





INTRODUCTION
Rinchuse et al’s abstract, consisting of outdated biomechanically driven occlusal opinions, was compared to a scientific data-based rebuttal with comments below:
This commentary claims to critically examine the validity of the Canine Protected Occlusion (CPO) concept from both biological and evidence-based perspectives to question:
"Does the presence of CPO protect an individual from having Temporomandibular Disorders (TMD), periodontal disease, orthodontic tooth relapse, tooth wear and/or tooth fracture.1
Is this understanding based on function, physiology, esthetics, or evidence?1
Is the notion that CPO is the preferred functional occlusion scheme an outdated concept?"1
Rebuttal - The authors failed to “critically examine” the extensive Measured Digital Occlusion published science from the past 4 decades that definitively supports the biologic and evidence-based neuro-occlusal physiologic patient benefits of a Canine Protected Occlusal (CPO) design.
“An extensive review of the pertinent literature related to the topic of Canine Protected Occlusion (CPO) was conducted by the authors.”1
Rebuttal - Despite claiming that an “extensive literature search” was made, it was an “extensively biased search” to avoid all the biometric CPO, T-Scan/EMG, and Disclusion Time Reduction (DTR) literature beginning in 1989, that validated the therapeutic benefits of a Canine Protected Occlusion (CPO) when refined with Disclusion Time Reduction (DTR) computer-guided occlusal adjustments. This volume of non-included science strongly validates the occluso-neurophysiologic muscle lessening effect of a Canine Protected Occlusion.2–54
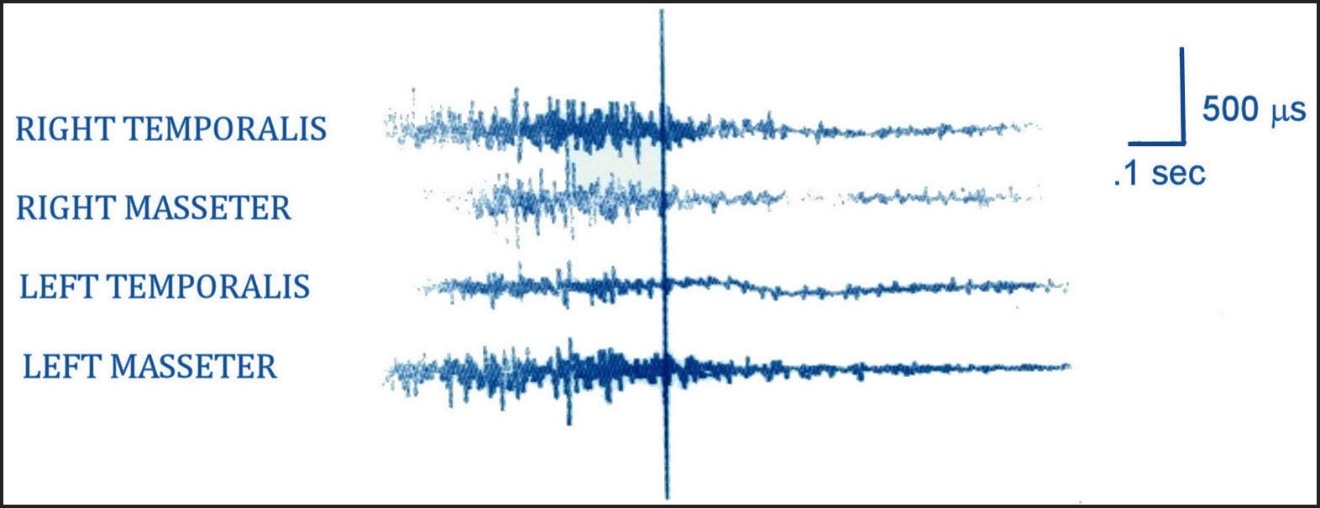
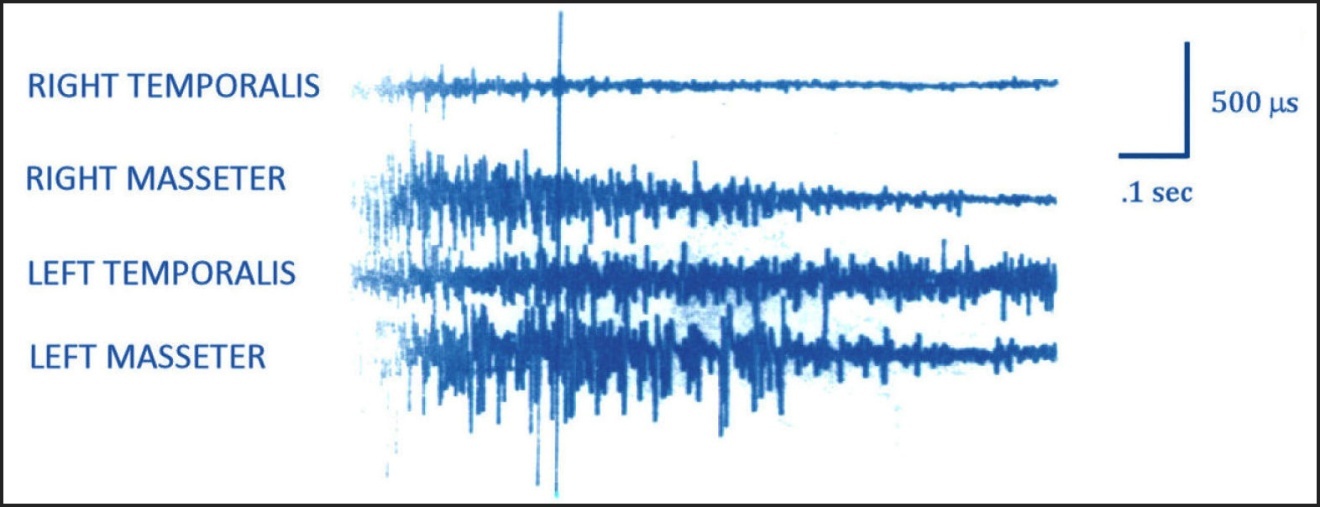
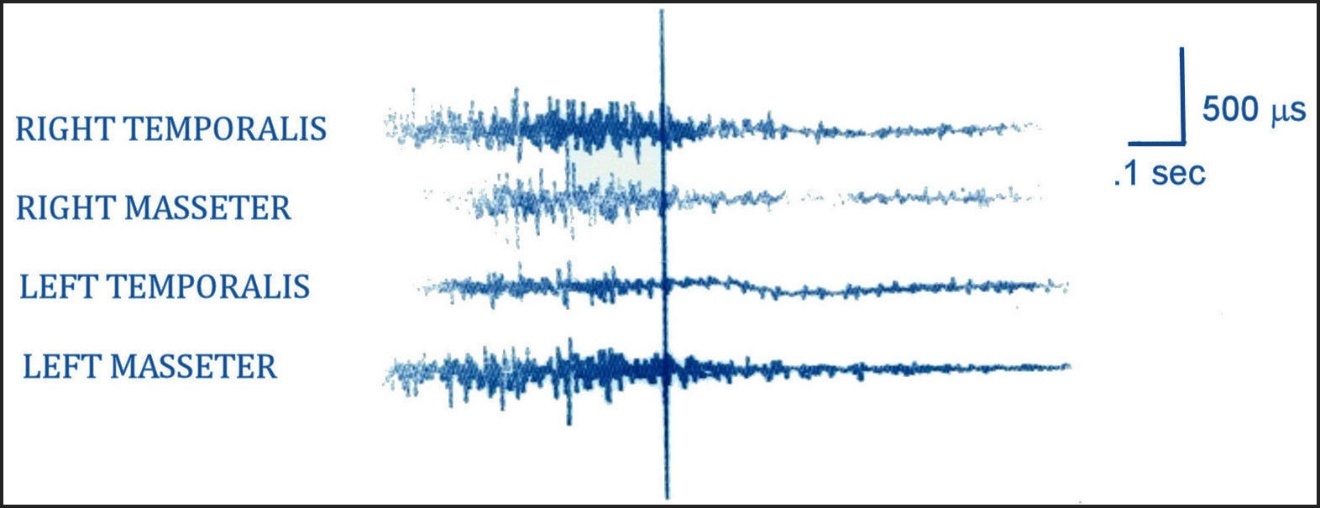
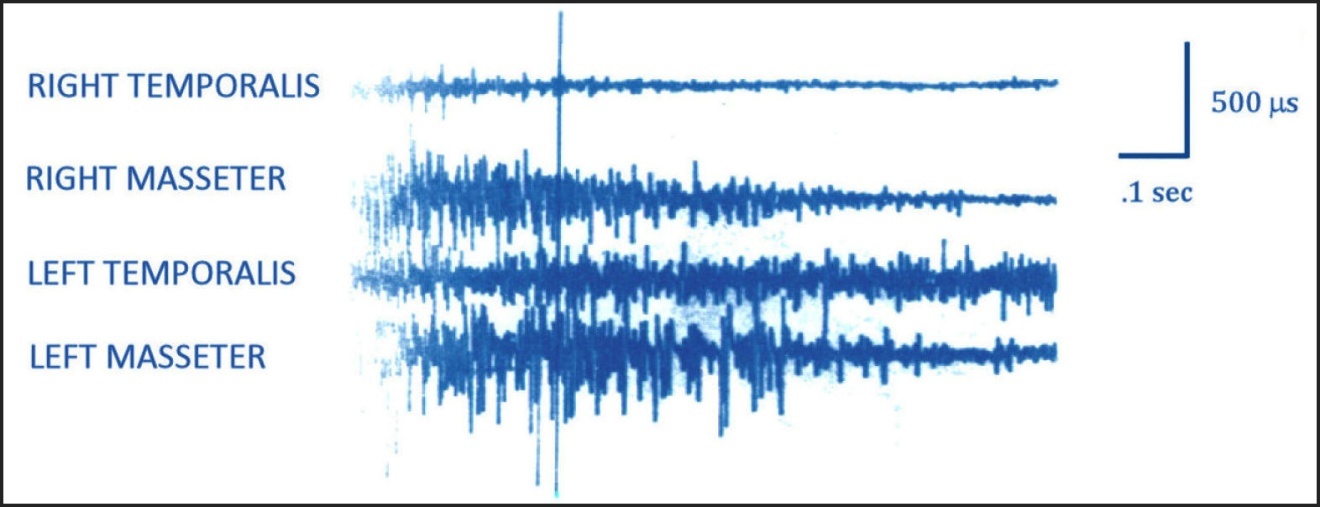
Much TMD occlusal treatment research was spawned from the excluded landmark anterior guidance study by Williamson and Lundquist, who first reported in 1983 on CPO’s muscle activity lessening effect (Figures 1 and 2).2
Then in the late 1980’s with T-Scan I (Tekscan Inc, S. Boston, MA, USA), the causal relationship between long Disclusion Time, high masticatory muscle firing, and chronic muscular TMD symptoms was discovered, and the ICAGD (Immediate Complete Anterior Guidance Development) time-measured coronoplasty was initially developed.3–12 That causal relationship was advanced in 2006 with the first T-Scan/EMG synchronization module (T-Scan III version 7/BioEMG III, Tekscan, Inc. S. Boston, MA; Bioresearch Assoc., Inc. Milwaukee, WI, USA)11–13 that has continuously been researched up to the present day with the T-Scan 10 Novus/BioEMG III synchronized occlusal and muscular technologies (Tekscan, Inc. Norwood MA, USA; Bioresearch Assoc., Inc. Milwaukee, WI, USA).14–54
METHODS
An independent literature search was undertaken using the key words" T-Scan/BioEMG", “T-Scan”, “Disclusion Time Reduction”, and “Canine Protected Occlusion.” PubMed listed 1626 English language publications for this search word combination (excluding duplicates) broken down by:
T-Scan AND BioEMG = 8
T-Scan = 661
Disclusion Time Reduction = 19
Disocclusion Time Reduction = 5
Canine Protected Occlusion = 1600
Note: Google Scholar listed 27,501 publications (12 times more than PubMed) for the same combination of search terms (non-English publications included):
T-Scan AND BioEMG = 311
T-Scan by Tekscan = 1,600
Disclusion Time Reduction therapy = 1,370
Disocclusion Time Reduction therapy = 1,120
Canine Protected Occlusion in dentistry = 23,200
Further, 3 separate T-Scan/Measured Digital Occlusion systematic reviews reported finding 100, 420, and 231 T-Scan research studies respectively.48–50 It is quite clear the Rinchuse et al did not perform anything approaching an “extensive literature search”; rather they performed a very biased selection of studies, reviews and commentaries upon which to base their conclusions.
“Canine Protected Occlusion (CPO) is neither the optimal or preferred functional occlusion in dentistry. The foundational principles of this concept are not supported by any biologic reasoning or scientific evidence. Furthermore, Canine Protected Occlusion (CPO) recordings fail to reflect or represent any type of physiologic mandibular motion and function or occlusal loading in humans.”
Rebuttal – The authors’ Results are based on outdated biomechanical occlusal concepts surrounding the macro-occlusal alignment of opposing coupled canines that can act as guidance surfaces when not impacted. This biomechanical thinking does not account for how posterior occlusal surface excursive friction impacts the neurophysiology of masticatory muscle hyperfunction.
The authors throughout this opinion paper completely ignored the biologic/neurologic CPO rationale described in all DTR treatment research studies,2–54 that is based upon the unique afferent dental peripheral neuroanatomy that the dental occlusion has within the Central Nervous System (CNS) and the dental occlusion’s extensive efferent outreach from the CNS to physically elevate masticatory and swallow mechanism muscle activity.55,56 By ignoring the occlusal surface friction neuro-occlusal physiology in their explanations for why CPO is unnecessary, and by excluding all the T-Scan/EMG and DTR muscle contraction lessening documentation over the past 4 decades, the authors purposefully censored the supportive biologic and neurologic reasoning to employ CPO as a desirable occlusal scheme.2–54
Lastly, CPO motions have been verified in 3 separate mastication, chewing smoothness, and jerk cost studies, whereby canine guided lateral excursions refined with short Disclusion Times improved mastication strength, duration, and motion mechanics in both TMD and Meniere’s Disease patients20,21,45 These studies are additional scientific evidence supporting the biologic reasoning that canine guided excursions are physiologic for optimal human jaw motion patterns.21,22,45
Conclusions
“The functional occlusion contacts that clinicians should focus on most are those in or close to maximum intercuspation. This perspective aims to discourage practitioners from undertaking unnecessary extensive and invasive procedures to establish Canine Protected Occlusion (CPO) in all patients, especially when this is not substantiated by evidence-based literature.”
Rebuttal – Drs. Rinchuse et al are misdirecting clinicians away from establishing CPO excursive function refined with short Disclusion Times when it is usually possible to achieve both skeletally and dentally. Although a stable MIP is important for patient comfort, human mastication is comprised of excursive movements that includes lateral motion, and not just occluding vertically up and down into MIP.21,22,45 Therefore when possible, dentists should strive to create CPO prosthetically or orthodontically to reduce high masticatory and swallow mechanism muscle firing that increases occlusal loads applied to teeth, the periodontium, dental implants, and both Temporomandibular joints.2–54
CPO Refined with Short Disclusion Time
Orthodontic and TMD treatment studies have shown that having visual Canine Protected Occlusion doesn’t ensure there is rapid posterior disclusion. An 89 subject Disclusion Time measurement study found that post orthodontic Class I Disclusion Times averaged 1.2 seconds, which is 2.5 times longer than the muscle lowering threshold of DT ≤ 0.5 seconds per excursion.4–10,14,15 Disclusion Times of ≤ 0.5 seconds/excursion must be adjusted into the existing occlusal scheme with the ICAGD coronoplasty4,9 to take advantage of the neuro-occlusal muscle contraction reducing effects that canine protection offers dental patients.
Therefore despite interocclusally restoring canine-canine contacts, or moving teeth to physically couple canine contacts in MIP, that anatomical orientation is incapable of discluding posterior teeth very close to the central fossa within a neurologically effective time frame.4,9,10,13–15 This clinical reality dictates that despite existing canine guidance surfaces being present, posterior teeth will maintain frictional excursive contacts very close to the central fossa that promote elevated muscle firing. In actuality, excursive movements initially operate as a bilateral group function for some time and distance before the anterior guidance surfaces can lift the posterior teeth apart.4–33
Rinchuse et al make note of this non-discluding aspect to early excursive movements in Challenges in recording functional occlusal contacts in clinical practice:
“Interestingly, the functional occlusion type can change several times when going from the first stage of the lateral movements to the extreme end of the lateral movements. As expected, there are a greater number of teeth contacting in the initial phase of laterotrusive movement than the later stages. CPO rarely occurs at the first stage. When canine guidance is found, it is typically at the later stage of lateral excursive movements”.1
Rinchuse et al infer that opposing posterior contacts must occur in the beginning of a lateral excursion. But when masticating, humans do not close all the way into MIP contact, such that opposing posterior teeth do not reach complete occlusion. Instead, the occlusal surfaces closely approximate each other to somewhat minimize the negative aspects of any existing friction near to MIP. Within a chewing cycle, any short duration light occlusal contact will produce a fleeting muscle shutdown (known as a Silent Period). Whereas a more forceful occlusal contact within the same chewing cycle will produce a longer Silent Period.57 Of significance is that in a group of dysfunctional chewers whose CPO was refined with ICAGD to lessen surface friction durations down to very short timing tolerances (DT < 0.5 seconds/excursion), markedly reduced number of Silent Periods were observed while subjects demonstrated improved mastication motion mechanics, strength and speed within 7 days after undergoing ICAGD.20
Moreover, these anti-CPO authors incorrectly classified MIP contacts as "functional contacts," suggesting that MIP contacts are involved in active chewing. However, bolus mastication that involves any tooth contact, whether in MIP or within excursions, are actually dysfunctional contacts. The purpose of mastication is to crush and grind food, but to not crush or grind teeth. When masticating, there is no "functional" reason for teeth to contact until the human is ready to stabilize the mandible for swallowing.57
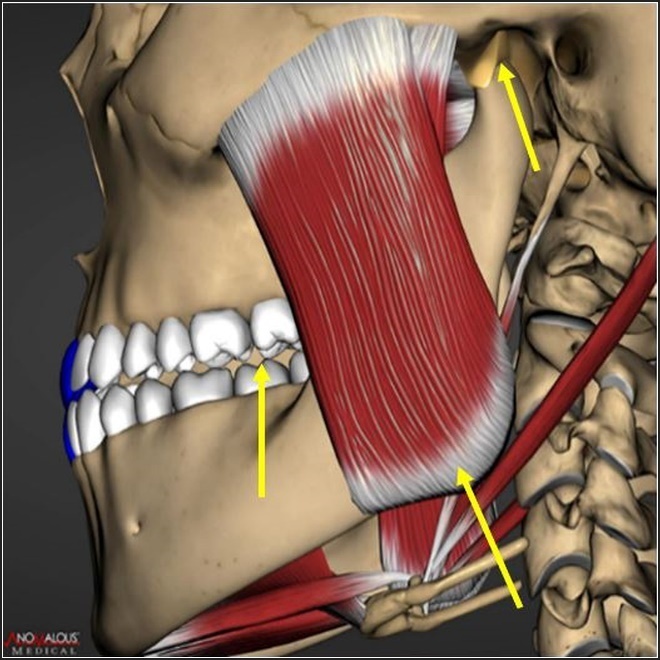
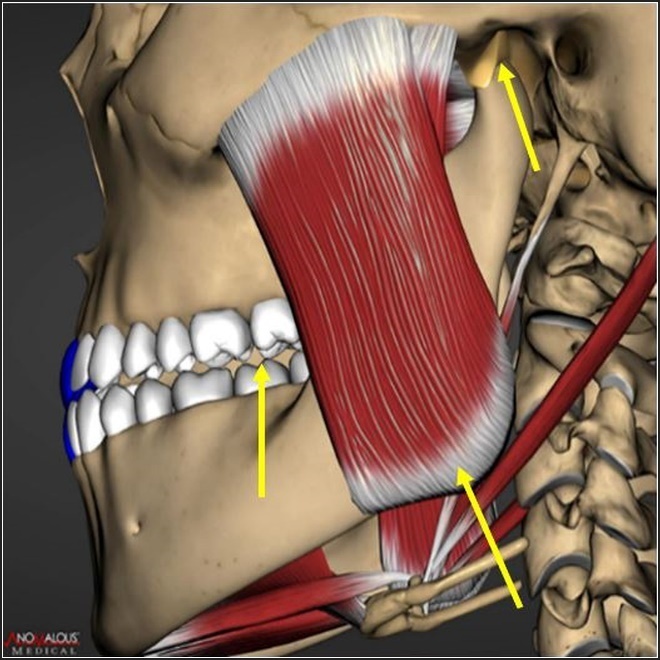
It’s important to explain why CPO anatomic alignment does not fully counter the occlusal surface friction that results during laterotrusive movements. Excursive friction results close to the central fossa because the working side condyle elevates antero-vertically into the soft articular disc when the working side lateral pterygoid contracts to participate in a laterotrusive movement (Figure 3). The disc is then compressed against the articular eminence while simultaneously, the back end of the mandible elevates the same distance upwards that the condyle elevates into the disc.
**_a_class_i_occluso-muscle_disorder_patient_in_the_mip_position_with_anatomically_ste.jpeg)
This inability of canine guidance lift to separate posterior teeth very early in excursive movements is why patients with visually contacting CPO surfaces can exhibit high excursive muscle firing,13–15 muscular TMD symptoms like clenching and grinding, facial pain and temporal headaches (Figure 4).8
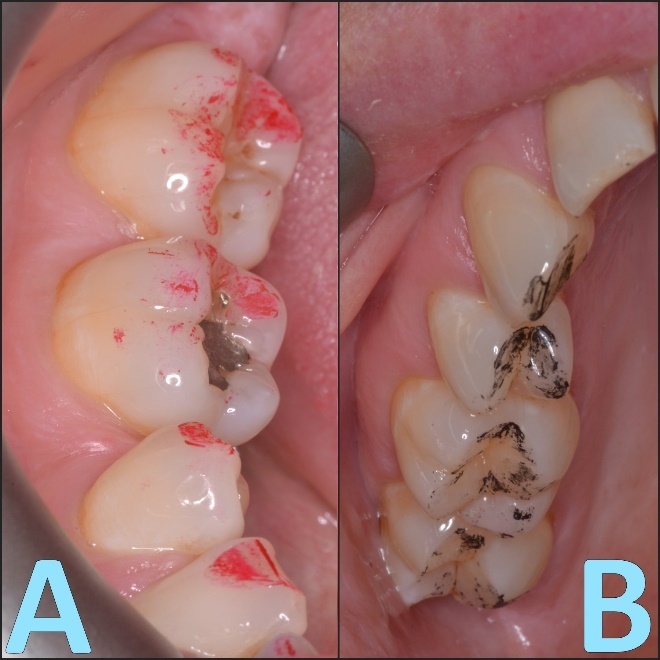
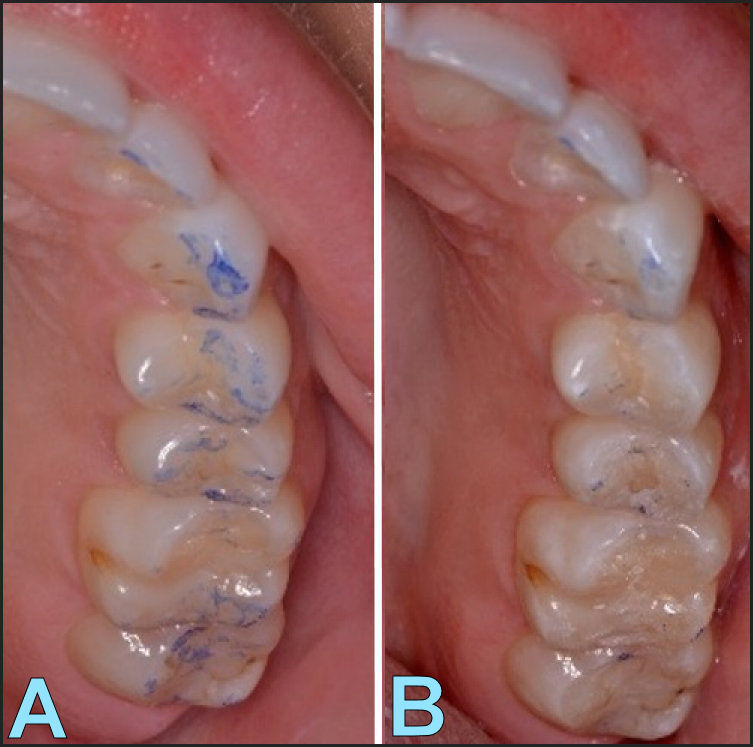
Examples of opposing posterior occlusal surface excursive friction can be seen in Figures 5A & B.
**_broad_red_buccal_and_lingual-to-lingual_excursive_ink_marks_visible_on_opposing_non.jpeg)
This excursive surface friction can hyperfunction the masticatory and swallow mechanism muscles,55 and must be machined out of the occlusal scheme with the ICAGD coronoplasty to lower muscle activities and optimize the neurologic advantages of a CPO occlusal design.4,9,15
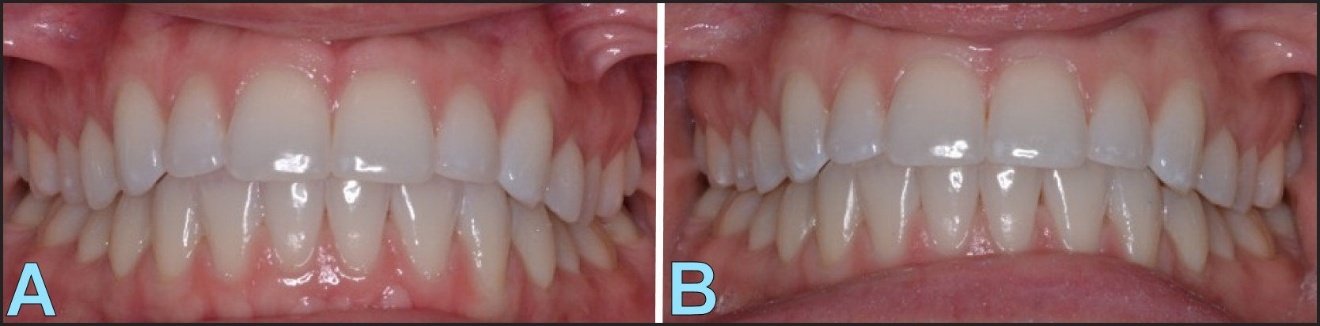
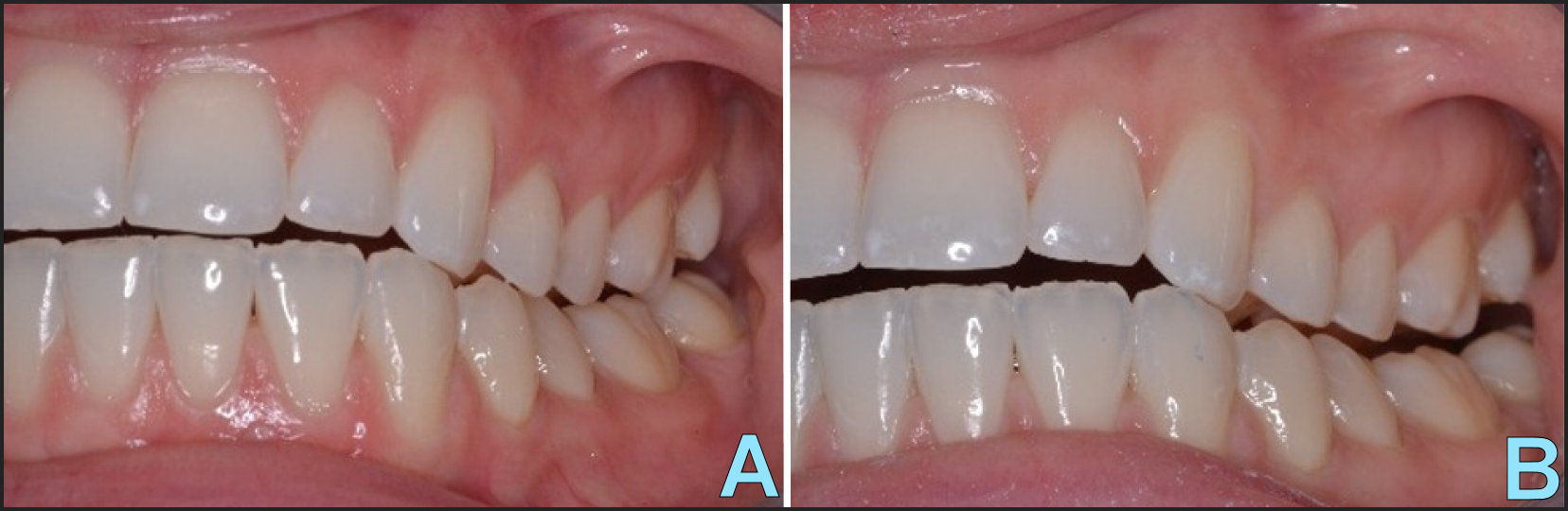
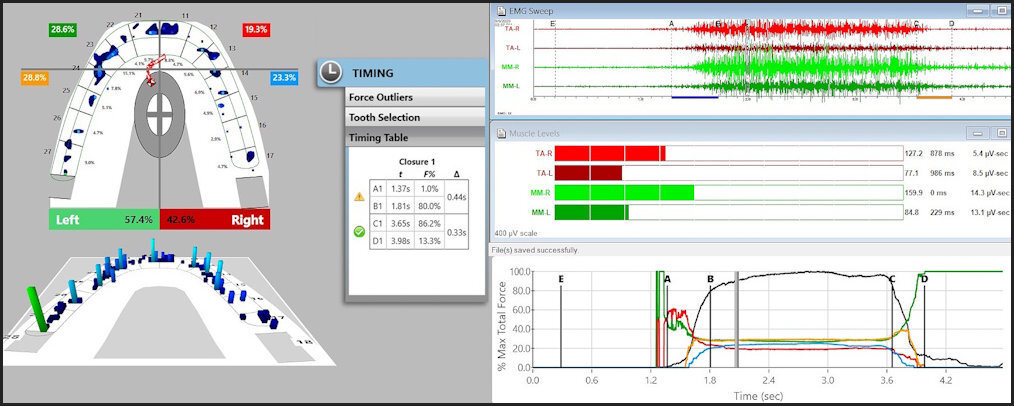
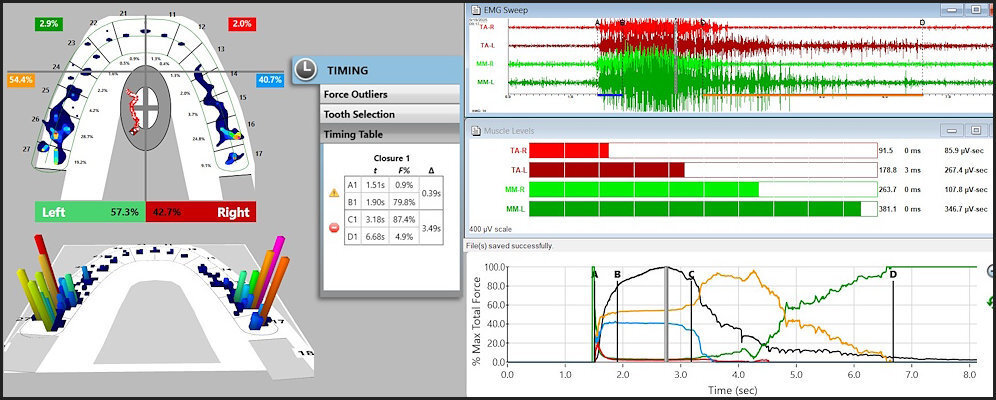
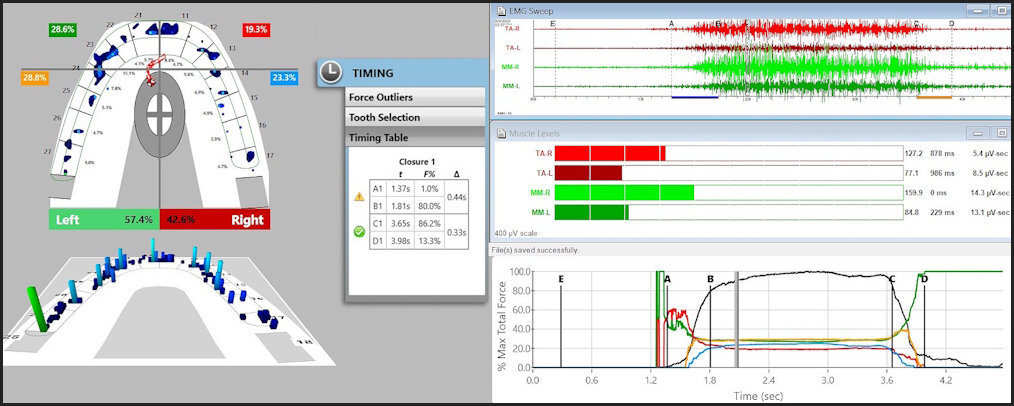
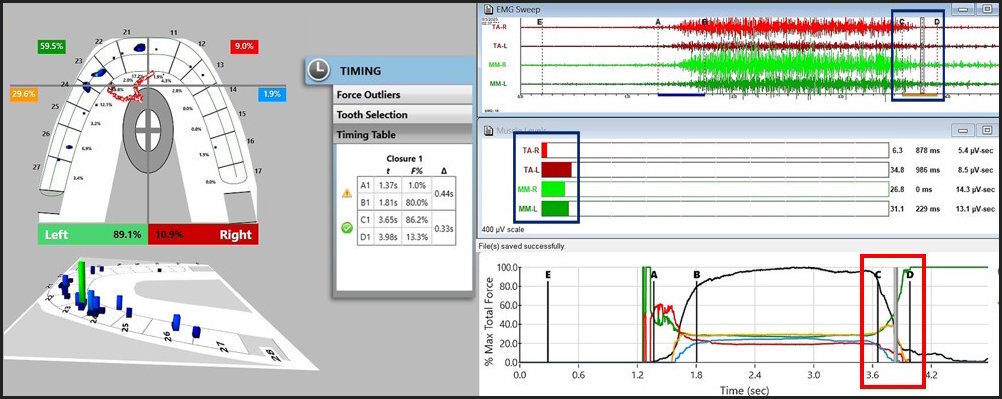
Figures 6-10 illustrate multiple paired views of a patient’s left excursion with anatomic CPO pre-ICAGD (left image) compared to the same patient’s post-ICAGD left excursion with the excursive friction removed (right image).
**_the_mip_anatomic_alignment_has_bilateral_canine_guidance_surfaces_in_place_that_can.jpeg)
**_despite_there_is_canine_contact_early_in_the_left_excursion__visible_buccal_excursi.jpg)
**_on_the_right_balancing_side__early_in_the_left_excursion__there_is_visible_excu.jpeg)
**_despite_the_cpo_guidance_track_visible_on_tooth__11__excursive_friction_articulatin.jpg)
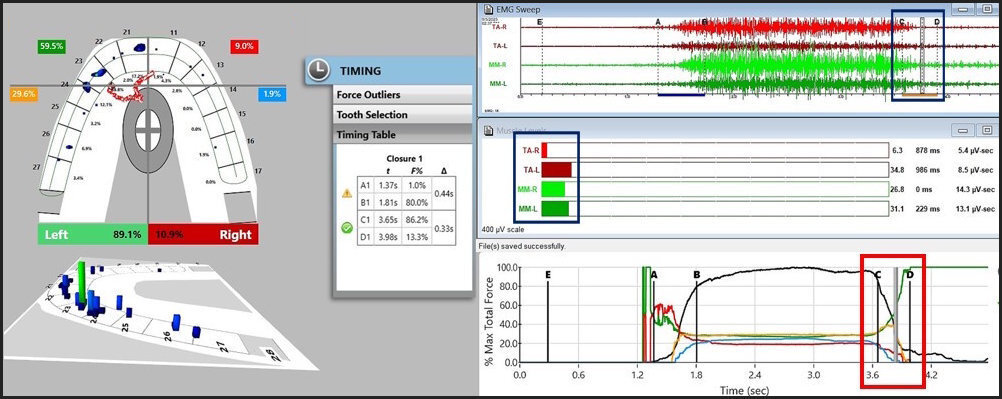
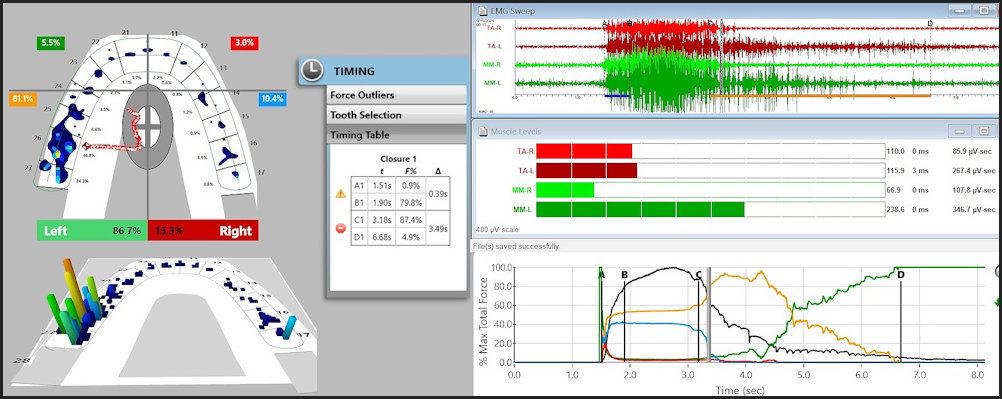
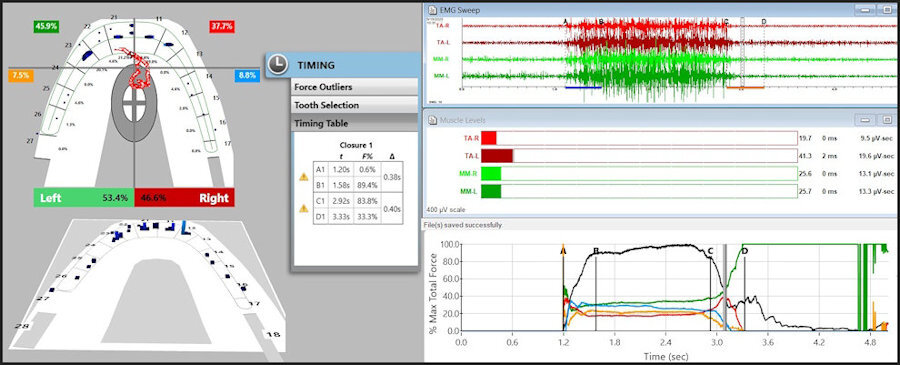
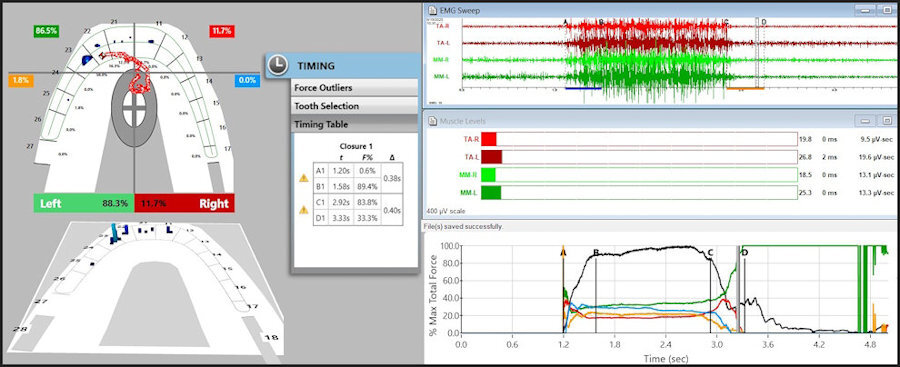
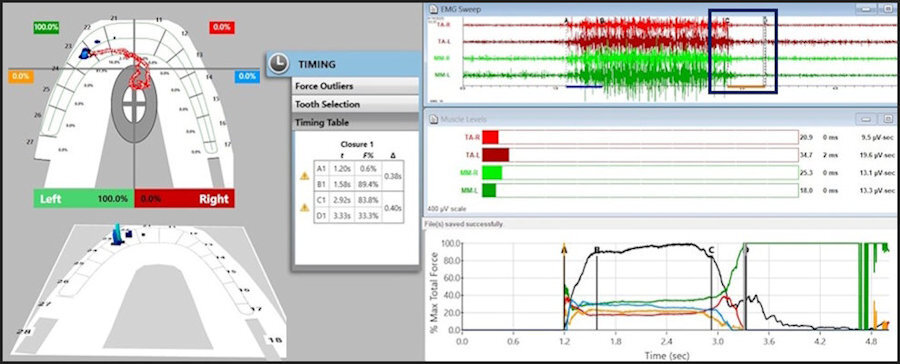
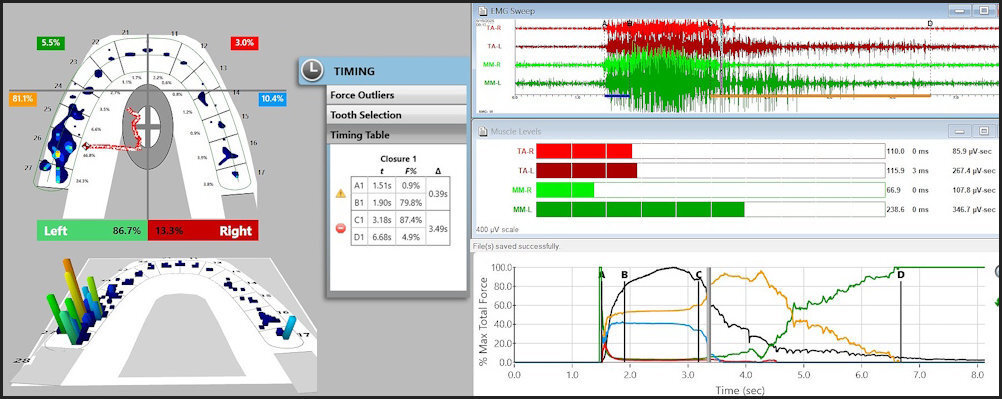
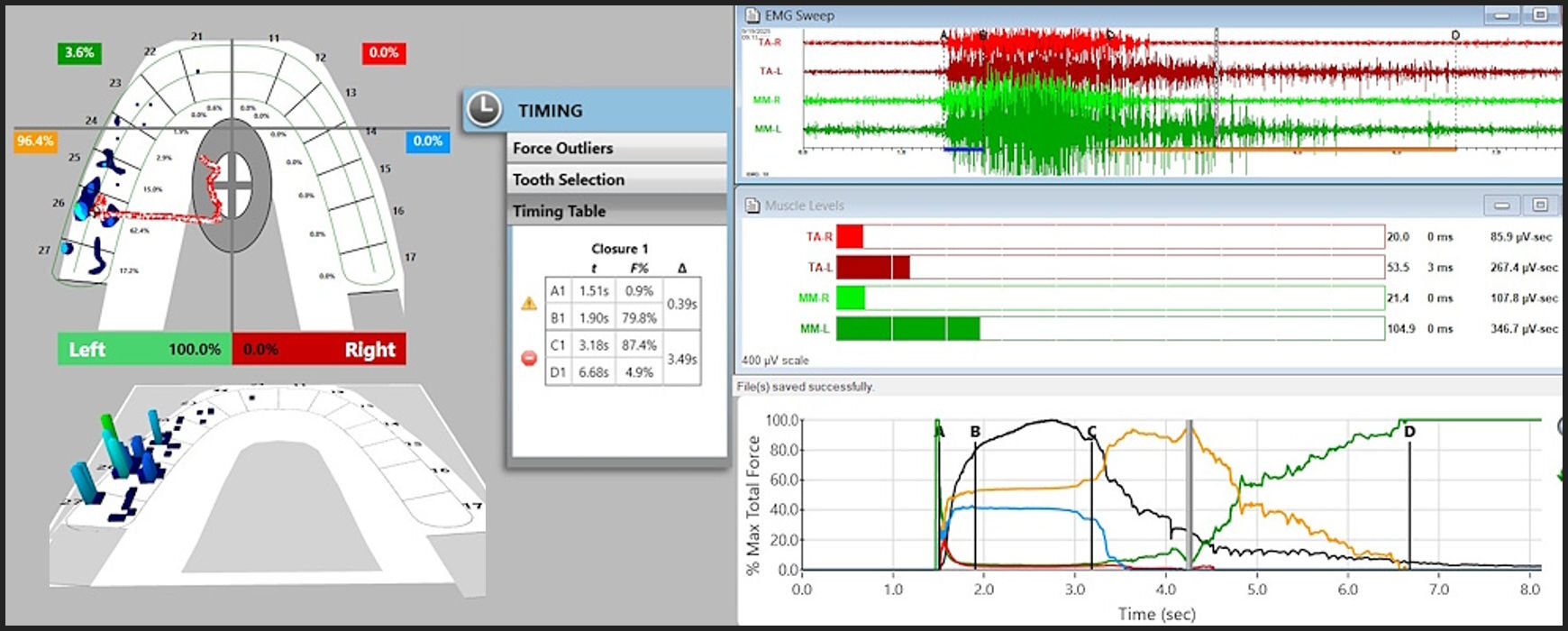
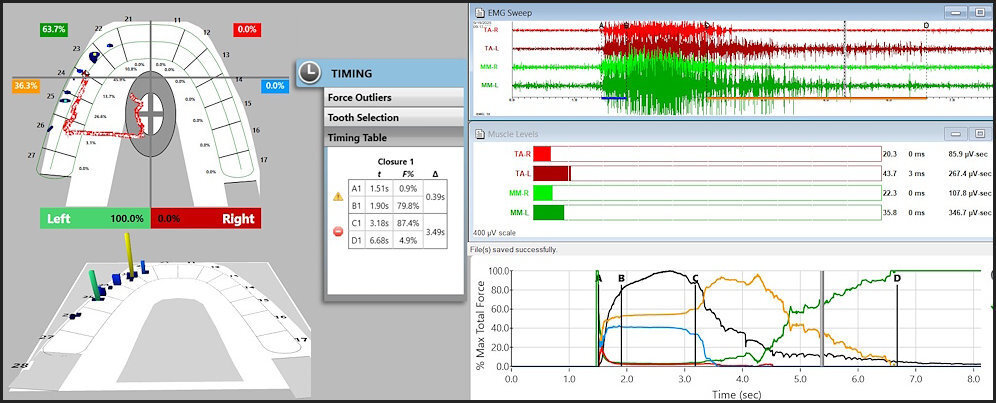
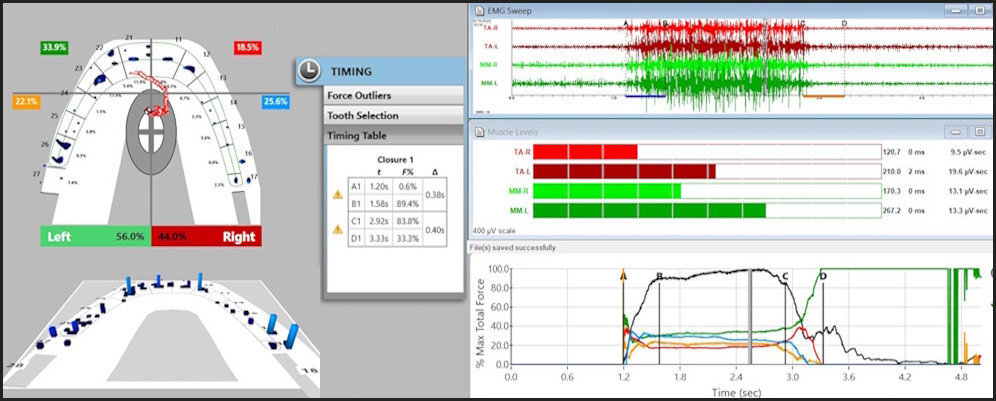
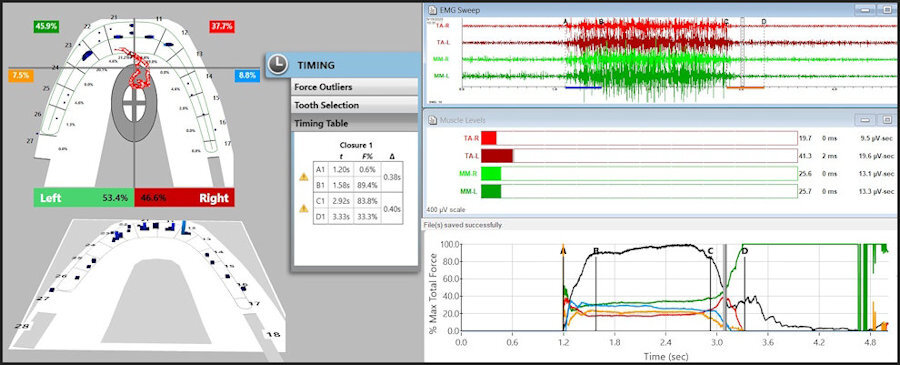
Comparing pre to post ICAGD, the same anatomic CPO surfaces rapidly separated all posterior teeth bilaterally and reduced the mid excursion muscle activity used to perform the left excursion (Figures 11 – 13).
Importantly, Canine Protected Occlusion (CPO) becomes neuromuscularly and physiologically optimized when ICAGD removes the excursive occlusal surface friction from all opposing molar and premolar occlusal surfaces (Figure 11 compared to Figure 13). The foundational scientific principle is that properly performed ICAGD drastically lessens afferent electrical input to the CNS, which directly reduces efferent output volume emanating from the Trigeminal Motor Nucleus into the masticatory and swallow mechanism musculature, drastically lowering functional muscle contraction levels close to baseline.4,14,15,55,56
The following sections will directly address each point proffered as “guidelines for clinicians to follow” within this anti-CPO opinion paper. Importantly, their incorrect and unscientific recommendations to discount CPO are far from being" patient-centered."
**_excursive_friction_articulating_paper_lines_are_visible_on_the_buccal_aspects_.jpeg)
Historical Background and Rationale for CPO
Despite the Historical Background stating D’Amico’s long root rationale for why canines are the desirable tooth to absorb lateral excursive forces, and that D’Amico himself believed muscle contractions turned off with canines in lateral contact, the authors purposefully left out any mention of CPO’s muscle activity levels lessening effect that was first illustrated Williamson and Lundquist in 1983,2 and then repeatedly documented by Kerstein’s early Disclusion Time Reduction research from 1989 to the early 2000s.3–11 These findings were then brought forward by other authors using the first T-Scan/EMG synchronization,12,13 that continued up to the present day with multiple differing authors replicating the original DTR studies and performing new ones that extend the breadth of DTR therapy’s proven clinical applications.14–54
Specifically, CPO combined with short Disclusion Time exploits the neuroanatomic anterior teeth function to limit muscle contractions because anterior teeth form within the Sympathetic Nervous System. This anterior tooth neurologic function is directly opposite that of the molar and premolar teeth that promote muscle contractions to masticate and swallow. The posterior teeth form within the Parasympathetic Nervous System and their pulp and PDL mechanoreceptors communicate directly with the brain’s Reticular Formation (Figure 14).55
**_general_somatic_afferent_nerve_pathway_(in_green)_from_molar_and_premolar_pulp_and.jpeg)
This section ends with the Rinchuse et al opining about “balancing and working contact severity” without providing any objective documentation that they have ever used the T-Scan technology, without ever including it in any of their multiple reviews and opinion papers, or having ever determined working and balancing contact force severities:
"…the CPO advocates also failed to consider that most of the studies that have dealt with functional occlusion and CPO (including Group Function and Balanced Occlusion) have not considered the severity of the contacts, i.e., notably, balancing contacts. That is, most studies merely looked at the number of contacts. To clarify, a balancing contact could range in severity from a very light and soft contact of the teeth to that of a deflective occlusal interference. Occlusal contacts are usually considered benign, while occlusal interferences are thought of as potentially pathologic. A balancing side occlusal contact is without incident, whilst an occlusal interference has been speculated to be potentially associated with clinical consequences (e.g., tooth mobility, tooth movement, fremitus, pulpitis, deflection of the mandible, alveolar bone loss, root resorption, intrusion of the teeth, tooth wear, tooth fracture) … In addition, Ash and Ramjford noted: “Lateral stress on the teeth is desirable within physiological limits; it stimulates the development of a strong fibrous periodontal attachment around the neck of the teeth.”1
Their opinions are not based on actual measured contact force “severities”, but on studies using ink marks and articulating paper, which cannot be correlated to “severity” in any way, regardless of how paper marks appear on teeth.58–61 More importantly, occlusal surface friction that elevates muscle activity as defined by Kerstein in the early T-Scan I and II Disclusion Time publications, encompasses both the time-durations and severities of all molar and premolar working side group function contacts (or interferences) and all molar and premolar balancing contact severities (or interferences).3–11 This is because the posterior pulpal and PDL mechanoreceptors do not neurologically differentiate working from balancing contacts. All opposing posterior occlusal contacts flex pulps and compress PDLs, which then directly within the CNS, fire the muscles that control masticating, and swallowing,55
Readers of this rebuttal should understand that the true physiologic impact of “balancing and working side contact severities” has been clarified because of the T-Scan 7/Bio EMG synchronized technologies (Tekscan Inc., S. Boston, MA; Bioresearch Assoc., Inc., Milwaukee, WI, USA). In 2012 by utilizing these 2 synchronized technologies, it was determined that working side group function contacts created the most muscle activity; far more than did balancing contacts.14 Therefore, working side group function contacts are far more problematic for teeth, muscles, and TM joints than are balancing contacts. Further, the outdated and pre-T-Scan opinions of Ash and Ramjford, intimating that lateral occlusal forces create “a strong fibrous periodontal attachment around the necks teeth” should be completely discounted.1 T-Scan/EMG research has determined that lateral stresses on teeth promote abfraction formation, gingival recession, and cold sensitive teeth.31,41
Lastly, an example of how these anti-CPO authors promote their incorrect beliefs as if they were "facts, is they make supposedly factual statements while misreporting the known facts, e.g., the below quote from their Historical Background:
“Occlusal factors have not been shown to be causative of bruxism. Bruxing is indeed a centrally-mediated phenomenon.”1
To supposedly support this false contention, the authors cited 11 papers, of which 5 were anatomic comparison studies attempting to find skeletal, anatomic, or occlusal biomechanical differences between bruxers and non-bruxers, reporting no anatomic or occlusal differences were found.1 This is quite similar to the findings of Seligman, Pullinger and Bush, who were unable to find any biomechanical occlusal causation of TMD symptoms by looking at surrogates of occlusion and not identifying the actual location and duration of occlusal contact.62,63 The other 6 papers were reviews (4), a consensus paper (1), and an argument paper (1), none of which included any published measured occlusion science.1 Importantly, Drs. Rinchuse et al provided no anatomic or statistical evidence that a region in the brain exists that generates bruxism behavior.1 Nor was there any discussion of the neuro-occlusal brain physiology that has been shown in multiple (excluded) DTR studies to contribute to bruxism behavior.5–7,55,56
Additionally, stating "Occlusal factors have not been shown to be causative of bruxism" is to state a complete falsehood. There exists multiple T-Scan/EMG and DTR studies, including a few RCTs, which have shown repeatedly that bruxism in TMDs patients has been reduced coincidentally with T-Scan/EMG occlusal treatment to shorten excursive Disclusion Times.6,7,20,25 Five long-term post ICAGD TMD follow up studies all reported that after initial ICAGD, bruxism episodes remained absent or at lower levels when subjects were reassessed at 1, 3, and 9 years.7,10,27–29 The theory that bruxism is centrally mediated lacks any definite evidence, but clearly teeth are bruxism causative and DTR has demonstrated predictably favorable treatment outcomes.
Challenges in recording functional occlusal contacts in clinical practice
The authors observations about the non-physiologic nature of lateral movements were made from non-biometric occlusal research, with visual inspection being their primary assessment tool:
"It is worth noting that these lateral movements are not natural or physiologic, but rather are guided by the operator and subject, raising questions about the validity of using such recordings to define functional occlusion "1
Once again, Rinchuse et al appear to misunderstand how excursive movements are properly performed by patients, and how they are repetitively, and accurately digitally recorded. All canine-guided pre-ICAGD T-Scan/EMG recordings are unguided by an operator, solely made by the patient self-occluding into MIP (with a T-Scan HD sensor interposed), then holding their teeth together for 1-3 seconds, and then excursing in 1 direction only (right, left, or protrusively).4,6,9,15,16,64 While the direction of the motion of the lateral excursion is reversed compared to the direction of masticatory function, the pathway is the same and very intimate with respect to the occlusion.
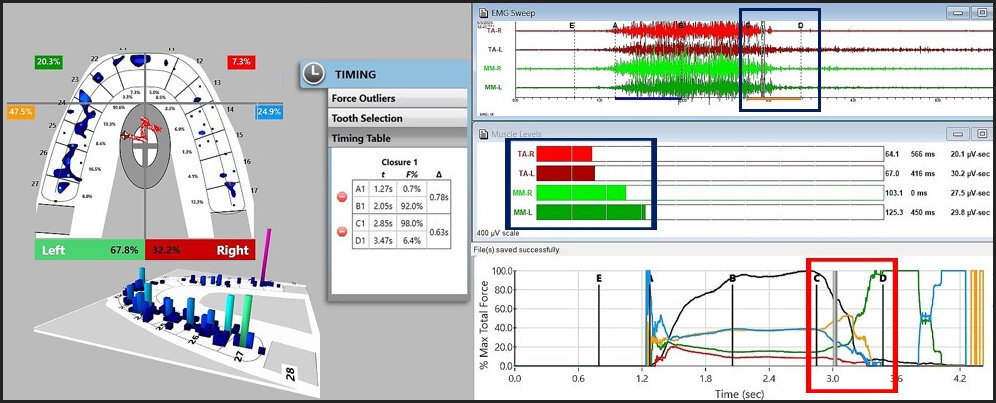
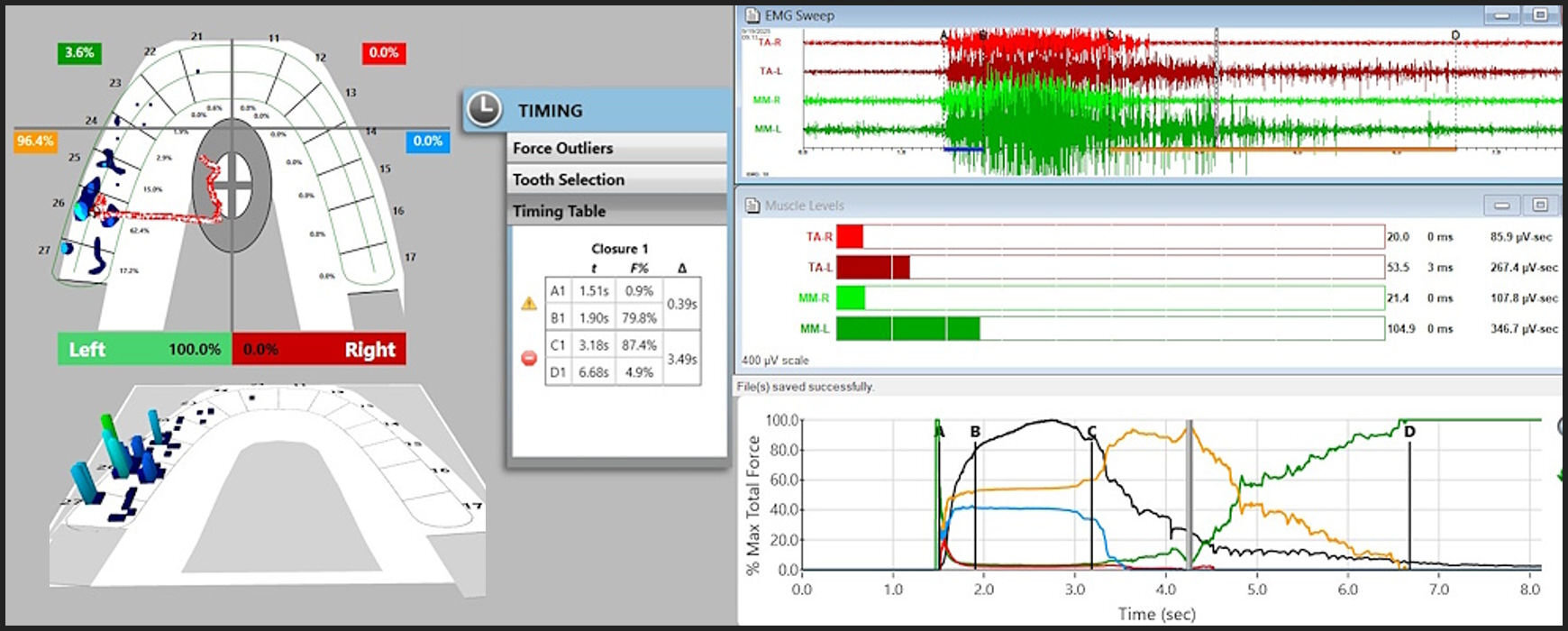
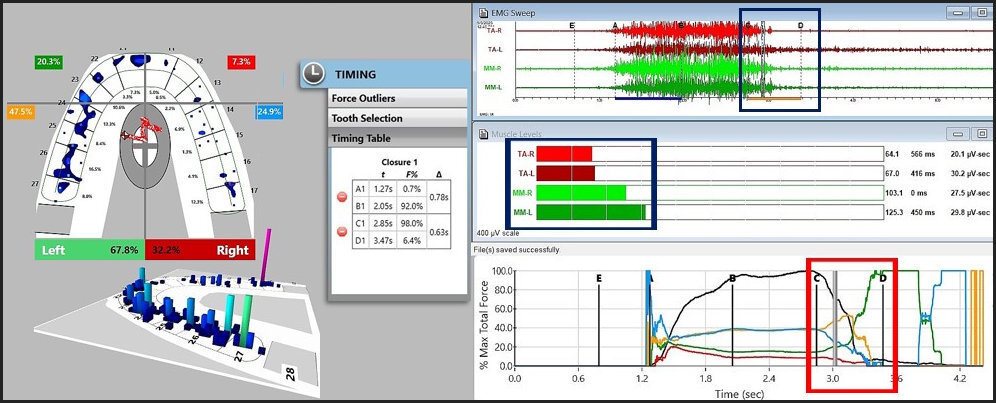
The T-Scan/EMG recordings of the excursive Disclusion Times capture the entire tooth contact transition continuum from commencement of the excursion into early group function and balancing contact time-durations, through to when complete posterior disclusion is achieved (Figure 15).4,6,9,15,16,65
**_in_mip__this_patient_appears_to_have__steep__left_canine_guidance_surfaces_that_sh.jpeg)
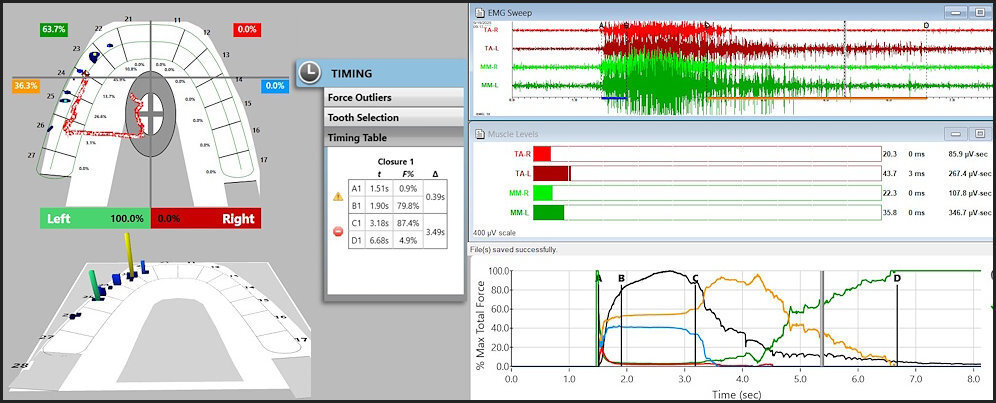
To fully understand the time durations of frictional contact transitions, one must sequentially view T-Scan/BioEMG excursive data at different time points within an excursive movement. The following figures (Figures 16 – 20) illustrate the key time-moment contact transitions within the continuum of the prior pictured left excursion (Figures 15ABC).
__prior_to_excur.jpg)
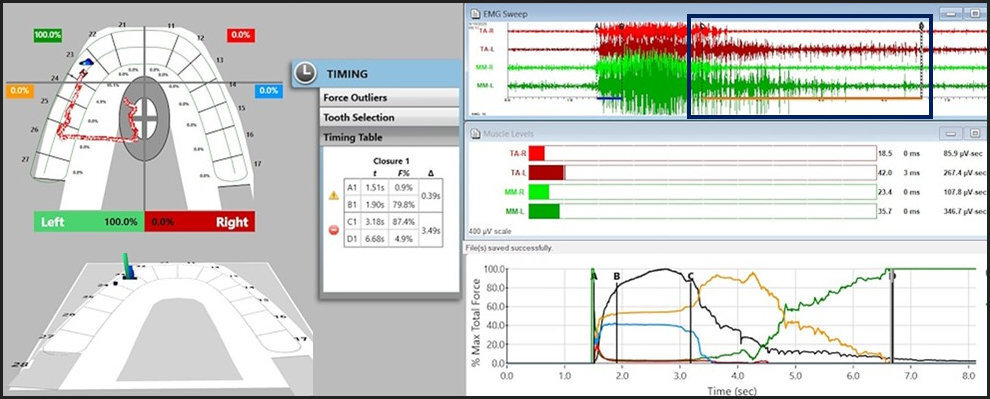
_finally_was_achieved_with_the_left_canine__23_.jpg)
Employing ICAGD, the time-durations that posterior teeth maintain excursive contact before the canine guidance takes excursive control can be markedly shortened, to give the canine guidance surfaces excursive control much faster than in the untreated pre-ICAGD condition.4,9 This physiologically reduces muscle activity because all posterior teeth quickly disengage, which directly stops flexing pulpal and PDL mechanoreceptors that in turn, lessens muscle contraction durations and volume (Figure 21).15
**_the_post_icagd_mip_appears_similar_to_the_pre_icagd_condition__except_that_the_lef.jpeg)
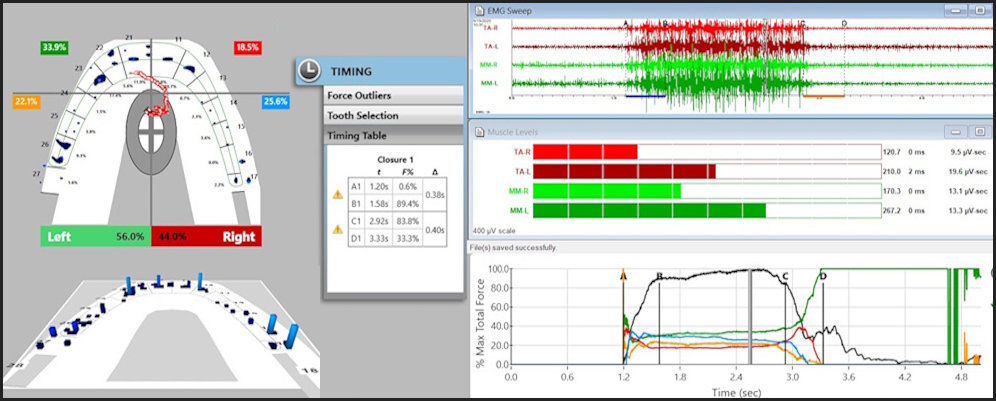
The post ICAGD frictional contact transitions within the continuum of the treated left excursion are markedly shorter time durations than in untreated conditions (Figures 22 - 25).
_almost_completely_controls_the_l.jpg)
_was_rapidly_achieved_with_the_left_canine_in_c.jpg)
Next, contrary to Rinchuse et al’s opinions, recording canine protective movements with the T-Scan/BioEMG is highly reproducible, and has been verified in many Disclusion Time Reduction studies.4–54 Although Rinchuse et al referenced a few T-Scan papers in their “recording challenge” section, pointing out “…these computer technologies used have their drawbacks,”1 these anti-CPO authors did not cite a single Disclusion time Reduction TMD treatment study, whereby different patient populations were repeatedly excursively recorded over multiple dates to gather pre and post ICAGD Disclusion Times. All DTR published studies have supported that CPO movements with both untreated Disclusion Times and shortened Disclusion Times were accurately and repeatedly recorded.4–54
In closing out this section, the authors question whether the amount of time teeth make contact actually matters, and point to studies that “estimated” the amount of daily time teeth are in contact. The CPO authors do not understand, “the amount of time teeth may make contact” results in frequent episodes of multiple muscles repeatedly contracting and electrically firing, creating and pooling lactic acid around muscle fibers “throughout the day.” Then again, the CPO authors blame “emotional bruxing” as a risk for pain instead of the frequently occlusally-activated electrical activity as the cause of painful muscular ischemia:
“Interestingly, it has been estimated that teeth only come into contact (swallowing and mastication) as little as 2 to 7 minutes to as high as 15 to 40 minutes per day (possibly 2–6 hours with added parafunction). Bracing, the activity of keeping the muscle tense without teeth contact, for instance, is indeed included in the spectrum of bruxism activities, being linked to emotional issues, and emerging as the most relevant risk factor for musculoskeletal pain. This information impacts upon the putative importance of any functional analysis in the etiology of pain and dysfunction.”1
Bracing is the act of posturing the mandible in an adaptive effort to avoid occlusal interferences, or to adapt to a compromised maxillo-mandibular mal-relationship. Although “bracing” requires a few microvolts of activity that arise from the smallest motor units, long duration, low level muscle firing can be as fatiguing for small motor units in the same way high level, short duration muscle contractions be for large motor units. Continuous bracing can lead to muscle pain and is most commonly seen in the temporalis muscles. Further, strong evidence exists that emotional issues are secondary to physically induced chronic pain.33,36,40
“In summary, one could ask, how does the length of time that teeth come into contact actually play into any considerations for a particular type of functional occlusion type? Should this information impact our clinical decisions? All factors considered, will they actually have any impact in the final functional occlusion in the long term? The answer is most likely no.”1
This is exactly where these authors are so neuro-occlusally incorrect about “the length of time teeth contact.” All the Disclusion Time Reduction treatment studies prove that “the time that teeth come into contact” actually has huge neurologic impacts on the dental occlusion, the supportive structures, and the muscles of mastication and swallowing.4–54 Contrary to the anti-CPO authors unfounded opinions, “the time that teeth come into contact” is an important long-term factor to consider when making clinical occlusal decisions.
Chewing Cycle Kinematics
In this section, the authors continue to mislead readers with their lack of neurologic understanding of how CPO effects muscle loading. They question whether force reduction is a part of CPO, using the word “unsubstantiated” to insinuate all the CPO and DTR research which illustrates muscle firing reductions, does not physically exist:
“There is the unsubstantiated belief that because CPO may reduce the horizontal forces on the posterior teeth, this can promote a more vertical chewing cycle…”1
Clearly, going back to Williamson and Lundquist in 1983, including all the T-Scan only, and all T-Scan/EMG and DTR treatment studies, a large volume of EMG data sets SUBSTANTIATES that CPO with short Disclusion Time dramatically reduces muscle force and hyperactive muscle firing durations.4–54
Rinchuse et al then confirm the importance of fitting teeth together into MIP involves the “gliding surfaces of the teeth,” yet they question if a particular occlusal scheme can influence all of the occlusal factors involved:
“What guides the mandible into maximum intercuspation is a combination of the underlying skeletal relationship (that sets the foundation from which the teeth are held in place) and the gliding surfaces of the teeth as well as the natural seating of the condyles within the fossae following opening and closing chewing movements… It would be naive and ingenuous to assume that all these factors are solely influenced once a particular functional occlusal scheme is achieved.”1
Despite the authors questioning whether an occlusal scheme can influence all factors involved in reaching MIP, CPO without the short Disclusion Time refinement consistently has an early group function component that does influence all factors in seating the mandible into MIP.20 This is because elevated muscle firing controls the mandibular pathways, the masticatory muscles (including the lateral pterygoid), and the swallow muscles neuroanatomically.55
Despite the authors’ statements that “canine protected motions are unnatural,” chewing studies utilizing electrognathography (jaw tracking technology) clearly demonstrate CPO motions are natural and occur as part of the chewing cycle.20,21,45 Specifically, dysfunctional patients with canine protection that had their disclusion times shortened demonstrated statistically improved chewing function, chewing strength, speed, smoothness, and motion patterns. These studies showed that the post ICAGD canine-guided chewing motions were very natural even for the dysfunctional chewers, compared to the group function or balanced occlusion the subjects presented with. These 3 mastication studies scientifically contradict the anti-CPO authors’ quite incorrect “unnatural” beliefs.20,21,45
CPO and Temporomandibular disorders (TMDs)
The authors repeatedly attempt to persuade readers to accept their unsupported theory that TMD is a psychosocial disorder with no occlusal foundation:
“The current approach to TMD management now involves taking into account brain neuroimaging, the genetics of pain vulnerability and pathophysiology, chronic musculoskeletal disorders, and behavioral and psychosocial factors.”1
Although the authors allude to TMJ symptom causation moving away from a traditional mechanical oral model to a behavioral and psychosocial model, no research from the psychosocial world exists that can counter the measured digital occlusal science on Disclusion Time Reduction. It’s been shown in psychological systematic reviews that it’s not possible to treat TMD effectively with Cognitive Behavioral Therapy, psychotherapy or with medicinal combinations thereof.64,66,67 Scientifically supportive emotional well-being studies (including an RCT) incorporating the Beck Depression Inventory II and the PHQ-15 have shown that treating the occlusion with CPO and the short Disclusion Time refinement, not only resolved physically painful TMDs, but also rapidly improved patient emotional states, and lessened stress levels measured by large, post ICAGD salivary cortisol reductions.15,33,36,51
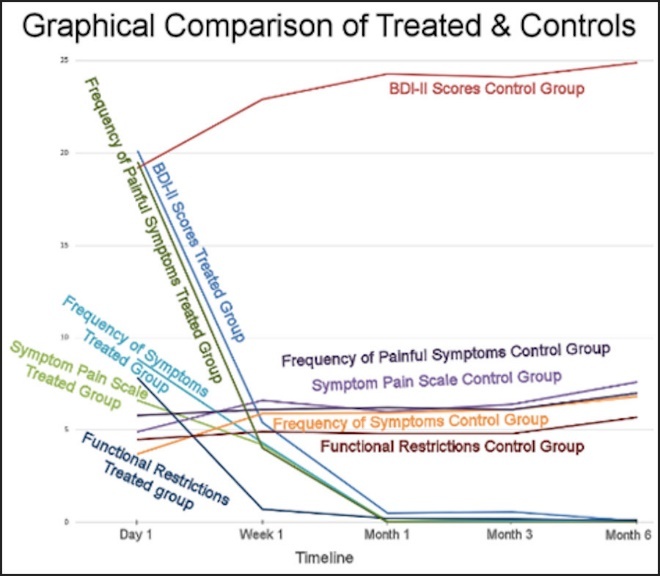
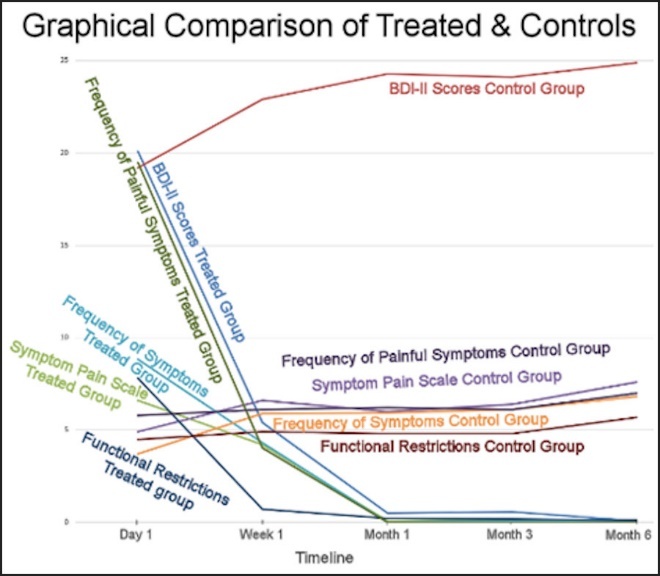
In a 100 subject Disclusion Time Reduction RCT, the 50 ICAGD treated participants’ muscular TMD symptoms statistically reduced dramatically to negligible at 6 months post-treatment, while the 50 control group subjects that received mock ICAGD reported their symptoms either increased or remained stable over the study duration (Figure 26).15 Further, the same 50 ICAGD treated subjects’ emotional well-being statistically improved, while the 50 controls that received mock ICAGD reported their levels of depression increased and other symptoms either increased or remained constant over the study duration, indicating that there was no placebo effect from mock ICAGD.15
Tooth wear
In this section, the authors continue to mislead readers with their lack of neurologic understanding of how CPO effects muscle loading and resultant tooth wear, questioning whether CPO is protective of tooth structure. The authors used the word “unsupported” to insinuate all the CPO and DTR published research which illustrate muscle firing reductions that lessen tooth overloading, has not actually been demonstrated.2,4–54 Rinchuse et al repeatedly substitute their own “unsupported beliefs” that multifactorial etiologies are at the core of many mechanical occlusal problems, primarily blaming bruxism and psychosocial factors for wear related dental pathologies:
“There is the unsupported belief that when the canine teeth are in CPO, they “protect” the posterior teeth from excessive occlusal forces and subsequent wear due to attrition. There are many factors that influence tooth wear such as age, diet, dental and facial skeletal characteristics, function and parafunction, and so on. Notably, most mechanical tooth wear is caused by attrition due to bruxism. Undeniably, the evidence does not support the notion that the lack of canine guidance is the underlying cause of tooth wear (or tooth fracture). Even if canine guidance is present or established, with attrition, tooth settling, growth and age-related changes over time, the final functional occlusion will most often be Group Function or Balanced Occlusion.”1
Undeniably, a lack of canine guidance definitively promotes excessive amounts of working and balancing occlusal surface excursive friction that can promote wear resultant from elevated muscle loads rubbing opposing teeth against each other. This will magnify any enamel damage as opposing occlusal surfaces cyclically frictionally engage during both mastication and parafunction.
And the observation that when CPO is present, often the functional occlusion is "Group Function or Balanced (which means bilateral group function with all posterior teeth frictionally involved in all excursive movements), is exactly why the Disclusion Time Reduction refinement with ICAGD is needed. As was pointed out in "Challenges in recording functional occlusal contacts in clinical practice," a group function always precedes any canine guidance providing posterior disclusion, when the condyle elevates into the soft disc under lateral pterygoid contraction (see Figures 16 – 20; Figures 22 – 24).
While it is true that when CPO exists anatomically in an occlusion, it does not stop wear from progressing unless it is refined with short Disclusion Time. Therefore, CPO has the potential to protect all the masticatory structures if the canine guidance is refined with short posterior Disclusion Times to reduce muscle activity levels.4,6,9,15,25 That is how all the benefits of CPO can be obtained from within the patient’s own neuro-occlusal physiology.
What’s interesting about this section is that the authors suggest that because group function is often the final occlusal scheme in a wear patient, it must be the “correct occlusal design”. When in actuality, group function self-perpetuates more wear because when canine guidance is lost, posterior teeth cannot be lifted apart to lessen the surface friction that over time, progresses the wear.
By itself, whether group function is “the final occlusal scheme”, does not justify that group function is desirable. Repeated DTR treatment studies indicate that group function is the worst occlusal design that can be provided to dental patients. It allows excursive friction to neurologically promote damaging muscular force applications to teeth, the TMJs, the supporting periodontal structures and to any occluding dental implants.4,6,9,15,16
An interesting periodontal index study reported that:
“teeth of mouths having canine-protected occlusions had significantly lower mean periodontal disease index scores than the teeth of mouths having progressive disclusion or group function. The canines and molars in the canine-protected group exhibited lower mean periodontal disease index scores than canines and molars in the progressive disclusion or group function categories.”68
These anti-CPO authors must be asked what their rationale is for embracing group function, when it elevates muscle activity that can damage teeth, cause gingival recession and abfraction, and promote occlusal wear?
Predominance
Certainly, the rebuttal authors confirms that no one occlusal scheme is observed in all dental patients:
“No single type of functional occlusion has been demonstrated to predominate in nature.”1
However, dental treatments in general should be designed to improve on nature where possible. Clearly, multiple excluded studies from the past 4 decades validate that a CPO refined with short Disclusion Time is a far less damaging occlusal scheme than group function or balanced occlusion. Therefore, clinicians performing occlusal design alterations should strive for a low muscle firing, non-damaging occlusion.
Smile esthetics
The authors once again show their neurologic occlusion ignorance regarding how CPO operates:
“In some cases, maxillary canine teeth are either extruded or their incisal edges are vertically restored with resin build ups, crowns, or veneers to establish CPO. When canines are extruded or restoratively built up (creating a vampire look) beyond their normal vertical position, the outcome would most likely be a non-consonant smile arc.”1
One can add length or height to worn canine incisal edges, or extrude canines orthodontically when attempting to steepen the exit angles and the lift of the anterior guidance surfaces. However, the anti-CPO authors do not realize that adding length/height incisally doesn’t affect the critical 1-3 mm distance the lower canine must travel against the upper canine palatal incline early in an excursion, during which the posterior teeth must be discluded bilaterally to stop the prolonged excursive friction from hyperfunctioning muscles.65
Leaving the existing CPO surfaces as is, and not unnecessarily extruding teeth or adding height/length incisally is acceptable to develop a CPO, as long as the canines are not overly worn or do not meet edge to edge. Then machining the friction out of the posterior excursive movements with ICAGD to shorten the Disclusion Times, using the existing 1-3 mm of upper canine palatal surface to lift the machined posteriors apart, is an effective and conservative way to optimize CPO, without compromising the natural smile curve (Figures 6 and 15A).
“The preferred esthetic smile design is a consonant smile arc where the incisal edges of the maxillary anterior teeth follow the lower lip curvature. A consonant smile arc is difficult to achieve with CPO. And, with age and/or parafunctional habits (bruxism), the canines will wear and the vertical height will be reduced, leading to Group Function or Balanced Occlusion.”1
The authors are completely misguided here perhaps because none of them has ever produced a CPO with an esthetically pleasing smile. A CPO can easily fit into a consonant smile because DTR optimization of CPO requires no anatomical canine alterations be made to reasonably intact maxillary canines. Further, when needed, bonding in guidance steepness, length, or creating canine-canine contacts when pre-treatment they are non-existent, can anatomically work with posterior ICAGD adjustments to create a low muscle firing, rapidly discluding occlusal scheme.69,70
Static occlusion versus functional occlusion
In the below discussion the author’s take a similar stance with respect to what mostly occurs in dynamic occlusion, regardless of the biomechanical anatomic inter-arch relationships. Group function or balanced occlusion (bilateral group function) apparently results even when canine guidance surfaces engage, such as in Angle’s Class I or II. As previously detailed in "Challenges in recording functional occlusal contacts in clinical practice" this occurs in all excursions because condylar elevation into the disc after excursive commencement out of MIP is followed by a time-duration of posterior group function that always precedes the anterior guidance lifting teeth apart:
“… Incidentally, when there is only canine contact on the working side, there is a greater probability for the lack of balancing-side contacts. Class I (and normal) occlusions most often exhibit Balanced Occlusion or Group Function Occlusion. A Class III relationship will have Balanced Occlusion or Group Function Occlusion…”1
Contrary to the authors opinions, when CPO has been refined with short Disclusion Times, rapid posterior disclusion dynamically occurs within a microscopic time duration (in ≤ 0.5 seconds/excursion).4,9,10,14,15,25 This markedly diminishes any period of posterior group function (or balanced bilateral group function), also reducing muscle contractions required to execute the excursive movement, while muscularly unloading all dental and supportive structures.
Considerations for the Clinician
Although a stable MIP is important for patient comfort, human mastication is comprised of excursive movements, as no human masticates by “biting up and down into MIP.”20,21,45 The authors are misdirecting clinicians away from attempting to establish CPO excursive function when possible both skeletally and dentally, incorrectly stating that a sound MIP will result in a good foundation for function. However, human “functioning” requires repeatedly moving laterally into and out of a position very close to but not touching MIP to chew. MIP is only used to swallow the bolus:
“Clinicians should always strive to achieve an optimal static occlusion as established by Angle and Andrews. Either prosthodontically or orthodontically, establishing a sound static occlusion should be the primary foundation goal from which other occlusal objectives are built upon. A proper static occlusion can best lead to an optimal functional occlusion.”1
Then Rinchuse et al state that contacts should be “differentiated” by force levels and severities for their “harshness, modifying occlusal changes over time,” yet provide no means to do that with any clinical accuracy or reliability.
“Next, and for the most part, the functional occlusion contacts that are at or closest to maximum intercuspation are generally the most important. Functional contacts should be differentiated and segregated based upon the extent of the contact, i.e., these can range from that of light and non-detrimental, to harsh and potentially harmful occlusal interferences. Consideration should be given to addressing these obvious occlusal interferences during treatment as well as how the occlusion will change with time.”1
Without the T-Scan 10 technology, the suggestion to “differentiate harsh from light force contacts” is not possible, nor is it possible to define the “obviousness of interferences.” Because Rinchuse et al have resisted all occlusal measurement technologies and have clearly advocated for outdated methods to analyze or treat the occlusion, the TM joint, and any existing muscular pathologies,71–73 the authors are advocating the use of ink, paper, shim stock and visual occlusal observations as their tools to “differentiate” contacts. Eight different studies clearly supported the subjectivity of the paper, ink and visual assessment methodology, as a completely inaccurate way to perform occlusal adjustments and won’t predictably change “harshness” to “lightness.”58–61,73–77
“Clinicians should not try to reconstruct patients’ occlusions to a preconceived notion of what constitutes an optimal functional occlusion. That is, it would seem prudent, and when at all possible, for clinicians to try to work with the type of functional occlusion the patient presents with or is leaning toward.”1
Lastly, the authors promote their idea of “accepting the occlusion the patient presents with” as the best approach to manage their occlusal presentation. That seems foolhardy at best when a patient arrives with recession, abfraction, wear, iatrogenic malocclusion,78 and chronic TMD symptoms from poor posterior disclusion elevating muscle loads in an ongoing way, while perpetually damaging teeth, TM joints, and their periodontal supportive structures. No amount of MIP adjusting to “theoretically optimize foundational contacts” with ink and paper can control those damaging occlusal elements from continually injuring a patient’s functional capabilities. Whereas multiple patient treatment studies not included in this Rinchuse et al opinion paper, clearly indicate that only with measured, computer-guided force and timing modifications of both closure into MIP contacts and drastically shortening the time-durations of frictional excursive contacts that are lifted apart by canine guidance surfaces, can muscle loads be diminished and optimum occlusal function be predictably obtained.4–54
What is the Rinchuse et al motivation to dissuade dentists from improving muscle physiology, and lessening applied occlusal loads?
The reason these authors should be vigorously questioned as to what their motivations were for feeling they should make misguided recommendations to reader dentists, when they specifically chose to ignore all the critical CPO with DTR research findings, is because that published science calls into question this opinion paper’s criticisms of CPO and the authors’ guidelines.2–54
The authors making these comments, do not want to recognize that better patient care comes with measuring the occlusion objectively using technology.54,55 It is disturbing that these authors making these misguided CPO recommendations to dental clinicians, not only negatively impact dental patient well-being, but also greatly diminish clinician occlusal effectiveness. To date, Rinchuse et al’s non-biometric, outdated, biomechanical approach and methods have no scientific support for the resolution of any occlusal maladies, while they continuously blame bruxism and patient psychological states as causative for chronic physical maladies.1,71–73 And yet, the direct occlusal approach that treats neurologically from within the Central Nervous system using a CPO occlusal design refined with short Disclusion Time, has found solutions for many chronic occlusal conditions without any psychological interventions, splints, appliances, Botox-A, physical therapy, or TENS.3–54
Final Recommendation
Readers of this biased opinion paper should completely dismiss Rinchuse et al as having no scientific basis in their occlusal guidelines. Instead, readers should undertake education into Measured Digital Occlusion that is practiced with biometrically-determined occlusal analyses, and direct high-precision occlusal therapy that requires establishing canine guidance surfaces and short Disclusion Times. Together, these 2 occlusal design approaches highly optimize the neurophysiology of human masticatory function, while protecting teeth and implants, the Temporomandibular joints, and the periodontal structures from sustaining chronic muscle force overload.
Disclosure
Mr. John Radke is the Chairman of the Board of Directors for BioResearch Associates, Inc., Milwaukee, WI, USA. The other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding{#fund}
No funding of any kind was received to support the research and writing of this rebuttal.