INTRODUCTION
Much has been published on Menière’s Disease (MD), which was first identified and characterized by Prosper Menière over 150 years ago.1 Today diagnosing and treating MD among clinicians remains challenging2–7 and as a result MD continues to be a catchall for vertigo of unknown origin. Endolymph Hydrops (EH) remains a histologic finding in most but not all MD cases, while the MD diagnosis remains purely a clinical diagnosis. There is no agreement on the etiology of MD as it relates to Endolymphatic Hydrops.6,8–12 Current considerations is that EH is a histological sign of the disease rather than a causative etiology.6,9–16 Some research has attempted to induce MD by increasing the endolymph production or limiting its reabsorption through medications. Those models did produce EH but did not produce MD symptoms.17–19 Even if EH does have some influence over vertigo, it does not adequately explain the persistence of tinnitus, ear fullness, or hearing loss progression.
In an attempt to bring clarity to the ENT community a few consensus statements and reviews have been published.6–12 The American Academy of Otolaryngology – Head and Neck Surgery published a clinical practice guideline on MD6 with the stated purpose: “To maximize treatment, it is important to clinically distinguish MD from other independent causes of vertigo that may mimic MD and present with hearing loss, tinnitus and aural fullness.”6 Even though TMD has been known to present with this same presentation of symptoms,20–31 the AAO-HNS fails to make any mention of the similarities in inner ear symptom presentation between TMD and MD anywhere in its 55-page guideline. This is counter intuitive if the aim of their guideline is to distinguish MD from other causes that could mimic MD symptomology. See Appendix summary for TMD vs MD Symptomology Comparison.
It is well known that James Costen, an otolaryngologist, read his initial findings of inner ear and sinus symptoms related to disturbed function of the TMJs in 1934 before the Texas Ophthalmological and Otolaryngological Society and was later pubished.32 More recent authors have subsequently labeled his work Costen’s Syndrome, which eventually became known as TMJ Syndrome and currently is labelled as Temporomandibular Disorders (TMD) or Temporomandibular Joint Disorders (TMJD).
From the 1990s into the 2000s research spearheaded by Bjorne et al began establishing a link between TMD and MD.22,33–35 Treating TMD patients that were also diagnosed with MD resulted in complete resolution of the MD (and TMD) symptoms or decreased to a level they no longer were life altering for the patient. The symptom resolution was long term as indicated by 3-year and 6-year follow up studies.33,34 Treatments rendered were occlusal adjustments, TMD splint therapy, cervical spine therapy and physical therapy.22,31–35 It is impossible to know if one therapy is responsible for the therapeutic outcome or if it was a result of a synergistic effect of all of the therapies being used in conjunction with each other.
A couple of case studies have shown occlusal adjustments to be highly effective in the treatment of patients that have a diagnosis of Meniere’s Disease.36,37 The present study only used bite revision therapy via DTR in an attempt to bring symptom relief in a cohort of 86 subjects with a diagnosis of MD. DTR has previously demonstrated effective and long-term symptom resolution in patients diagnosed with TMD and Orofacial pain.38–47
OBJECTIVES
The objectives of this cohort study were: 1) to perform DTR Therapy on patients with an otolaryngologist’s diagnosis of MD who presented with long Disclusion Times and/or a bite force imbalance, including high excursive muscle activity levels, all of which could promote MD symptomology and 2) to reveal any significant changes in masticatory function as indicated by EMG and EGN data. The Null hypothesis: DTR does not affect MD symptomology.
METHODS
Eighty-six patients previously diagnosed with Meniere’s Disease (MD) by otolaryngologists were evaluated in two different dental practices that offered specialized Disclusion Time Reduction (DTR) services for patients with temporomandibular disorders (TMD). All patients had prior magnetic resonance imaging (MRI), which ruled out auditory neuromas. All 86 patients had received various unsuccessful treatments from dietary restrictions such as avoidance of salt and caffeine to inner ear gentamycin and stem cell injections. None of these treatment options had brought about relief for an extended length of time. While patients were not selected at random, they were consecutive patients referred to each of the two dental offices. In one general dentistry office located in Eugene, Oregon, 32 consecutive patients diagnosed with MD were treated successively. All who walked in and met the inclusion criteria were evaluated and treated. The second dental office was located within the RajaRajeshwari Dental College, Dept of Orofacial Pain under Rajiv Gandhi University of Health Sciences in Bengaluru India. The Dept of Ear Nose and Throat at RajaRajeshwari Medical College was contacted to refer patients (52) that met the inclusion criteria to the second dental office to be evaluated and treated with DTR. An IRB approval was requested and obtained for a retrospective cohort study #BIRB/99Z/2022.
The Inclusion criteria were:
-
A MD diagnosis from an otolaryngologist with MRI that definitively ruled out an auditory neuroma.
-
The existence of ongoing MD symptomatic episodes
-
28 teeth with symmetrically missing teeth (if one molar was missing on the left side, then one had to be missing on the right side)
-
Near normal occlusal relations with molars and premolars in contact during the right and left excursions
-
Angles Class I and Class III occlusal relations, with guiding anterior teeth that were either in contact, or near to contact.
-
Patients that had been previously treated for MD but had not received symptom resolution.
-
Patients 18 years of age or older
The Exclusion criteria were:
-
Severe Class II malocclusions
-
Anterior open bite where anterior guidance contact could not be achieved.
-
A previous history of TMJ trauma
-
The presence of unstable Temporomandibular Joint internal derangements verified by CBCT and/or Joint Vibration Analysis (JVA).
-
Patients that had been previously treated with MD therapy and received symptom resolution.
-
Patients who had undergone prior TMD therapy, including prior occlusal adjustment treatment.
Informed consent was obtained from each patient for undergoing the DTR coronoplasty, and for collecting MD symptom severity, frequency and duration data from questionnaires as well as masticatory evaluation. Oral health histories were also obtained where the whole participant group reported experiencing MD symptoms. All the group reported fullness in the ear, tinnitus, vertigo (including drop attacks) and hearing loss in at least one ear. The group also reported many TMD symptoms with moderate to severe frequencies and intensities. The TMD symptoms seemed to be randomly distributed and no correlation could be made with any one symptom to the MD symptoms. DTR therapy is discussed and reviewed in Part 1 of this series and will not be repeated here.
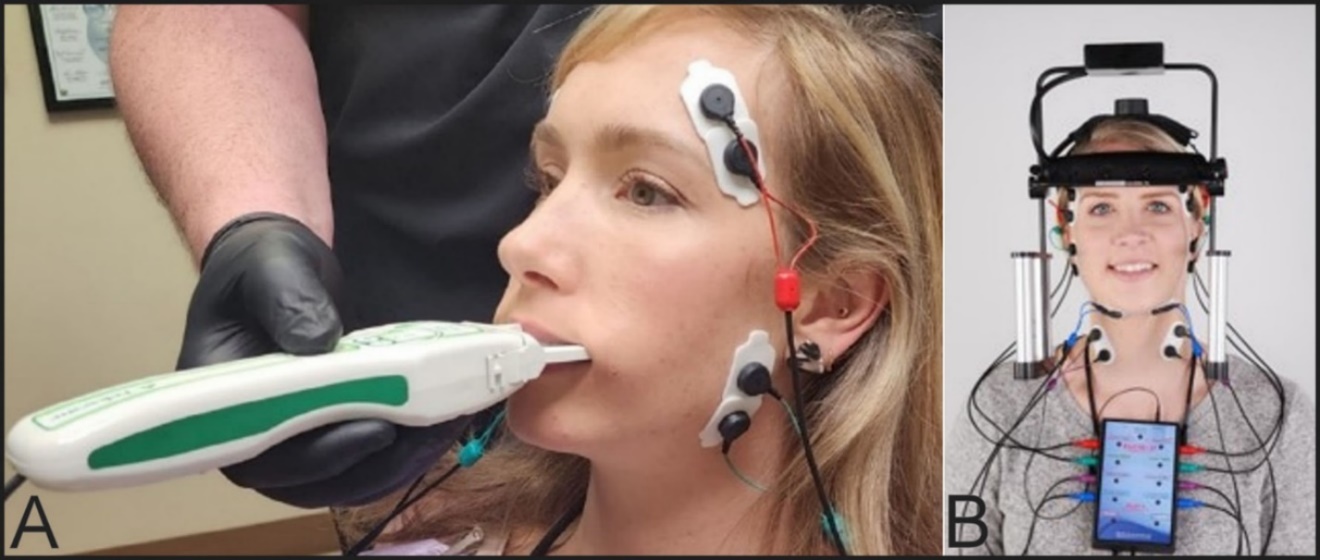
Every participant underwent a pre-DTR right and left excursive Disclusion Time/muscle hyperactivity evaluation with the synchronized T-Scan 10/BioEMG III technologies (Tekscan Inc., S. Boston, MA USA; Bioresearch Assoc., Inc. Milwaukee, WI, USA). See Figure 1A. This allowed accurate EMG and disclusion times to be recorded prior to the therapy. All subjects, at the same appointments, had masticatory function assessed with combined electrognathology (EGN) (Bioresearch Assoc., Inc. Milwaukee, WI, USA) and electromyography (EMG) recordings of gum chewing.48–58 See Figure 1B. This was done to evaluate; 1) the function of the TMJ and 2) the quality of mastication of a soft bolus (gum) using BioPAK software (BioResearch Associates, Inc. Milwaukee, WI USA).59–61 The recordings were repeated at each initial appointment and mastication was evaluated at pre-treatment and 3 to 4 months follow-up appointments.62 The analysis of the masticatory function data is reported in this Part II.
_t-scan_10_digital_occlusal_analyzer_recording_bite_force_and_time_synchronized_with_bio.jpeg)
A total of 86 patients participated, 47 males and 39 females at a ratio of 1.2:1. The mean age was 50.8 (+/- 18.1) years with a range from 17 to 80 years and a median of 55. While the age distribution was not a normal one, it does represent a range of likely candidates. Patients were selected sequentially as they agreed to participate.
The Wilcoxon Signed Rank test was applied to the survey data of MD symptoms to detect significant improvements. Student’s paired t test was applied to the measured intra-patient EGN and EMG data, making each subject his or her own control. Consequently, no separate control group was enlisted because the purpose was simply to correlate the masticatory function data with the MD symptom levels.
RESULTS
The previous report (Part I) revealed that the presence of ear fullness, vertigo and tinnitus were significantly reduced up to 3 – 4 months after DTR treatments (p < 0.05). This report (Part II) is focused on significant improvements in masticatory movement and muscle function towards the expected norms for these parameters.
Where the timing of the chewing motion was significantly changed post-treatment after DTR, the changes were towards mean normal values. For left-sided gum-chewing the mean Opening Time and mean Cycle Time were significantly shortened (p < 0.05) with a trend towards a shorter Occlusal Time as well (p < 0.10). For right-sided gum-chewing the mean Opening Time, mean Closing Time and Mean Cycle Time were significantly shortened (p < 0.05), while the Occlusal Time was significantly lengthened (p < 0.05). The pre-treatment cycle times were long, but the post treatment mean cycle times were within the expected normal range of 0.50 to 0.8 seconds. See Table 1.
The means of the left and right gum-chewing vertical Turning Points (TP) increased significantly towards the mean normal value (16 mm) after DTR treatment (p < 0.05). The mean of the left gum-chewing antero-posterior Turning Point increased significantly (p < 0.05), but the increase in the right-sided gum-chewing antero-posterior Turning Point did not reach significance (p > 0.05). For left-sided gum-chewing the mean lateral Turning Point significantly decreased (p < 0.05), but the right-sided gum chewing lateral Turning Point only trended toward a significant change (p < 0.10). See Table 2.
The mean Terminal Chewing Position (TCP) is the distance between the arches at the point of maximum bolus crush. The amount of crush is dependent on the nature of the bolus. Gum usually crushes to a very thin bolus. Although the bolus was crushed more in all three dimensions during left gum-chewing, only the left chewing Lateral TCP change was significant (p < 0.05) post-treatment with DTR. See Table 3.
Maximum lateral width trended towards an increase for left-sided gum-chewing (p < 0.10) but decreased significantly for right-sided gum-chewing (p < 0.05). For Left-sided gum-chewing both the opening and the closing velocities increased significantly (p < 0.05). For right-sided gum-chewing the opening velocity increased significantly (p < 0.05) while the closing velocity only showed a trend towards increasing (p < 0.10). See Table 4.
Frontal opening angles did not change significantly for either left or right gum-chewing. However, frontal closing angles were reduced significantly to smaller angles for both left and right gum-chewing (p < 0.05). Jerkiness during opening was reduced significantly for both left and right gum-chewing (p < 0.05). Jerkiness was significantly reduced during closing for right gum-chewing (p < 0.05), but not for left gum-chewing. See Table 5.
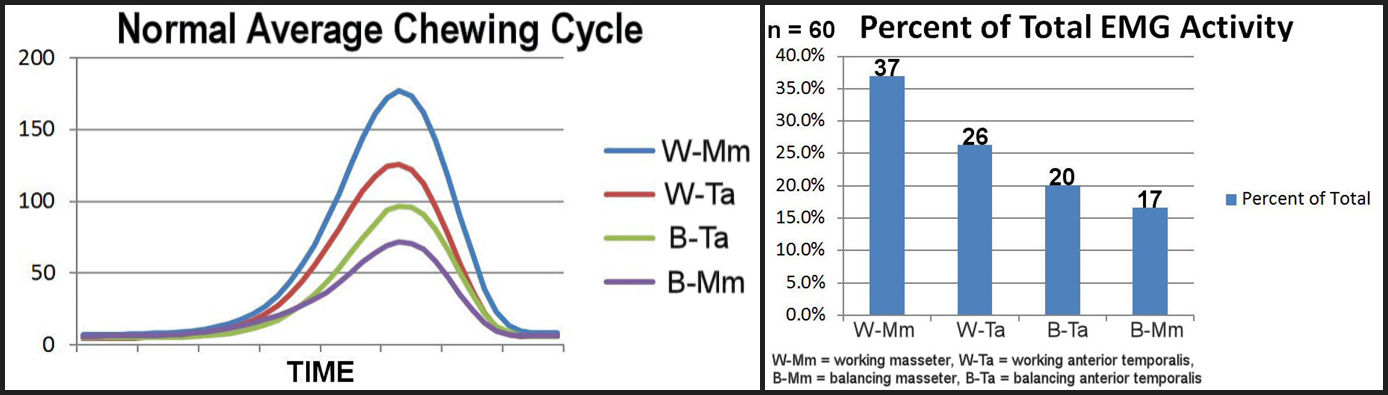
The overall effort of chewing is indicated by the mean levels of EMG activity in the 4 superficial elevator muscles measured from each given subject. All four muscles significantly reduced their activity after DTR treatment, both for left-sided gum-chewing and for right-sided gum-chewing (p < 0.05). See Table 6.
The coefficient of variation (the standard deviation divided by the mean) is an indication of the relative variability. Among this group of subjects, significant reductions were seen in the right-sided gum-chewing relative variability after their DTR treatments (p < 0.05). For the left-sided gum-chewing only the non-working temporalis varied significantly less (p < 0.05), although a trend was present in the reductions in the CV for non-working masseter and working temporalis muscles activities (p < 0.10). See Table 7.
The Peak Amplitude in microvolts is the highest level of contraction during the chewing cycle. Three of eight mean values revealed significant reductions in peak amplitude (p < 0.050, three reductions showed trends towards significant reductions (p < 0.10) and two showed non-significant reductions. See Table 8.
The significant decreases in mean cycle times were repeated for all four muscles in both left and right gum-chewing with shortened mean times from the onset of opening to the peak amplitude of each muscle’s contraction (p < 0.05). See Table 9.
Significantly shorter times from peak EMG amplitude to the end of closure (onset of occlusion time) was recorded in all four muscles during right-sided gum-chewing (p < 0.05). However, only the working temporalis’ reduction in time achieved significance during left-sided gum-chewing (p < 0.05). See Table 10.
DISCUSSION
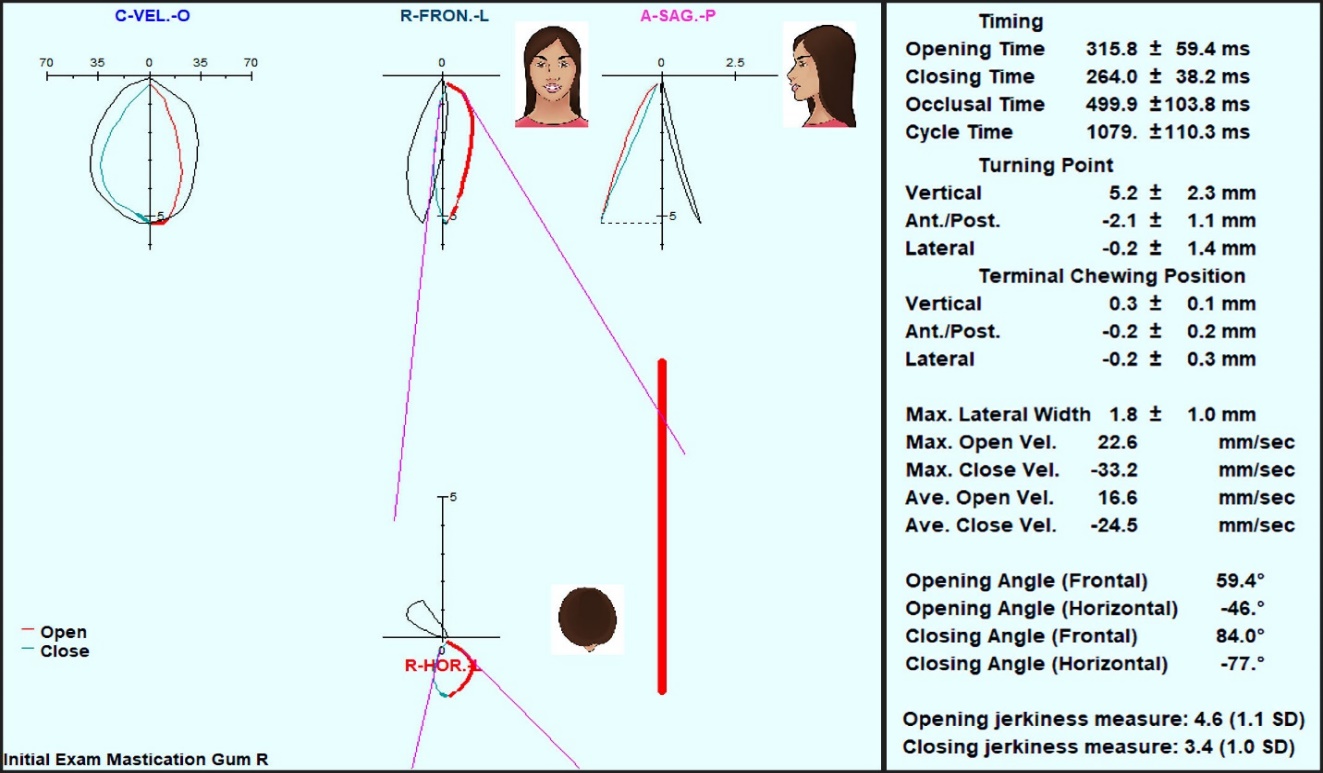
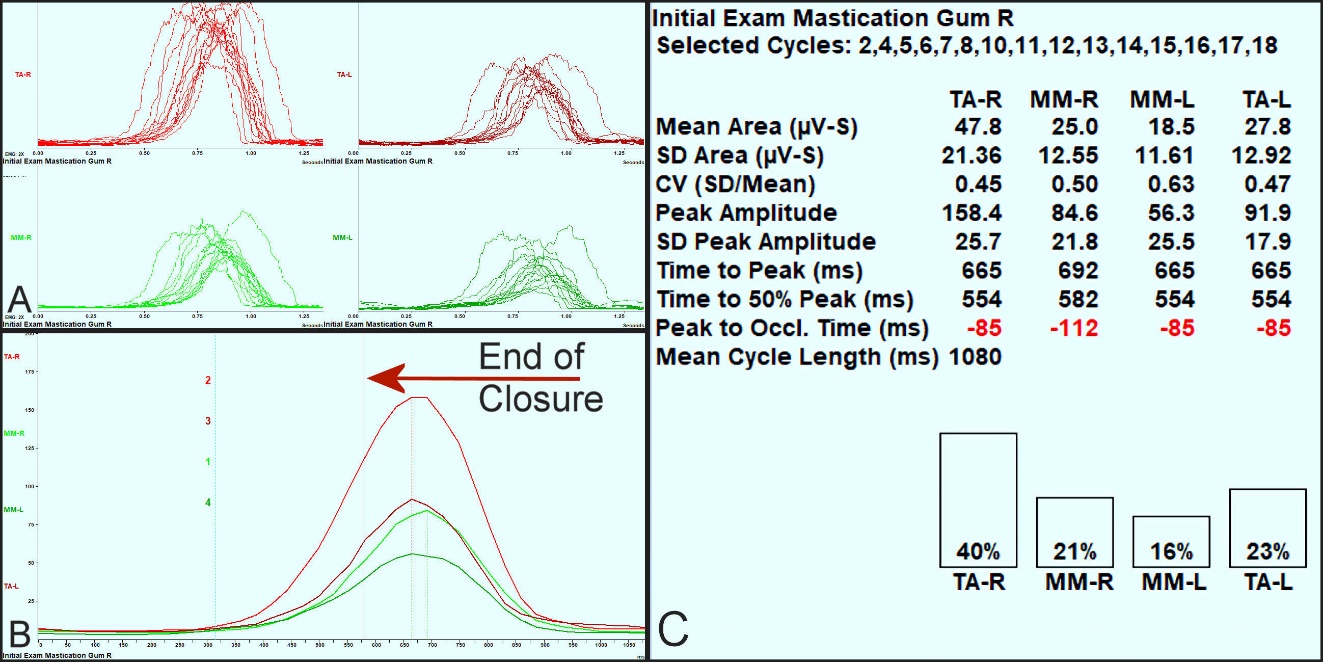
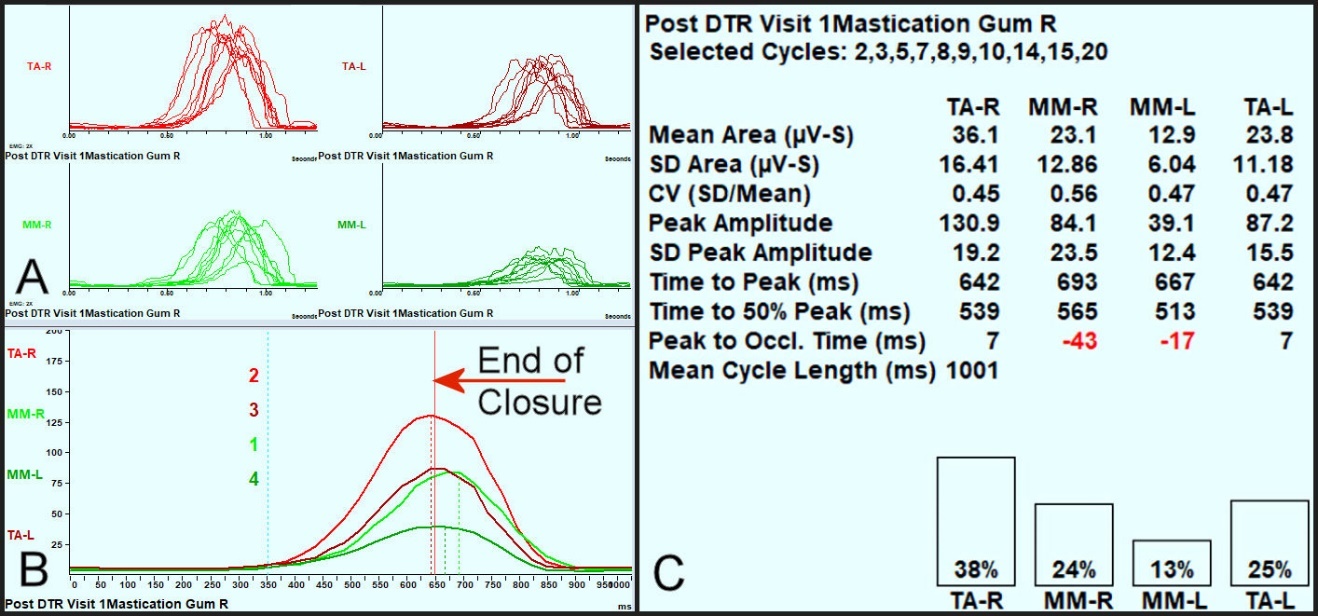
The results of this study corroborate the prior case report’s that observed MD symptom reductions following a measured occlusal adjustment therapy (DTR).36,37 EGN (jaw motion) and EMG (temporalis and masseter muscles) were recorded bilaterally and simultaneously and analyzed together. Figure 2. Shows an example of the pre-treatment Average Chewing Pattern (ACP) along with the timings, Turning Point, Terminal Chewing Position, velocities, angles and Jerkiness. The ACP was very small, slow and highly variable, all indications of masticatory dysfunction. In Figure 3 the right and left temporalis muscle bursts (in red) and R and L masseter muscle bursts (in green) during gum chewing pretreatment. The right temporalis was providing a disproportionate amount of effort compared to a normal muscle balance. Notice there was a delay in all the peaks of muscle contraction (red numbers) until after the end of closure. This indicates hesitancy, in retrospect, most likely due to muscles that were firing carefully to avoid occlusal interferences.
_pre-treatment_with_numerical_values._ve.jpeg)
_the_same_patient_s_highly_variable_firing_pattern_of_elevator_muscles_cycle_to_cycle_sh.jpeg)
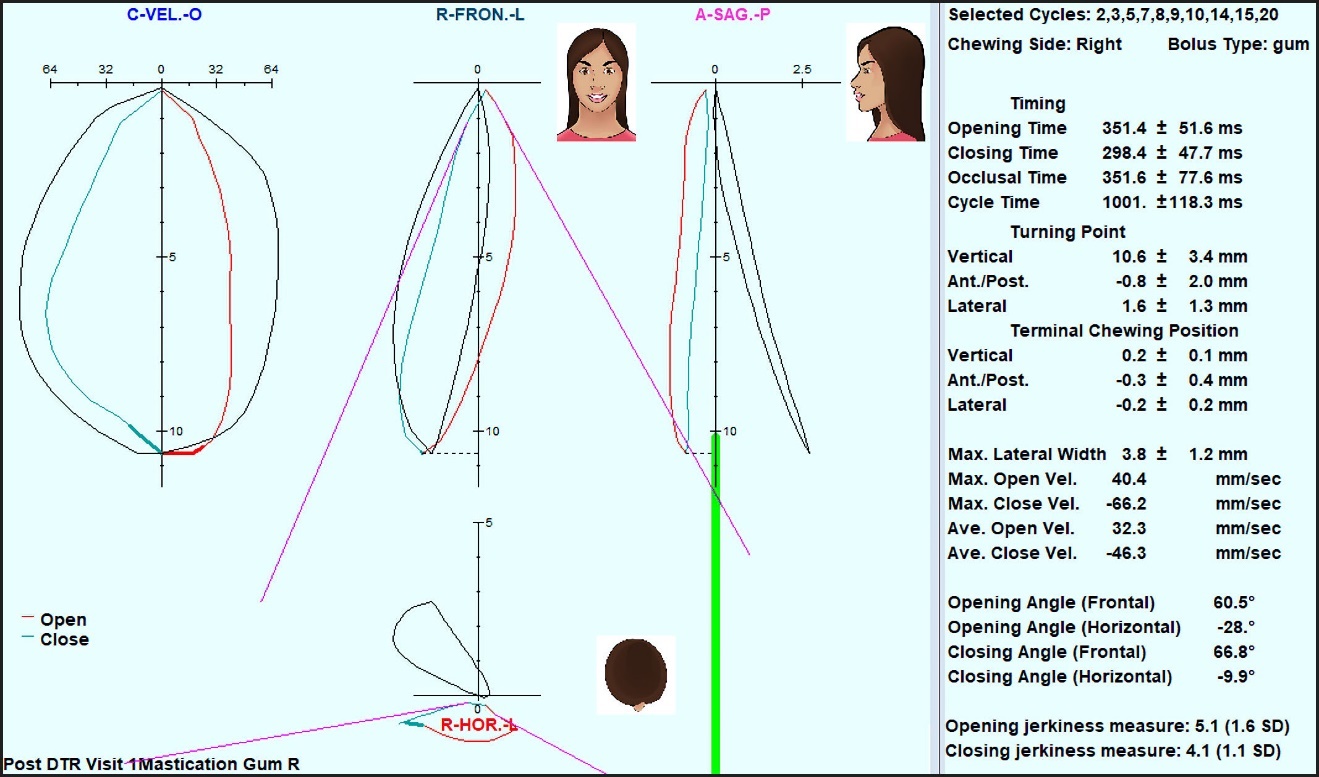
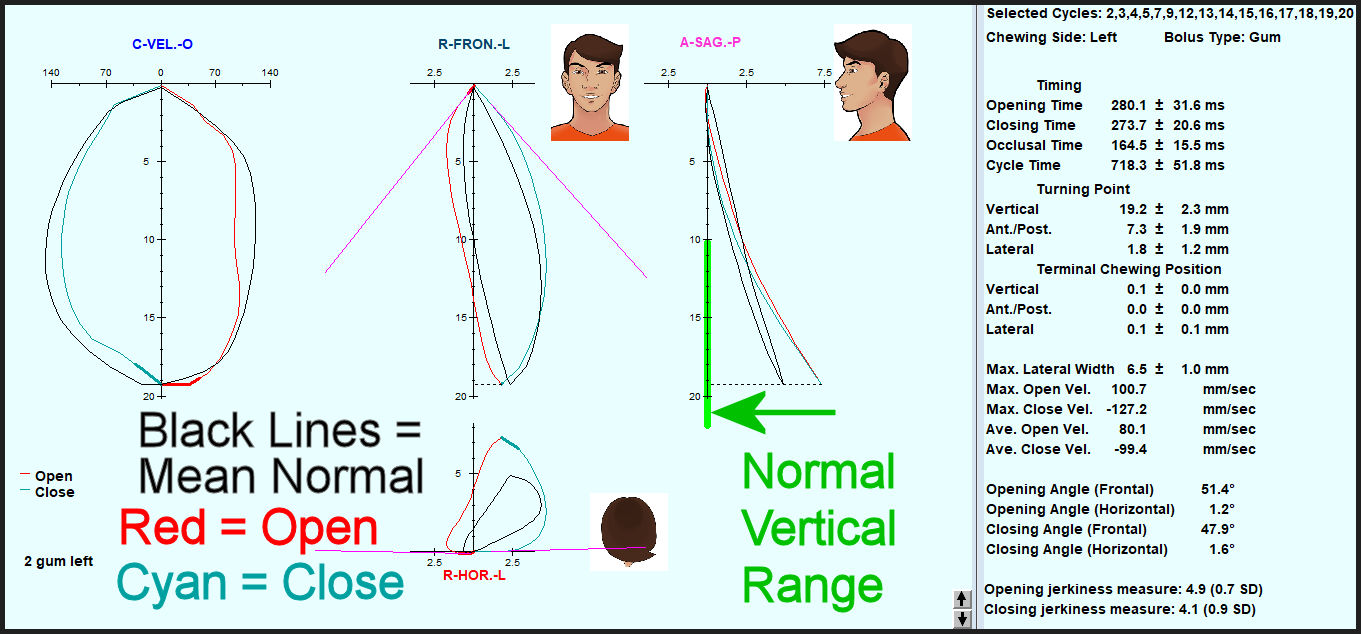
In Figure 4 the size of the ACP was increased dramatically (see Turning Point) and the velocities were increased towards normal values. The other numerical values were only changed slightly. In Figure 5, the same ACC data immediately following DTR therapy, the balance between the muscles was improved and only the masseter muscles peaked slightly delayed after the end of closure (red numbers in Figure 4). Synergy of muscle contraction was improved, and the ACC curve composite appears closer to a “normal” non-MD sufferer’s muscle pattern.

_immediately_following_dtr_therapy_the_standard_deviation_of_each_muscle_s_activity_was_.jpeg)
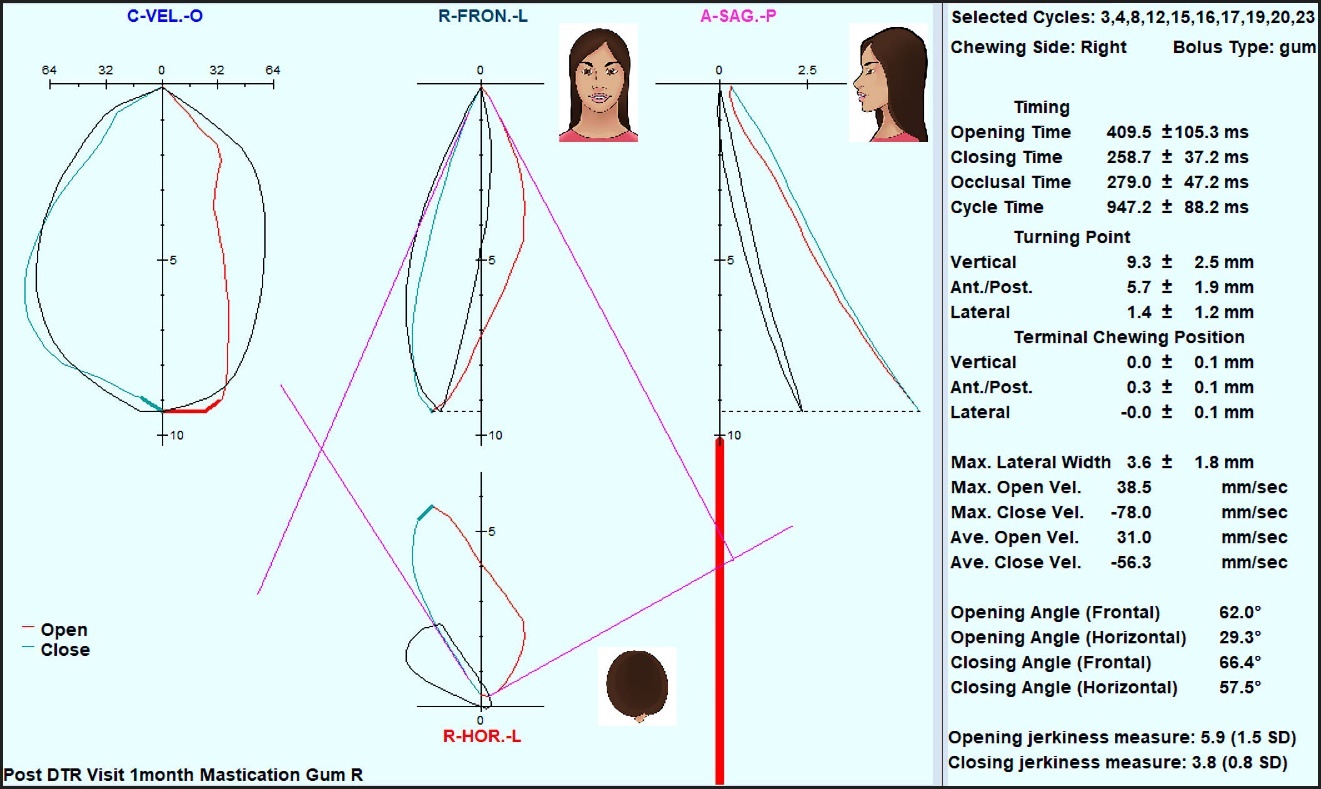
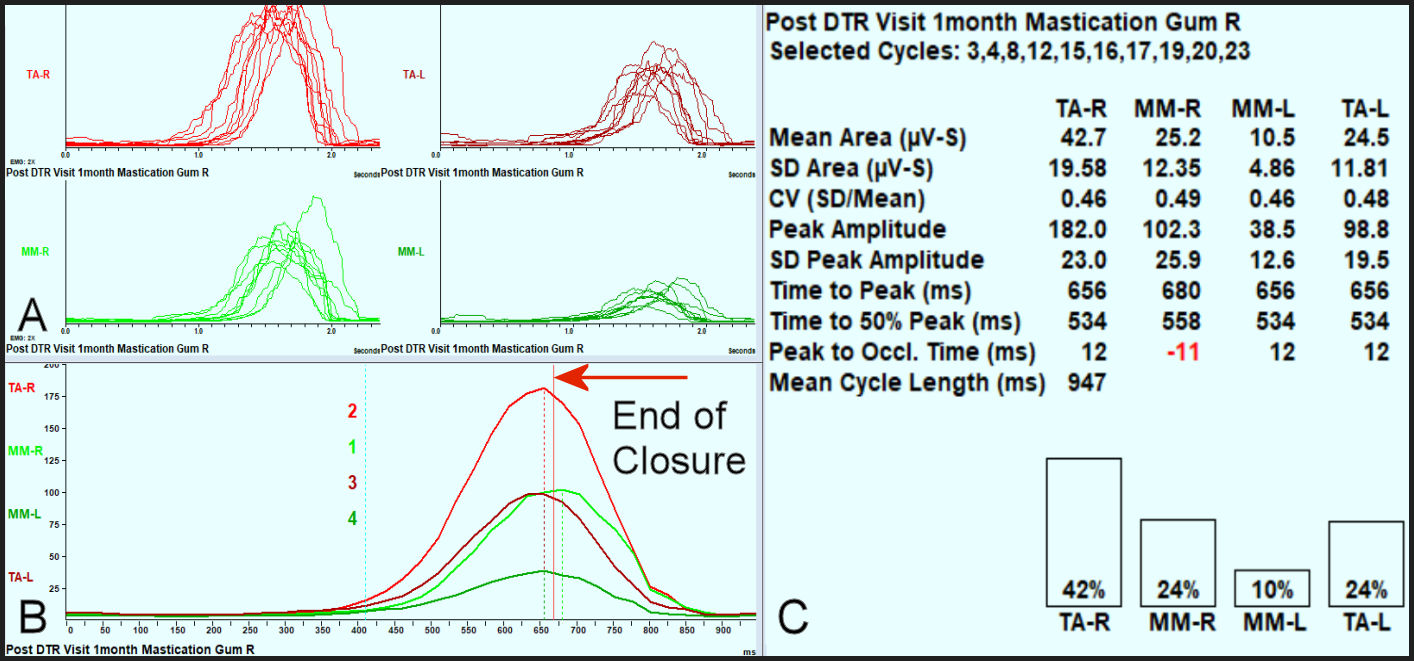
In Figure 6, one month post DTR, the closing time, occlusal time and cycle time were reduced and most importantly, the ACP shapes (red and cyan) were matching the mean normal shapes (black) very closely. Note: The overall shapes of the APCs are more indicative of normality than any single parameter. There was some opening interruption in the velocity, probably a left TMJ issue, which retained a retarded opening time and contributed to a longer than ideal cycle time. Figure 7 reveals the same ACC values one month post treatment. Only the right (working) masseter peak was still delayed to slightly after the end of closure (by 11 milliseconds) and the other three muscles peaked together prior to the end of closure. The amount of effort of the non-working masseter, an adaptation factor, and its variability were both reduced.

_four_months_post_therapy_the_variability_was_more_consistent_between_muscles__b)_workin.jpg)
Movements
Opening time delays are often caused by TMJ internal derangements, less often by occlusal interferences. Closing delays are more likely due to hesitancy, avoidance of occlusal interferences and uncertainty with respect to the Intercuspal position. For the left-sided gum-chewing (Table 1) the only timing factor of the group that did not show any reduction was the mean closing time. However, the pre-treatment mean closing time already fell within normal limits.53–55,59 The pre-treatment mean Opening Time was greater than the mean normal value but was reduced to within normal limits after treatment. For right-sided gum-chewing all 4 timing parameters were reduced by treatment to values within normal limits.53–55,59 Dysfunction slows down masticatory function such that any improvement in function shortens the timings.
The Turning Point (TP) is the point at the furthest opening where the transition occurs from opening to closing. The mean normal for vertical dimension is 16 mm with a range of 10 to 22 mm. The mean Vertical and Antero-posterior Turning Points increased significantly towards the mean normal value for left-sided gum-chewing, but the increase in the A/P Turning Point for right-sided gum-chewing did not achieve significance.53–55,59 The left gum-chewing lateral turning point showed a trend towards an increase (p < 0.10), while the right gum-chewing lateral turning point was already close to the mean normal value (2.3 mm) prior to treatment and changed little post-treatment. See Table 2.
The Terminal Chewing Position (TCP) indicates the extent of the bolus crush with smaller numbers indicating a more crushed bolus. Although the left-sided Terminal Chewing Position decreased in all three dimensions, only the lateral dimension decreased significantly. No significant changes were found in any dimension of the Terminal Chewing Position for right-sided gum-chewing. Since gum is a very soft bolus easily crushed, this result was not surprising and it means that as a group, most of these subjects were muscularly accommodating to their existing malocclusions. See Table 3.
The Maximum Lateral Width is the extreme lateral dimension of the frontal chewing pattern. While there was a significant decrease during right-sided gum chewing and a trend towards an increase in left-sided gum-chewing, all four mean values were found to be within normal limits prior to and post treatment.53–55,59 See Table 4. Significant increases in Maximum Opening Velocity were observed post-treatment in both the left and right-sided gum-chewing. The left-sided gum-chewing closing velocity increased significantly, while the right-sided gum-chewing only exhibited a trend towards a significant increase (p < 0.10). The mean normal values for opening (> 100 mm/second) and closing (> 120 mm/second) were nearly all achieved by this group post treatment.
The frontal opening angles did not change significantly for left-sided or right-sided gum chewing because both sides were within normal limits prior to treatment. Significant decreases towards more normal values (less restrictive) for frontal closing angles were found for both left-sided and right-sided gum-chewing. While opening jerkiness decreased significantly for both sides of gum-chewing, the closing jerkiness only decreased significantly for right-sided gum chewing because the left-sided gum-chewing was already within normal limits prior to treatment (3.2). Patients with un-adapted dysfunction tend to close carefully, which often reduces their closing jerkiness to within normal limits. See Table 5.
Muscle Function
The overall effort of chewing was significantly reduced for all four muscles after treatment (Bilateral masseter and anterior temporalis). When the need for accommodation to structural issues like malocclusion and/or temporomandibular joint dysfunction is reduced, the muscular effort required to chew is lessened. A simple change like removing pre-mature occlusal contacts, as done in this study, can significantly reduce extra muscular effort, especially from the non-working side muscles. See Table 6.
The coefficient of variation (CV) is a relative indicator of variability (the standard deviation divided by the mean). Although variability is expected with good masticatory function, excess variability occurs when dysfunction is present. For right-sided gum-chewing the variability was reduced significantly after treatment for all four muscles. For left-sided gum-chewing the variability decreased but significantly only for the non-working temporalis. The non-working masseter and the working temporalis exhibited a trend towards reduced variability (p < 0.10), but not the working masseter. See Table 7.
The Peak Amplitude represents the highest effort exhibited by the muscle. As the term suggests, it is a momentary level of highest intensity contraction within each cycle. In all muscles under both left and right-sided conditions there were reductions in all mean peak amplitudes. The changes were significant in 3 of the 4 muscles for left-sided gum-chewing, but not for right-sided gum-chewing. Only a trend towards a reduction occurred in both temporalis muscles (p < 0.10), but no significant change in the masseter peak contraction levels. See Table 8.
Table 9 concurs with Table 1 in that the significantly reduced cycle times post treatment also resulted in significantly reduced times from the onset of opening to the peak of the muscle activity for all 4 muscles and for both left-sided and right-sided gum-chewing.
The time from the peak of muscle activity to the onset of occlusion (end of closure) is normally a positive value meaning the peak occurs prior to the end of closure. Within this group of subjects, the mean values were positive both prior to and post treatment, but with significant reductions for right-sided gum-chewing (p < 0.05). For left-sided gum-chewing only the working temporalis timing was significantly reduced (p < 0.05). However, the variability was reduced for all muscles and for both chewing sides. See Table 10.
SUMMARY OF SIGNIFICANT FINDINGS
Improvements towards normality were seen in all 10 parameters used to evaluate the masticatory function of these Meniere’s Disease patients.
-
The mean chewing timings improved towards mean normal values after DTR.
-
The mean vertical turning point increased significantly towards the mean normal.
-
The left-sided gum-chewing mean lateral terminal chewing position (TCP) significantly reduced.
-
The mean opening and closing chewing velocities either increased significantly or showed a trend.
-
The mean frontal closing angles significantly decreased towards more normal (less restrictive) values.
-
The mean EMG chewing activity was significantly reduced for working and non-working muscles.
-
The mean variability in the EMG muscle contraction activity patterns decreased for all muscles.
-
The means of the peaks of EMG activity decreased for all muscles post treatment.
-
Mean time to peak muscle activity was reduced significantly for all muscles and conditions.
-
Time from peak muscle activity to the end of closure appeared to increase for all muscles.
These findings do correlate with MD symptoms improving as the mastication improves and support the findings of others investigating masticatory disfunction.63–69 We reject the null hypothesis.
LIMITATIONS
The ICAGD treatments via DTR therapy are standardized and have been successfully reported from different practitioners in previous studies.47,60–62,70–73 This study’s primary focus was treatment outcomes. No control subjects were utilized, but rather each subject served as their own control being compared to themselves pre vs post therapy. This was intentional in the study design because denying symptomatic subjects’ treatment or giving a placebo for several months carries ethical concerns and are difficult to maintain.
CONCLUSION
Eighty-six subjects with a confirmed diagnosis of Meniere’s Disease experienced reductions in frequency, duration and intensity of their MD symptoms following reductions in Disclusion Time and muscle activity via DTR through computer guided coronoplasty (Part 1). This study shows definitively that the pretreatment evaluation of masticatory function (through EGN and EMG) reveals dysfunction. The post therapy mastication data indicates more normalized function after therapy. Although occlusion has been overlooked in most of the medical and dental literature as a possible etiology of MD, the results of this study point to malocclusion, specifically bite force and bite timing, as the etiology for the symptoms in this group of subjects diagnosed with MD. These findings support occlusion as a major contributor to the function and disfunction of the masticatory system thus playing a significant role in symptomology. This includes symptoms such as hearing loss, vertigo, tinnitus and fullness of the ear, which in isolation from other symptoms suggests MD.
DECLARATION OF CONFLICTS STATEMENT
Drs. Ben Sutter, Prafulla Thumati, and Roshan Thumati claim no conflict of interest. John Radke is the Chairman of the Board of BioResearch Associates, Inc., the manufacturer of the BioEMG III and a distributor of the T-Scan. He receives no commission or other monetary incentive based upon sales of the T-Scan or the BioEMG III.
FUNDING STATEMENT
No funding from any source was provided to complete this study.
_of_chewing_motion_(black_lines)_with_a_control_.jpg)
_of_bilateral_masseter_and_anterior_temporalis_mus.jpg)