minute disturbances. A nanometer-sized particle between occluding tooth surfaces can be very disruptive. Consider that something as innocuous as a slightly high filling or crown can very quickly initiate TMDs-like symptoms.6–8 It has also been shown previously that a structural disturbance in one part of the body can affect multiple other parts including the phenomenon of referred pain.9
The protocol for “pain management” of TMDs
The PM protocol limits treatment of all TMDs to “pain management” irrespective of the patient’s physical conditions.6 The TMDs patient’s painful complaints are corroborated with a clinical examination and palliative, or behavioral treatments are usually considered appropriate. Those who utilize this approach expect that TMDs are usually multifactorial, complex, never fully curable and that the only course of action for the practitioner is to make the patient as comfortable as possible by attempting to reduce their pain complaints.10 This belief relieves the practitioner of the responsibility for accurately diagnosing any specific etiologies presently causing the symptoms in TMDs patients.11 The PM view of TMDs is defined by a “painful-symptoms-based” diagnosis along with the presumption that their etiologies are either too vague or unknowable.12 Since a majority of TMDs patients’ complaints do surround discomfort, the reduction of pain is the objective pursued while biological contributing factors may be ignored or only noted.11 Any slight improvement in the patient’s pain complaints or ability to cope with their pain is considered as a success, but complete remission of all painful symptoms is neither expected nor pursued. The following conclusion epitomizes the beliefs of those adhering to the treatment of TMDs with pain management, “There was no superiority of multimodal therapy including splints as compared with simple care.”13
The presence of mild to severe depression and anxiety have been very well documented within TMDs patient populations.14–16 According to Türp et al, “Patients with widespread pain who indicated pain locations in any one or more of the extremities plus the lower back scored significantly higher on the Pain Disability Index (PDI) and the Beck Depression Inventory (BDI) than patients with no such combined involvement.”17 They found that the PDI and the BDI both increased in severity with the greater extent of the pain distribution.
The pain management approach usually suggests incorporating psychosocial testing for the presence of depression, somatization, catastrophizing, and anxiety during the initial diagnostic examination (E.g., PHQ-15, PHQ-9, GAD-7, BDI, etc.).16,18 However, according to psychiatry it is not possible to differentiate physiologically based painful symptoms from somatic pain symptoms.19 A headache due to muscle tension or stress is still just a headache to the patient. This is why psychiatry requires a nullification of any possible biologic etiology before a diagnosis of Somatic Symptom Disorder (SSD) can be confirmed. “True somatization disorder is very rare (< 1%) and requires a DSM-III-R diagnosis of at least 13 different physical symptoms which cannot be explained by, or are in gross excess of physical findings, and have caused the patients to seek health care or alter their lifestyles.”4 Note: It seems highly inappropriate for dentists that are not trained in psychiatry to be attempting to diagnose Somatic Symptom Disorders (SSDs), especially since no physical diagnosis is usually considered necessary for PM palliative treatments.
One of the recommendations for TMDs treatment from those using the pain management protocol is that only reversible treatments should be considered.6,20,21 It is rationalized that reversible treatments have the advantage that they can be withdrawn if they are ineffective or worsen the patients’ conditions, causing “chronification.” This suggests that their lack of focus on the detection of the underlying etiologies in TMDs patients generally leads to a trial-and-error approach to treatment, which makes reversibility almost a necessity. Utilizing the PM protocol may include prescribing NSAIDS, heat, cold, a temporary flat-plane appliance, or Cognitive Behavioral Therapy (CBT), but avoids making any permanent correction to the biology of the stomatognathic system. However, oral appliances like the Michigan splint, which are claimed to be reversible, have been shown to cause changes in the bite whether they are temporarily effective or not.22
Since the PM protocol does not require a biological diagnosis, all decision-making is based solely upon the health history and the patient’s subjective report of symptoms during examination.6 While this greatly simplifies the diagnostic process it limits the information available upon which to select the best potential treatment. This protocol also implies that a "one-size-fits-all" approach to treatment may be possible and can encourage the establishment of a “usual” or “standard” routine trial & error treatment sequence that is applied to every new TMDs patient. E.g., NSAIDS and soft food, a muscle relaxant, self-treatment consisting of muscle exercises, a hot pack, a cold pack, or in some cases a Michigan (flat-plane) splint after nothing else relieves the painful symptoms.6 When there is minimal response to these “standard/usual treatments,” Cognitive Behavioral Therapy may be initiated after the production of a false-positive diagnosis of Somatic Symptom Disorder using the Patent Health Questionnaire (PHQ-15, PHQ-9) or PDI. The conclusion that a patient suffers from a SSD conveniently removes the onus of failure associated with the patent’s lack of a sufficient response to palliative and reversible physical treatments.
The PM protocol for the management of TMDs does not value imaging since the information gained from MRIs and CBCTs is only descriptive of the current morphology and the damage to the structures involved. Diseased and chronically damaged joints are painful when active infections are present, but not when successful adaptation is present. The PM protocol assumes “no pain no problem.” Because the promoters of PM appear to be very concerned about the cost of imaging for patients, they require a practitioner to 1) anticipate in advance what any specific image will contribute to the diagnosis and/or 2) a treatment’s success before it should be prescribed.6 This is a very unrealistic expectation devoid of common sense.
Masticatory function has never been considered important within the PM protocol, even when the patient relates chewing complaints. Jaw Tracking motion and EMG muscle activity patterns of chewing are not considered important within general dentistry,5 even though the combined recordings of jaw motion and muscle activity represent the best objective measured analysis that elucidates the real extent of physical masticatory dysfunction and disability.23–27
The Neuromatrix Model of Pain theory
The PM approach to TMDs diagnosis and treatment appears to accept the Neuromatrix Model of Pain, which presumes that pain is “generated” within the central nervous system rather than being interpreted from signals coming from sensors at the site of a trauma or a biological dysfunction. The model offers a weak explanation for phantom pains and pains of unknown origin but does not account for the Gate Theory of Melzack and Wall, which has demonstrated that pain signals can be blocked electrically in the periphery using TENS.28 That should not be possible if the Neuromatrix Model of Pain theory was true.
The protocol for treatment of TMDs that focuses on correcting Musculo-skeletal Dysfunctions
The more effective alternative approach to pain management of TMDs requires a comprehensive diagnosis especially for multifactorial cases.1,29,30 It presumes that for every TMDs patient there is a primary biological etiology and at times one or more secondary biological etiologies, producing true multifactorial cases. The use of this concept has led to 1) a better understanding of what the biological etiologic factors are, 2) has allowed practitioners to focus on correcting them, and 3) has increased the probability of the total remission of many TMDs patients’ symptoms. Consequently, the achievement of Maximum Medical Improvement (MMI) relies on obtaining an accurate and comprehensive diagnosis and using that information to develop an efficacious corrective physical treatment plan. Without developing an accurate comprehensive diagnosis, the probability of complete remission is greatly diminished.
Coincidentally, the correction of physical etiologic factors has had the additional benefit of consistently relieving TMDs patients’ emotional symptoms such as depression31 and reducing the number of false diagnoses of Somatic Symptom Disorders.32 This secondary phenomenon of the relief of depression and apparent somatic symptoms supports the contention that the emotional symptoms commonly associated with TMDs are secondary to and not etiologic of TMDs. It has been established that as TMD pain increases somatic symptoms increase and that as TMD pain decreases the apparent somatic symptoms decrease.33
The well documented association between chronic TMDs pain and apparent somatic symptoms34,35 may be interpreted in several ways: 1) somatic symptoms drive chronic pain, 2) chronic pain drives somatic symptoms, 3) Chronic pain and somatization mutually interact, or 4) the association is only coincidental. While previous studies have demonstrated that successful reduction of TMDs chronic pain dramatically reduces somatic symptoms32 and depression,31 no study has demonstrated that using CBT is effective for the elimination of chronic pain, only that it may improve the coping skills of TMDs patients still suffering in chronic pain.36,37 Since the assessment of painful symptoms relies upon subjective reports from patients, improved coping skills could lead to fewer or milder reported complaints. Thus, it confounds the possibility of determining whether any real change has occurred in the pain levels of TMDs patients.
The objective of the MSD protocol is to minimize or eliminate the painful symptoms of TMDs by achieving maximum medical improvement (MMI). This is accomplished after the physical etiologies driving the TMDs conditions are identified and treated successfully. The structural etiologies that the MSD protocol reveals fall into three broad categories 1) occlusal factors, 2) TMJ factors and 3) maxillo-mandibular mal-relationship factors. There is vast support in the literature for each of these factors in the form of successful treatment studies at sufficiently high success rates that cannot be attributed to a placebo effect.
Occlusal Factors
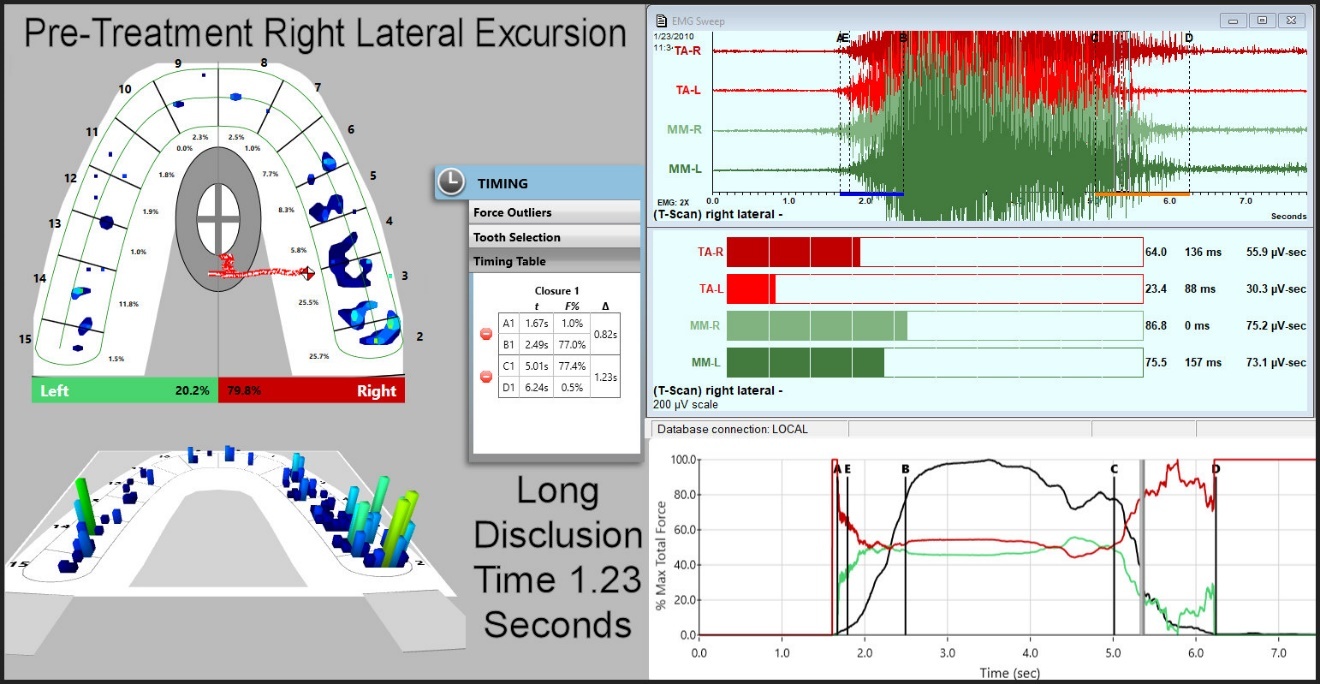
The most effective treatment of Musculo-occlusal TMDs (patients with painful muscles, normal TMJ function and with an acceptable maxillo-mandibular relationship) has been performed using the T-Scan (Tekscan, Inc., South Boston, USA) synchronized with BioEMG III (Bioresearch Associates, Inc. Milwaukee, WI USA).38 Recording T-Scan force and timing together with the EMG activity of the anterior temporalis and masseter muscles has enabled the precise identification and efficacious occlusal correction of functionally interfering contacts.39–47 Without the use of T-Scan/EMG the accurate identification of real functionally interfering posterior occlusal contacts just by using articulating paper, foils, or silk ribbons has a very low probability.48–53
Disclusion Time Reduction (DTR) is a T-Scan/EMG data driven technique that measures the time required by the patient to discluding their posterior molar and premolars during a lateral excursion. See Figure 2. Although lateral excursive motions are analogous to “walking backward” compared to the path of closure during mastication, they reveal the same interfering contacts. When interfering contacts exist, they impede the excursion either by contact or by requiring avoidance, increasing the time of closure during mastication. After the removal of interfering contacts, the disclusion time is targeted to less than 0.5 seconds and the closing time during mastication is also measurably reduced.23–26,54
__posteri.jpeg)
The classic TMDs symptoms of occlusal interferences are painful muscles with the absence of myopathy or neuropathy and may or may not include acceptably normal TMJ function. Historically many occlusal appliances have been successfully prescribed to reduce orofacial pain symptoms, which simply disengage the occlusion, but only temporarily remove the underlying problem of interfering occlusal contacts.55 While an appliance can be effective for muscular pain reduction, it tends to mask rather than reveal precisely the primary etiology of interfering occlusal contacts. One negative of splint treatments is they may require a “phase II” permanent solution using orthodontics or prosthodontics to achieve a permanent solution. Is occlusal adjustment 100 % effective for all TMDs patients? Remember that TMDs can be multifactorial with multiple etiologies overlapping. When malocclusion is secondary to other etiological factors, DTR cannot be expected to provide a complete resolution of all symptoms.
TMJ Factors
Internal derangements of the TMJs, either full or partial, are common (affecting up to 80 % of TMDs patients) and may reduce upon opening or remain permanently displaced.56–58 In most cases reducing disc displacements are noisy, but permanent disc displacements are quiet unless they become degenerative. The effects of internal derangements are variable because of the differences in adaptability between patients. Some patients succeed in adapting to an internal derangement after a few years and regain good masticatory function, but many patients do not.59 Because the occlusion is a very precise relationship, a relatively small change in the TMJ can alter the occlusion enough to affect the musculature, especially when it is unilateral.
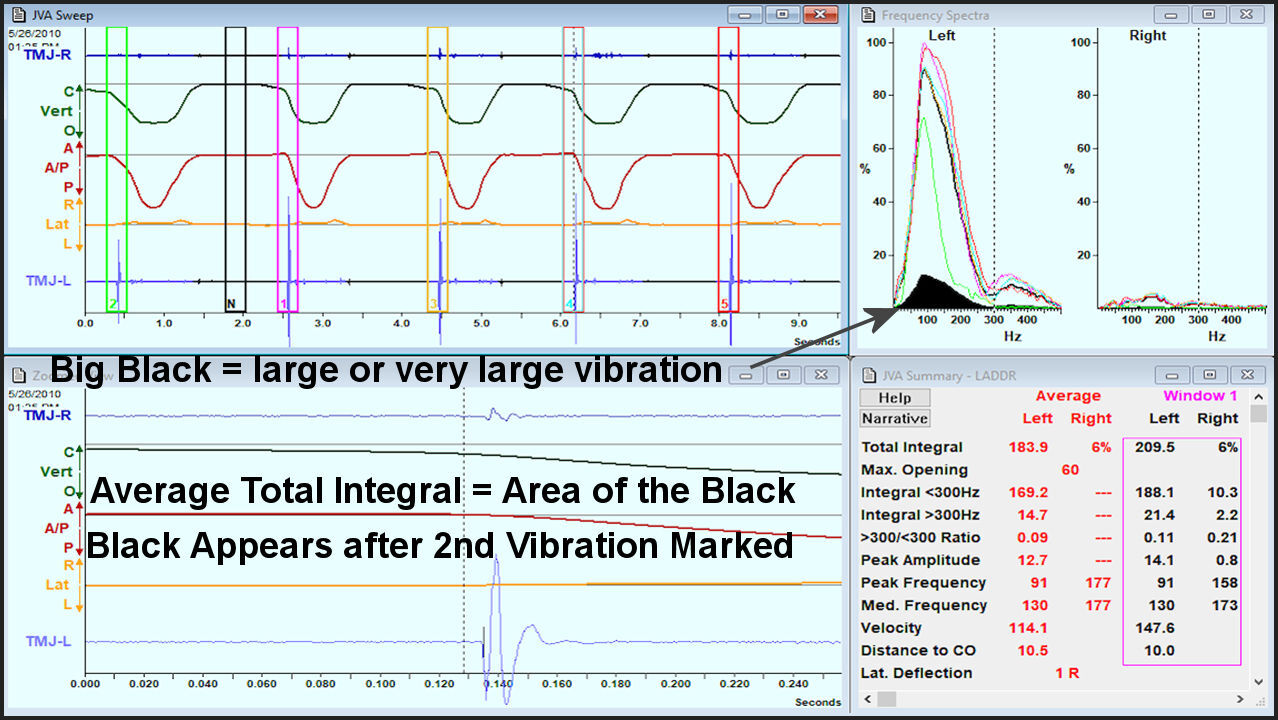
Only about 1 in 4 TMJs can be accurately diagnosed as a specific internal derangement just from a clinical examination.60 This unacceptable level of accuracy can be improved at least threefold by recording TMJ vibrations with BioJVA (Bioresearch Associates, Inc. Milwaukee, WI USA) with its artificial intelligence developed computerized analysis.61 See Figure 3. In the remaining cases TMJ imaging with CBCT or MRI is needed to fully describe a patient’s joint condition precisely.
_of_a_classic_reduction_vibration_of_an_anterior_disc_displa.jpg)
The most common non-surgical treatment of internal derangement historically has been the oral appliance (splint). Although not guaranteed, it has been found that an anterior repositing splint has a higher probability of successfully recapturing a reducing anteriorly displaced disc than a flat-plane appliance.62 The relatively high rate of successful symptom reduction attributed to splint treatments in patients without TMJ issues also supports an indictment of malocclusion for producing TMDs symptoms.
Although some studies have been unable to measure any spatial change within the TMJ provided by a splint, that is probably because any change is subtle.63 However, a splint provided for TMJ internal derangements that has a positive effect on the whole masticatory system (e.g., TMJs, masseters, anterior temporalis, etc.) implies that some spatial change has very likely occurred within the TMJs.64
Body posture has been measured as changed with some internal derangement patients.65–67 However, in one study the body postures of subjects with well-adapted internal derangements (asymptomatic subjects) were compared to the body postures of normal TMJ subjects, and no difference was found.68 No explanation was given by the authors for why only subjects with well adapted and asymptomatic internal derangements were compared to normal subjects instead of selecting any symptomatic TMDs subjects, but their results do support Kurita et al’s conclusion that successful adaptation of permanent disc displacements can occur in some cases.59
Symptomatic Maxillo-mandibular Mal-relationships
The relationship of the mandible to the maxilla develops during growth either normally or abnormally depending on the patient’s genetics and multiple environmental factors.69,70 Successful adaptation may be achieved when a process proceeds gradually, but for sudden changes (loss of teeth, trauma, etc.) poor adaptation is a more likely outcome. Developmental changes can occur gradually, such that if a patient with an abnormal maxillo-mandibular relationship (E.g., bilateral posterior crossbite) has never developed any symptoms, it is an indication that successful adaptation has occurred. Good adaptation presents with minimal muscle discomfort with the current maxillo-mandibular relationship, and the patient can function well despite any apparent structural abnormality.
Poor adaptation to a developmental or traumatic alteration of the relationship of the mandible to the maxilla can be the source of TMDs symptoms. Developmental abnormal relationships can best be corrected early with interceptive orthodontics71,72 or later with orthognathic surgery.73 For symptomatic adults, correction can easily be tested with a neuromuscular concept oral appliance to determine what extent of correction is possible. A permanent correction, aside from a permanent removeable appliance, can be far more complex involving prosthodontics, orthodontics, or surgical procedures.
The steps required to fabricate an appliance that is compatible with the musculature are quite simple. The first step requires the relaxation of the entire musculature (e.g., ULF-TENS, LLL, etc.).74–76 The second step includes the registration of a maxillo-mandibular bite that is determined by the patient’s own musculature without any hands-on manipulation involved.77–79 The preferably lower appliance needs a maximum intercuspal equivalent occlusion to establish a “home plate,” which is required for good proprioceptive function. A flat-plane appliance leaves the patient wondering where to close. An ideal lower appliance even allows the patient to masticate with the appliance in place. In extremely dysfunctional cases the ideal position may have to be gradually attained over a period of up to several months.
Historically missing molars and premolars were a common reason for developing a maxillo-mandibular mal-relationship in adulthood. Already by 1936, Dr. James B. Costen, an ear, nose and throat physician, had evaluated 125 fully edentulous patients with ear and head TMD-like symptoms, but without any detectable ear pathology.80 He referred these symptomatic patients to a local dentist who provided them with removable complete dentures and in doing so, reduced or eliminated their ear and head painful symptoms. Costen theorized that overclosure due edentulousness was the primary cause of their ear and head symptoms. Using early X-ray technology in 1938 he found various forms of TMJ damage in edentulous patients, which he correctly labeled “Mandibular Joint Syndrome.”81 Later it was renamed by dentistry, not by Dr. Costen, as “Costen’s Syndrome,” which evolved into TMJ Syndrome. Since the addition of fluoride into water systems and toothpaste formulas, and substantial improvements in oral healthcare, the percentage of fully edentulous adults, especially those without dentures, in this country has been substantially reduced.82 Thus the current TMDs population in the USA is not so highly edentulous. In countries with less developed economies edentulousness is often associated with TMDs.
How etiology can be determined
When a selected group of TMDs patients with a common etiology is treated successfully while comparable untreated cases do not improve, it supports the efficacy of the treatment. That is the maximum support that science can provide, because the scientific method can only disprove a theory it cannot prove one. Therefore, the only possible support for the theory that TMDs really are SSDs is to successfully treat TMDs patients using psychology/psychiatry. Psychological treatment must be able to demonstrate the alleviation of true Somatic Symptoms mirroring the way aspirin alleviates headache. However, to date no successful psychological treatments of TMDs have been demonstrated.83,84 Thus, very few TMDs can ever be labeled as SSDs (< 1 %)4 because 99 + % are driven by many real physical etiologies. See Figure 1. The sum of the available evidence supports somatic symptoms as being secondary to the physical etiologies of TMDs.31,32
Are obstructive sleep apnea, bruxism and airway constraints contributing factors to TMDs?
Breathing constraints such as obstructive sleep apnea have been linked to TMDs and bruxism has also been implicated in contributing to some TMDs.85–88 These conditions also support the concept that TMDs are Musculo-skeletal dysfunctions rather than somatic symptom disorders. These dysfunctions may or may not be etiologic in specific cases. However, they may be symptoms, like apparent SSDs, rather than causes of some TMDs.
DISCUSSION
There are limitations to the pain management approach to treating TMDs. Consequently, any even modest reduction in pain complaint is considered a successful treatment. While it is popular to claim that TMDs are Somatic Symptom Disorders (SSDs), (the current psychiatric term for somatization or psychosomatic illness), that claim is lacking in scientific support. Although it has been well documented that TMDs patients commonly appear to have emotional states comparable to SSDs, 99 % of TMDs cases the apparent SSD is not etiologic, but rather secondary to chronic pain, especially when the chronic pain is intractable.4,27,31,32 If TMDs were routinely SSDs, there should be many studies demonstrating successful psychological treatments of TMDs, but the few attempts at psychological counseling have produced very meager results. Meanwhile, there are scientific studies that demonstrate the efficacy of physical TMDs treatments and some even demonstrating the psychological benefits of successful physical treatments.27,31,32
A simple question must be answered for each TMDs case: Does the TMDs patient’s chronic pain cause the apparent somatic symptoms or are the somatic symptoms causing the TMDs? If somatic symptoms are causing TMDs, then a CBT approach should be rational, but if chronic pain from a Musculo-skeletal Dysfunction is causing the somatic symptoms, the MSD approach is the more rational choice.
“The new Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, somatic symptom disorder over-psychologizes people with chronic pain; it has low sensitivity and specificity, and it contributes to misdiagnosis, as well as unnecessary stigma. Adjustment disorder remains the most appropriate, accurate, and acceptable diagnosis for people who are overly concerned about their pain.”89 Patients unable to adapt successfully to their physical dysfunctions routinely exhibit somatic symptoms.
CONCLUSIONS
The pain management of TMDs does not require effort by the practitioner to understand the underlying physical etiology of a given case. When the practitioner erroneously concludes that a TMDs patient suffers from a somatic symptom disorder (SSD), any focus on physical treatment is lost. When the reduction of orofacial pain is the only focus of treatment, limiting care to palliative treatments can be rationalized, especially when the Neuromatrix Model of Pain has been embraced.28 Designating TMDs as somatic symptom disorders leads to a one-size-fits-all approach to TMDs limited to palliative, non-invasive, reversible methods and cognitive behavioral counseling. However, the dearth of evidence for successful pain management treatment of TMDs leaves that option without enough scientific support.
In stark contrast, the MSD approach to TMDs focuses on detecting the etiology of the disorder. This approach requires obtaining an accurate diagnosis so the focus of treatment can be upon eradicating the cause(s), whether multi or unifactorial. The MSD approach to solving TMDs benefits from modern computerized measurement technologies and treatments. Technologies such as ULF-TENS and EMG,90–92 JVA, Jaw Tracking, CBCT and MR imaging can identify the underlying etiologies involved in a specific case that are not revealed from the patient’s medical history or the clinical examination alone. Several oral appliances, T-Scan computer occlusal correction, and multiple lasers can provide corrective and healing capabilities that are well documented within the dental research literature. Thus, it is often possible to achieve the complete resolution of TMDs conditions, which is a comparatively rare accomplishment using a pain management approach.
Funding Statement
No funding of any kind was received to support this project.